











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Mexico is home to almost 23,314 species of vascular plants (Villaseñor 2016), and at least 2,140 of them have been used for medicinal purposes (Caballero & Cortes 2001). Therefore, there is an extensive collection of traditional knowledge about the use of this medicinal flora, as shown by the scientific literature on ethnofloristic lists (Valdés-Cobos 2013, Méndez-González et al. 2014), quantitative ethnobotany (Heinrich et al. 1998, Sánchez-González et al. 2008, Canales-Martínez et al. 2005, Magaña-Alejandro et al. 2010, Alonso-Castro et al. 2012, Méndez-González et al. 2014, Can-Ortíz et al. 2017) and ethnopharmacology (Giovannini & Heinrich 2009, Juárez-Vázquez et al. 2013, Nambo-Camacho 2015, García-Hernández et al. 2015, Geck et al. 2017).
Oaxaca, with 10,229 species, is the Mexican state with the greatest floristic (Villaseñor 2016) and cultural (Caballero et al. 2004, de Ávila 2004) diversity. Mixteca is an interesting region in Oaxaca state due to its contrasts between high biological and cultural diversity along with high degrees of poverty, marginalization, deforestation, and edaphic erosion (Flores 2009, Palacio-Prieto et al. 2016). This region is characterized by the prevalence of indigenous people, where the health services provided by the government do not have broad coverage and present irregularities in the availability of medical staff and medication (OPS 2014). Therefore, resorting to the use of plants to address health problems is a common option among Mixtecan inhabitants, and 145 plant species have been reported with medicinal uses in the region (Caballero & Cortes 2001). Knowledge associated with the medicinal uses of this local flora is part of the community’s biocultural heritage (Palacio-Prieto et al. 2016).
Although there have been ethnobotanical studies focused on medicinal plants in the Mixteca region, most have been descriptive and qualitative studies. These studies have usually provided lists of plants and their uses (Pacheco-Hernández 2013, Pacheco et al. 2009, Nambo-Camacho 2015, Martínez-Cortés et al. 2017) and sometimes they have carried out comparisons between communities of the same (Ferrer-Pérez 2009, Nieto 2009, Hernández-Cruz 2013, Valdés-Cobos 2013) or different ethnic groups (Giovannini & Heinrich 2009). Other studies have focused on aspects of the traditional medical system that influence the choice of medicinal plants, such as the hot-cold humoral concept (García-Hernández et al. 2015).
The way in which plants are selected by peasant communities has been studied from cultural approaches through the use of ethnobotanical indices, which evaluate the value of use and the consensus in its use (Hoffman & Gallaher 2007, Reyes-García et al. 2007, Zenderland et al. 2019), as well as the hot-cold properties of the species. Likewise, ecological hypotheses have been proposed, such as those discussed by Gaoue et al. (2017), which state that the selection of medicinal plants by peasant communities is the result of their availability, both in the wild and in managed systems (Albuquerque 2006, Voeks 2004), as well as the versatility of the introduced species to be used. as medicinal plants (Alencar et al. 2010, Bennett & Prance 2000).
The versatility hypothesis assumes that some species were originally introduced into a community for food or ornamental purposes; later, the inhabitants gave them medicinal uses (Alencar et al. 2010, Ceuterick et al. 2008, Bennett & Prance 2000). Thus, among medicinal plants from a community, there may be a greater proportion of introduced plants than native plants. Versatility becomes a positive selection factor that increases knowledge, uses, and access to useful species. Thus, a more cosmopolitan plant will be more versatile since it will have additional uses in the new region where it was introduced. This hypothesis can be evaluated by comparing the number of uses between native and introduced species. The use value (UV) can be an index to estimate the versatility of a medicinal species according to Gaoue et al. (2017) and Zenderland et al. (2019).
The availability hypothesis assumes that the selection of medicinal species has to do with access to them (physical distance from the community and collection zone) or their local abundance in areas where people obtain the plants. The presence of anthropogenic environments (milpas, home garden, and disturbed forest), where introduced species grow and are collected, becomes relevant since they can be reservoirs providing plants for medicinal uses, where many of them could be introduced to the community. Testing this hypothesis requires knowing the environments where people indicate that they obtain plants for medicinal use and associating the local abundance or quantity of species with each environment, natural or anthropocentric (Albuquerque 2006, Gavin 2009, Stepp & Moerman 2001, Voeks 2004).
The therapeutic concept of hot-cold properties is a fundamental part of traditional medicine in Mesoamerica. Although it came from European humoral theory (Galen 1561, Foster 1984, 1986, 1987, 1988), it was influenced by medical Mesoamerican beliefs by incorporation of the principle of binary opposition. Mesoamerican therapeutics have evolved since colonial times by the incorporation of European medicinal practices (Foster 1987, López-Austin 1980, Manderson 1987, Messer 1987, Tedlock 1987, Jackson 2001, García-Hernández et al. 2015, Geck et al. 2017). This conception is based on the plant-disease relationship, involves selecting a medicinal plant, balancing the healthy human body between a hot and cold state, and applying remedies with the opposite property to the disease (Foster 1986, Toledo 2003). An imbalance in the plant-disease relationship results in a disease. The selection of a plant with hot or cold properties can be determined by its organoleptic characteristics or the healer’s experience and sensory perception (García-Hernández et al. 2015, Geck et al. 2017).
In this study, we recorded the richness of medicinal plants and the therapeutics associated with them in two peasant communities in Oaxaca, Mexico. Both communities belong to the Mixtec ethnicity and employ plants for health care as a common practice, which include native and introduced species to Mexico. These medicinal plants can be obtained from surrounding forests, but others are maintained in anthropocentric systems such as home gardens where native and introduced species coexist. We attempt to test the versatility and availability hypotheses based on the selection of plants for medicinal use in both communities. In the versatility hypothesis, we assume that there will be a higher percentage of introduced species with medicinal uses than native species and that UV indices (an estimate of versatility species) will be higher for introduced plants. For the availability hypothesis, we assume that most medicinal plants will be obtained from anthropogenic systems such as home gardens (where native and introduced species are cultivated) in comparison with a natural system such as the forest.
Materials and methods
Study area. The study was conducted in two communities in the Mixteca Alta region, Oaxaca, Mexico (Figure 1). First, San Andrés Nuxiño (SAN) is located at 17° 14' 13.5’’ - 17° 14’ 37.5’’ N and 97° 06' 14.3’’ - 97° 6’ 39’’ W, at 1,840 m. The other community, San Pedro Topiltepec (SPT), is located at 17° 25’ 57.3’’ - 17° 26’ 24.4’’ N and 97° 20’ 12.7’’ - 97° 21’ 11.1’’ W, at 2,160 m. For health care, people from both communities have access to free medicinal service in a health center on the weekends (SAN) or in a rural clinic with a doctor and nurse who serve from Monday to Friday (SPT). In emergencies, people travel to the district seat, Asunción Nochixtlán, to be treated at a health clinic, where medicine is frequently unavailable. The most common diseases in SAN are flu, pharyngitis, gastroenteritis, diabetes, and hypertension, while in SPT, they are tonsillitis, pharyngitis, gastroenteritis, conjunctivitis, diabetes, hypertension and chronic degenerative diseases (SSA 2020). Table 1 summarizes the demographic aspects for both communities, including the main economic activities that they pursue. The closest meteorological station in the study area (Station 20159, San Pedro y San Pablo Teposcolula) reports a temperate subhumid climate, with summer rains, an annual average temperature of 15.4 °C, and an annual precipitation of 723.2 mm; the main natural vegetation is pine-oak forest (García-Mendoza et al. 2004). We observed in both communities four socioecological systems where people obtain medicinal plants: 1) home garden where medicinal plants are cultivated for direct consumption; 2) community forest, Piedra de Troje communal reserve in SAN (60-minute walk away) and Yusacodo communal reserve in SPT (45 minute walk away); 3) pathways in the community; and 4) milpa, where medicinal herbs can grow alongside corn and bean crops.
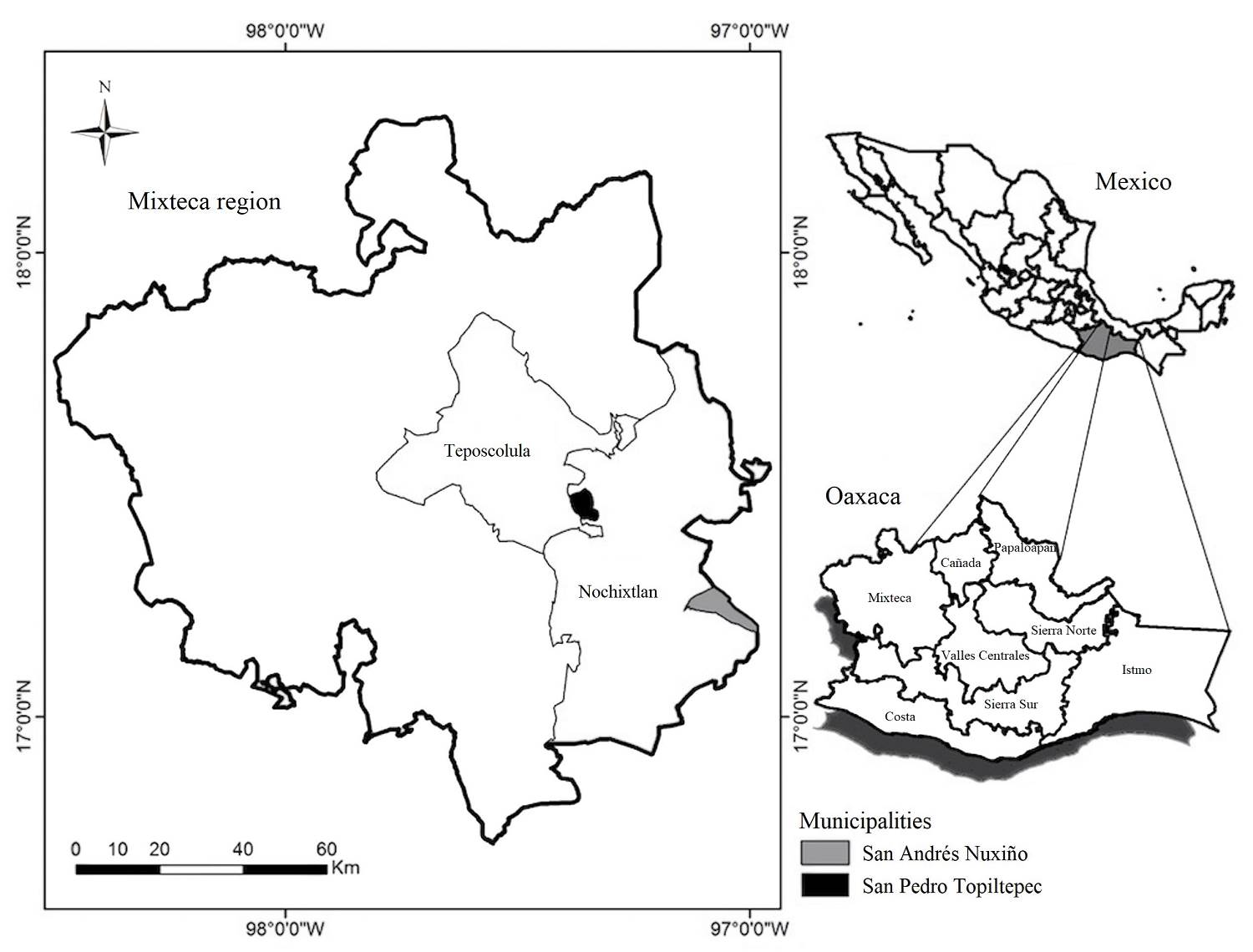
Figure 1 Geographic location of the study area, San Pedro Topiltepec and San Andrés Nuxiño, in the Mixteca Alta in Oaxaca, Mexico.
Table 1 Summary of sociodemographic parameters of San Andrés Nuxiño (SAN) and San Pedro Topiltepec (SPT), Mixteca Alta of Oaxaca, México, according to INEGI (2020).
| Parameter | SAN | SPT |
|---|---|---|
| Inhabitants in municipality | 1,850 | 373 |
| Inhabitants in municipal seat | 123 | 179 |
| Number of households in municipality | 587 | 131 |
| Number of households in municipal seat | 62 | 60 |
| Formal education average (years) | 6.6 | 5.8 |
| Inhabitants speaking indigenous language (%) | 43 | 1.97 |
| Household in conditions of poverty (%) | 92.64 | 92.60 |
| Household with provision of basic services (%) | 98.24 | 72.67 |
| Household with land floor (%) | 5.62 | 8.40 |
| Household lacking electricity (%) | 1.87 | 0.76 |
| Household lacking drainage (%) | 93.36 | 7.63 |
| Household using coal and firewood as fuel (%) | 82.73 | 40 |
| Household lacking social security (%) | 13.24 | 13.94 |
| Economic activities | Agriculture (corn, bean), breeding (sheep and goat), handcraft, merchants, bricklayers, bakers, drivers, day laborers, | Agriculture (corn, bean), bricklayers, bakers, carpenter, merchant, day laborer, store, cafeteria, driver. |
Floristic and ethnobotanical work. The permission of the communal and municipal authorities was requested in both SAN and SPT; for this, it was necessary to present the activities and objectives of the work in communal assemblies (Weckerle et al. 2009). In these meetings, it was possible to identify and approach members that the community recognized as being knowledgeable about medicinal plants because they worked as bonesetters, herbalists, therapists or midwives; therefore, they served as key collaborators. Four key collaborators were identified in each community, and between September 2015 and August 2016, field work was carried out to prepare an inventory of the medicinal flora known or used by these people. The work was complemented by semistructured interviews of key collaborators following Hurtado-Rico et al. (2006) and Hurtado-Ulloa & Moraes (2010) to obtain information on common names in Spanish and/or Mixtec for the species, as well as their medicinal uses, methods of preparation, and parts used. The properties in the hot-cold system were also recorded for each species following a classification with an emic perspective, in which the key collaborators assigned the property for each plant and its corresponding health condition, according to García-Hernández et al. (2015) and Geck et al. (2017).
The collected plant material was pressed, dried, and determined according to conventional techniques. One of the authors (RS) had a permit for botanical collections issued by the Mexican Environmental Ministry, which was valid during the study. Two sets of duplicates were prepared to be deposited in the Centro Interdisciplinario de Investigación para el Desarrollo Integral Regional Oaxaca, Instituto Politécnico Nacional (OAX) and Instituto Mexicano del Seguro Social (IMSS) herbaria. The assignment of species and genus names followed Villaseñor (2016), but in some instances, the Plant List (www.theplantlist.org) and Tropics (www.tropicos.org) databases were used.
With the information provided by the key collaborators, we made a catalog of the medicinal flora for each community, which included a photograph of each species as visual support. Following García-Hernández et al. (2015), the catalog was used as a tool in the structured survey (questionary format provided as Table S1 conducted from November 2016 to March 2017 at SAN, a community inhabited by 123 inhabitants in 62 households, and SPT, which has 179 inhabitants in 60 households (INEGI 2020). The survey allowed us to evaluate the degree of knowledge about the medicinal flora present in each community. None of the key collaborators from each community participated in this interview. In both communities, all households were visited to determine if their occupants use plants to meet their health needs; one member was interviewed per household (the decision of who was interviewed was made by the family), avoiding the participation of a second occupant to assure independent information. Of 62 households in SAN, 56 agreed (90 %) to respond to the survey, while of 60 households in SPT, 41 (68 %) agreed to the same. The interviewed inhabitants were 67 women and 30 men from 11 to 80 years old in both communities (Table 2). All informants from both communities were informed about the study goals and were asked for permission to be interviewed, guaranteeing his or her anonymity, privacy, dignity, and the confidentiality of the information provided. The guidelines of the Instituto Nacional de Ciencias Médicas y Nutrición (National Institute of Medical Sciences and Nutrition) Salvador Zubirán (INCMNSZ 2014), derived from the Declaration of Helsinki of the World Medical Association (WMA 2014) and the Code of ethics for research and ethnobotanic collaboration in Latin America (Cano-Contreras et al. 2015), were followed.
Table 2 Summary of the sociodemographic information of people interviewed in San Andrés Nuxiño (SAN) and San Pedro Topiltepec (SPT), communities of the Mixteca Alta region, Oaxaca, Mexico. For occupation, peasant indicates that the main work is related to corn and bean cultivation or sheep and goat breeding.
| Parameter | SAN | SPT |
|---|---|---|
| Informant number | 56 | 41 |
| Age category | ||
| Under 18 years | 3 (5.4 %) | 4 (9.8 %) |
| 18 - 60 years | 40 (71.4 %) | 30 (73.1 %) |
| Over 64 years | 13 (23.2 %) | 7 (17.1 %) |
| Genre | ||
| Women | 39 (69.6 %) | 28 (68.3 %) |
| Men | 17 (30.4 %) | 13 (31.7 %) |
| Occupation | ||
| Peasant | 12 (21.4 %) | 10 (24.4 %) |
| No peasant | 44 (78.6 %) | 31 (75.6 %) |
| Speak indigenous language (Mixtec) | ||
| Yes | 20 (35.7 %) | 1 (2.4 %) |
| No | 36 (64.3 %) | 40 (97.6 %) |
Analysis of data. The diseases and health problems treated with the plants, as reported by the informants, were grouped according to the guide of the International Classification of Primary Care (ICPC-2, available at https://www.who.int/standards/classifications/other-classifications/international-classification-of-primary-care) accepted by the World Health Organization (WHO) but modified with the help of key collaborators to generate an emic perspective (Staub et al. 2015). Key informants from both communities classified the health problems treated with medicinal plants according to the body system, and they agreed that cultural diseases should be grouped into the category of social problems. Within this category, there is a subclassification named sociocultural problems, where the world is analyzed according to parameters of the culture (Verbeke et al. 2006, WONCA 2015). The informant consensus factor (ICF) was also obtained (Trotter & Logan 1986) to estimate the level of similarity in the information provided by informants of each community about the plants used to treat the health problems in each category. The ICF was calculated as follows:
where Nur is the number of citations for the species used per category and Nt is the number of species used per category. The ICF takes a value from 0 to 1, where a value close to 1 indicates a well-defined selection criterion in the community and/or that the information is disseminated among the informants; a value close to 0 indicates that the choice of a species is random or that informants do not exchange information about its use.
A modified version of the relative value proposed by Vitalini et al. (2013) and Kayani et al. (2015) was employed to determine which body systems accumulate more mentions of plants used for treating health problems in each community. The value was calculated as follows:
where Ui refers to the number of species used per body system mentioned by community informants and N refers to the total number of species in each community.
In a similar way as mentioned above, the relative value of citations by body system was also calculated, which shows the local importance of the medicinal plants used. This value was calculated as follows:
where FC refers to the frequency of use citations per body system and N refers to the total number of citations of use.
The UV (Phillips & Gentry 1993) is a quantitative index calculated to determine the relative importance or versatility of each taxon used in each community depending on the different uses given to it. The UV was calculated as follows:
where Ui is the number of taxon uses mentioned by each informant and N is the number of informants.
Results
Richness of medicinal plants. In the two communities, 119 medicinal plant species were mentioned, belonging to 48 families and 109 genera (Table S2). Of these species, 73 are native to Mexico, and 46 are introduced. In SAN, 64 species were mentioned, 75 % native and 25 % introduced, while in SPT, there were 81 species, 52 % native and 48 % introduced; both communities had 26 species in common. In both communities, Asteraceae was the family best represented by the number of species, which was used to treat 82 diseases, followed by Lamiaceae, which was used to treat 52 diseases.
Figure 2 shows the percentages of medicinal plants that people obtain from different socioecological systems in each community. People from SAN obtained slightly more than half (58 %) of their medicinal species from the forest and almost a quarter of them (23 %) from home gardens. A different scenario occurred for SPT, where 62 % of medicinal plants comes from home gardens and 19 % from the forest.
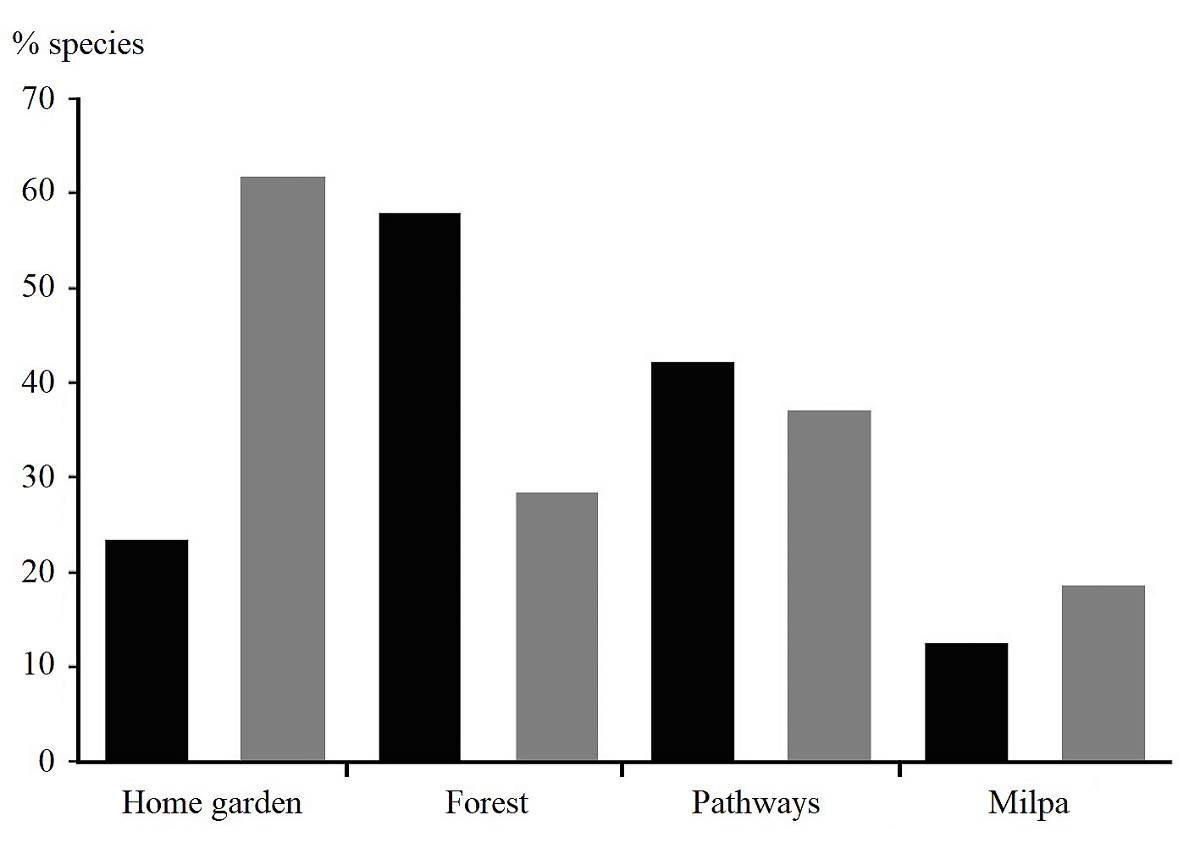
Figure 2 Percentage of plant species with medicinal use by socioecological system where they are obtained in San Andrés Nuxiño (black bars) and San Pedro Topiltepec (gray bars) in the Mixteca Alta of Oaxaca.
In SAN, medicinal plants recorded 1,135 use citations for the treatment of 134 health problems, while medicinal plants in SPT recorded 1,244 use citations and 177 health problems (Table S2). Medicinal plants from SPT, compared with those from SAN, had a lower average number of citations per species (15.36 vs. 17.73).
Parts used and mode of preparation. In both communities, the leaves were the part of the plant most frequently used, followed by flowers (Figure 3). In SAN, the leaves of 38 species (59 %) were used to treat 28 health problems, flowers of 18 plants (28 %) were used to treat 37 health problems, and roots of 14 species (22 %) were used to treat 38 health problems. In SPT, leaves of 62 plants (77 %) were used to alleviate 144 health problems, flowers of 30 species (37 %) were used to treat 52 diseases, and fruits of 14 plants (17 %) were used to treat 29 health problems. The plant structure and plant derivative with the lowest use frequency in both communities were bark and sap, respectively, but the latter was used only in SPT.
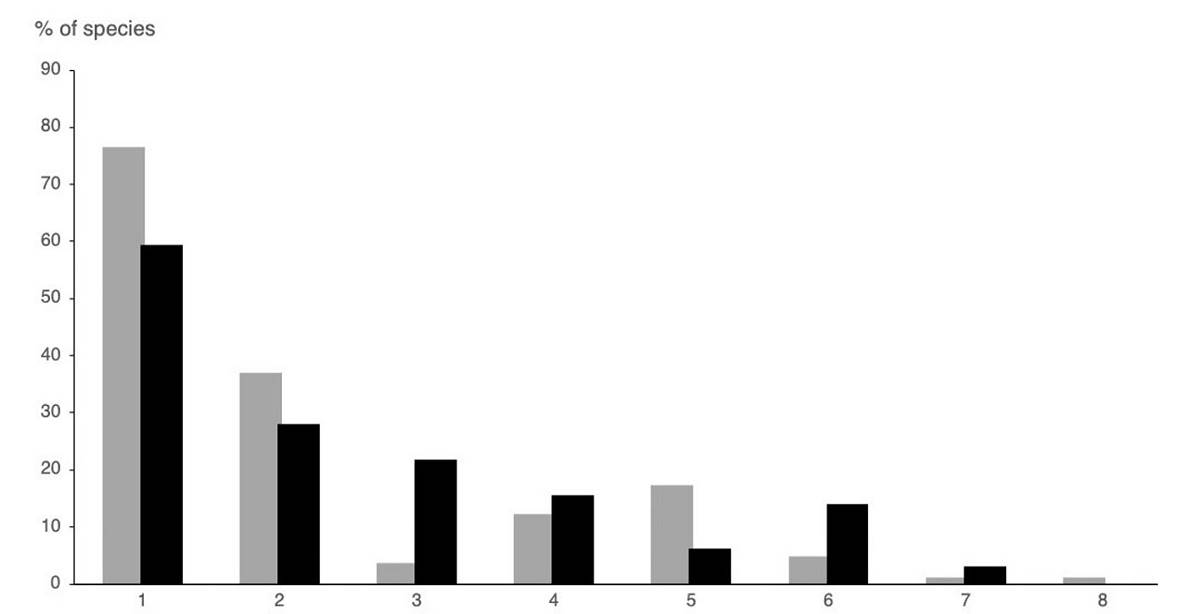
Figure 3 Percentages of plant parts used medicinally by informants from San Andrés Nuxiño (black bars) and San Pedro Topiltepec (grey bars) in the Mixteca Alta of Oaxaca, Mexico: 1 = leaves, 2 = flowers, 3 = root, 4 = the whole plant, 5 = fruit, 6 = stem, 7 = sap, and 8 = bark.
In SAN, the mode of application of medicinal plants was oral (infusion, decoction, crushed, minced, or roasted) or external (decoction, cataplasm, bath, washes, roasted, esquimil, crushed, minced or ramear). In SPT, the mode of application of the species was oral (infusion, decoction, crushed, or minced), external (decoction, cataplasm, bath, washes, roasted, macerated, crushed, minced or ramear), rectal (enema) or topical (pomade) (Table S2).
Some medicinal plants were prescribed in combination, but the plants used, and their therapeutics employed differed among communities. In SAN, an infusion with leaves of Mentha × piperita L. and Ruta chalepensis L. was used to treat migraine; a bath with leaves of Salvia lavanduloides Kunth and Heterotheca inuloides Cas. was for fever; a cataplasm with leaves of Stevia salicifolia Cav., Verbesina crocata (Cav.) Less. and Mimosa albida Humb. & Bonpl. ex Willd. was used to treat “cuerpo abierto” (open body); an infusion with leaves of Phytolacca icosandra L. and Ipomoea murucoides Roem. & Schult. was used for gangrene; and an infusion with cones of Juniperus flaccida Schltdl. and roots of Donnellsmithia cordata (J.M. Coult. & Rose) Mathias & Constance was used for urinary problems. In SPT, the combinations of medicinal plants used in infusions were as follows: leaves of Justicia spicigera Schltdl. and Agave nussaviorum García-Mend. were for anemia; leaves of Petroselinum crispum (Mill.) Fusss and Casimiroa edulis La Llave was for high blood pressure; leaves of Cirsium mexicanum DC. and Cynara scolymus L. were for weight loss; washes made with a combination of leaves and flowers of Heterotheca inuloides and stems of Equisetum hyemale L. were used to promote wound healing.
In SAN, there were 10 different modes in which plants were prepared for health care, while in SPT, 12 modes of preparation were recorded. In both communities, infusion was the most common form of preparation. In SAN, infusion was used for 80 % of the species, while in SPT, it was used for 89 % of the plants (Figure 4). In SAN, decoctions (water mixed with roots or bark over a fire) and washes (plant placed in cold or hot water) were the second most common preparation forms (22 % of the species in each one). In SPT, the second most common preparation form was washes (36 % of the species). In SAN, “ramear” (plant mixed with alcohol and then shaken over the body) and esquimil (leaves of Ageratina petiolaris (Moc. & Sessé ex DC.) R.M. King & H. Rob. and Sambucus nigra L. cooked with charcoal ash and applied as a cataplasm) were the least frequent forms of preparation (3%), while in SPT, it was roasted material and pomades (leaves of Calendula officinalis L. applied directly to the skin).
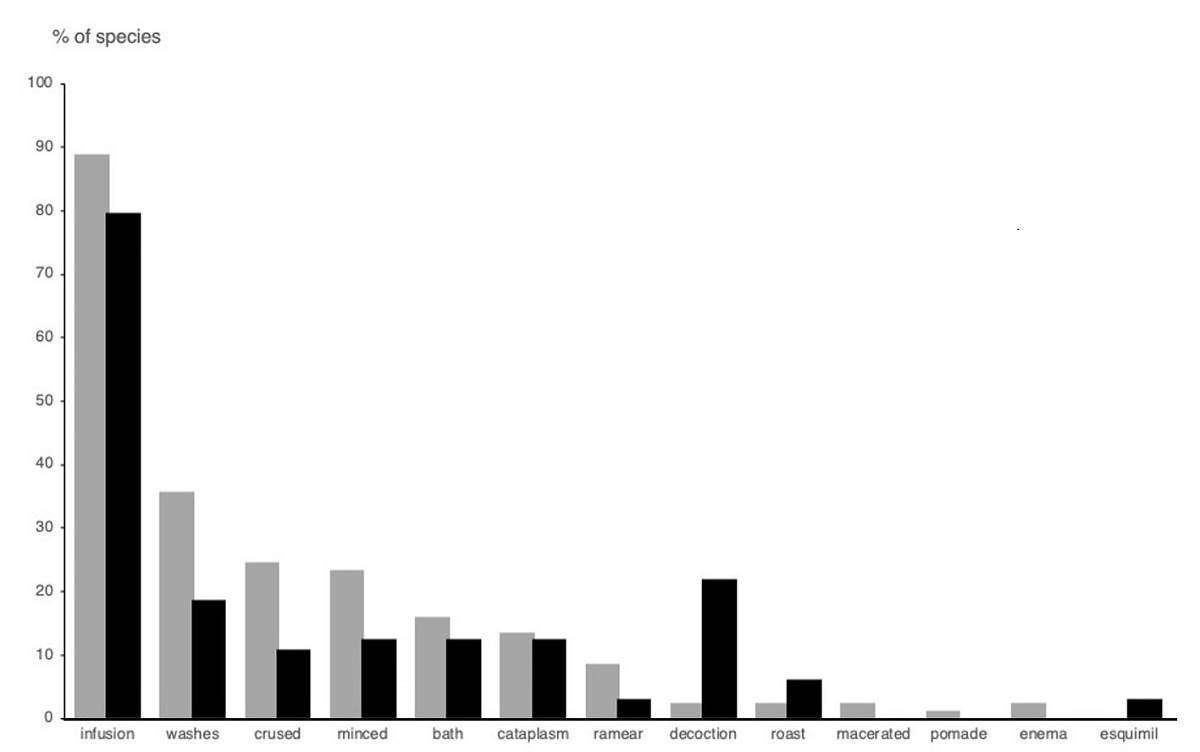
Figure 4 Percentages of forms of preparation of medicinal plants used by informants in San Andrés Nuxiño (black bars) and San Pedro Topiltepec (grey bars) in the Mixteca Alta of Oaxaca, Mexico.
Table 3 shows a comparison of the practices used in both SAN and SPT regarding the plant species involved, parts used, and preparation forms. In SAN, the category of illness for which most parts of the plant were used corresponds to the urinary system, while in SPT, most plant parts were used as remedies for conditions of the endocrine system. In SAN, social problems were the category with the most modes of preparation, but in SPT, the osseous system was the one with the most modes.
Table 3 Comparison of the therapeutic practices employed for the medicinal flora in two Mixtec communities of Oaxaca, Mexico. Number and percentages are based on the total number of health problems and medicinal species recorded in each community: in (SAN), 134 and 64, respectively; in (SPT), 177 and 81, respectively. Parts of plant: L = leaves, F = flowers, FR = fruits, R = roots, S = stem, B = bark, A = the whole plant, SA = sap, and N/C = not classified. Preparation form: 1 = roast, 2 = bath, 3 = cataplasm, 4 = decoction, 5 = esquimil, 6 = infusion, 7 = washes, 8 = crushed, 9 = minced, 10 = ramear, 11 = enema, 12 = macerated, and 13 = pomade.
| Health problems | Plant species used | Parts of plant used | Form of preparation | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SAN | SPT | SAN | SPT | SAN | SPT | SAN | SPT | |||||
| Body system | No. | % | No. | % | No. | % | No. | % | ||||
| Social problems (cultural diseases) | 11 | 8.2 | 6 | 3.4 | 21 | 33 | 17 | 21 | L, A, R, F | L, A, F | 1, 3, 4, 5, 6, 8, 9, 10 | 6, 10 |
| Skin | 17 | 12.7 | 25 | 14.1 | 25 | 39 | 34 | 42 | L, A, F, R, FR | L, A, F, FR, B | 1, 2, 3, 4, 6, 7, 8, 9 | 3, 7, 8, 9, 12, 13 |
| Respiratory | 15 | 11.2 | 13 | 7.3 | 28 | 44 | 31 | 38 | L, A, R, F | L, A, F, R, FR | 2, 3, 4, 5, 6, 7, 8 | 3, 4, 6, 8 |
| Blood | 4 | 3.0 | 14 | 7.9 | 8 | 13 | 12 | 15 | L, F | L, F, S | 3, 6 | 6, 8, 9 |
| General problems | 9 | 6.7 | 11 | 6.2 | 8 | 13 | 13 | 16 | L, A, FR, R | L, A, FR | 1, 2, 3, 6, 8, 9 | 1, 6, 7, 8, 9 |
| Nervous | 5 | 3.7 | 13 | 7.3 | 11 | 17 | 27 | 33 | L, A, F | L, F, A, FR | 6, 8 | 6, 8, 9, 10 |
| Urinary | 6 | 4.5 | 3 | 1.7 | 18 | 28 | 7 | 8.6 | L, F, A, FR, R, B, S | L, F, FR | 4, 6 | 6, 9 |
| Endocrine, nutrition and metabolism | 7 | 5.2 | 20 | 11.3 | 15 | 23 | 27 | 33 | L, F, A, B, S | L, F, A, FR, S, B, R | 6, 8 | 4, 6, 8, 9 |
| Muscular / Locomotor System | 14 | 10.4 | 11 | 6.2 | 24 | 38 | 16 | 20 | L, F, A, R, B | L, F, A, FR, B | 1, 3, 4, 6, 7, | 3, 6, 7, 8 |
| Bones / Osseous | 6 | 4.5 | 9 | 5.1 | 10 | 16 | 14 | 17 | L, R | L, FR, S | 1, 2, 3, 6, 7, 8 | 1, 3, 6, 7, 8, 9, 10, 12 |
| Women's diseases / Female reproductive system | 11 | 8.2 | 5 | 2.8 | 23 | 36 | 9 | 11 | L, F, A, B, R | L, A, F | 1, 4, 6, 9 | 6, 7 |
| Digestive | 18 | 13.4 | 28 | 15.8 | 33 | 52 | 48 | 59 | L, F, FR, A, R, S | L, A, FR, F, S | 3, 4, 6, 9 | 3, 6, 8, 9, 11 |
| Pregnancy and childbirth | 7 | 5.2 | 1 | 0.6 | 20 | 31 | 18 | 22 | L, F, A, B | L, A, F, FR | 1, 2, 4, 6 | 2, 6 |
| Diseases of man / Male reproductive system | 1 | 0.7 | 1 | 0.6 | 2 | 3.1 | 1 | 1.2 | F, FR | L | 6 | 6 |
| Eyes | 1 | 0.7 | 6 | 3.4 | 1 | 1.6 | 8 | 9.9 | A, SA | L, A, F, L, SA | 7 | 6, 7, 8 |
| Ears / Auditive system | 1 | 0.7 | 1 | 0.6 | 5 | 7.8 | 2 | 2.5 | L, R | L, A | 4, 6, 7 | 8, 10 |
| Brain | 1 | 0.7 | 0 | 0 | 1 | 1.6 | 0 | 0 | L | NC | 6 | NC |
| Teeth | 0 | 0 | 4 | 2.3 | 0 | 0 | 5 | 6.2 | NC | L, FR, S, A, B | NC | 4, 6, 8, 9 |
| Circulatory system | 0 | 0 | 3 | 1.7 | 0 | 0 | 11 | 14 | NC | L, S, FR, B | NC | 6, 8, 9 |
| Immune system | 0 | 0 | 3 | 1.7 | 0 | 0 | 10 | 12 | NC | L, A, F, FR, LA | NC | 6, 7, 8, 9 |
Informant consensus factor, relative value and use value. In SAN, medicinal plants were used to treat conditions that corresponded to 17 body system categories, while in SPT, plants were used to treat health problems that belonged to 19 categories. The key collaborators in SAN classified tooth problems as general problems and epilepsy as brain problems, while those in SPT classified the immune system, circulation, and teeth as separate systems. There were 1,135 recorded use citations for SAN and 1,244 for SPT. The disease categories with the highest ICF values were those related to the skin and respiratory systems in SAN and those related to the digestive and respiratory systems in SPT (Table 4).
Table 4 Disease classification with an emic perspective following the International Classification of Primary Care (ICPC-2), as was mentioned by key informants from San Andrés Nuxiño (SAN) and San Pedro Topiltepec (SPT), Oaxaca, México. Relative value for citations and species were calculated according the sum of mentions and number of species recorded in each community. CU = cites of use, RV = relative value, Sp = species, ICF = informant consensus factor. NA = Not apply.
| BODY SISTEM | SAN | SPT | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CU | RV (%) |
Sp (#) |
RV (%) |
Specie most cited |
ICF | CU | RV (%) |
Sp (#) |
RV (%) |
Specie most cited |
ICF | |
| Social problems (cultural diseases) | 61 | 5.4 | 21 | 32.8 | Clinopodium macrostenum | 0.67 | 54 | 4.3 | 17 | 21.0 | Clinopodium mexicanum | 0.70 |
| Skin | 238 | 21.0 | 25 | 39.1 | Anagallis arvensis | 0.90 | 156 | 12.5 | 34 | 42.0 | Heterotheca inuloides | 0.79 |
| Respiratory | 219 | 19.3 | 28 | 43.8 | Plectranthus hadiensis | 0.88 | 190 | 15.3 | 31 | 38.3 | Bougainvillea glabra | 0.84 |
| Blood | 19 | 1.7 | 8 | 12.5 | Justicia spicigera | 0.61 | 33 | 2.7 | 12 | 14.8 | Medicago sativa | 0.66 |
| General problems | 25 | 2.2 | 8 | 12.5 | Castilleja dendridion | 0.71 | 26 | 2.1 | 13 | 16.0 | Juglans regia | 0.52 |
| Nervous | 13 | 1.1 | 11 | 17.2 | Solanum lanceolatum | 0.17 | 73 | 5.9 | 27 | 33.3 | Lactuca sativa | 0.64 |
| Urinary | 117 | 10.3 | 18 | 28.1 | Equisetum hyemale | 0.85 | 7 | 0.6 | 7 | 8.6 | Cynara scolymus, Cirsium mexicanum, Ageratina petiolaris, Junniperus flaccida, Petroselinum crispum, Opuntia sp. and Arctostaphylos pungens | 0.00 |
| Endocrine, nutrition and metabolism | 29 | 2.6 | 15 | 23.4 | Crotalaria sp. and Lepechinia flammea | 0.50 | 89 | 7.2 | 27 | 33.3 | Opuntia sp. and Medicago sativa | 0.70 |
| Muscular / Locomotor System | 73 | 6.4 | 24 | 37.5 | Mimosa albida | 0.68 | 69 | 5.5 | 16 | 19.8 | Agave nussaviorum | 0.78 |
| Bones / Osseous | 22 | 1.9 | 10 | 15.6 | Boussingaultia sp. | 0.57 | 52 | 4.2 | 14 | 17.3 | Gymnosperma glutinosum | 0.75 |
| Women's diseases / Female reproductive system | 59 | 5.2 | 23 | 35.9 | Adiantum capillus-veneris and Cirsium ehrenbergii | 0.62 | 12 | 1.0 | 9 | 11.1 | Lippia graveolens and Ruta chalapensis | 0.27 |
| Digestive | 182 | 16.0 | 33 | 51.6 | Tagetes lucida | 0.82 | 320 | 25.7 | 48 | 59.3 | Chamomilla recutita | 0.85 |
| Pregnancy and childbirth | 64 | 5.6 | 20 | 31.3 | Chimaphila maculata | 0.70 | 43 | 3.5 | 18 | 22.2 | Phoradendron carneum | 0.60 |
| Diseases of man / Male reproductive system | 2 | 0.2 | 2 | 3.1 | Juniperus flaccida and Cirsium ehrenbergii | 0 | 1 | 0.1 | 1 | 1.2 | Arctostaphylos pungens | 0 |
| Eyes | 5 | 0.4 | 1 | 1.6 | Chamomilla recutita | 1 | 28 | 2.3 | 8 | 9.9 | Rosa gallica | 0.74 |
| Ears / Auditive system | 6 | 0.5 | 5 | 7.8 | Solanum lanceolatum | 0.2 | 3 | 0.2 | 2 | 2.5 | Argemone ochroleuca | 0.50 |
| Brain | 1 | 0.1 | 1 | 1.6 | Laennecia filaginoides | 0 | NA | NA | NA | NA | N/A | NA |
| Teeth | NA | NA | NA | NA | N/A | NA | 17 | 1.4 | 5 | 6.2 | Quercus castanea | 0.75 |
| Circulatory system | NA | NA | NA | NA | N/A | NA | 39 | 3.1 | 11 | 13.6 | Casimiroa edulis | 0.74 |
| Immune system | NA | NA | NA | NA | N/A | NA | 32 | 2.6 | 10 | 12.3 | Pinaropappus roseus | 0.71 |
The body systems that presented a higher relative value of appointments of use were skin (21) and respiratory (19.3) in SAN. In SPT, they were digestive (25.7) and respiratory (15.3) systems. The lowest values were for male reproductive (0.2) and brain (0.1) systems in SAN and for auditive (0.2) and male reproductive (0.1) systems in SPT. The relative value of species was higher for the digestive (51.6) and respiratory (43.8) systems in SAN and digestive (59.3) and skin (42) in SPT; the body systems with lower values were brain (1.6) and eyes (1.6) in SAN and auditive (2.5) and male reproductive (1.2) systems in SPT (Table 4). In both communities, the body systems with the highest relative value of species also had the highest ICF value.
In SAN, the UV ranged between 0.02 and 0.27; Solanum lanceolatum Cav. (0.27), Ruta chalepensis (0.25), Achillea millefolium L. (0.23), and Ageratina petiolaris (0.21) had the highest value in this community. In SPT, the UV ranged from 0.02 to 0.46, with the highest value observed for Aloe vera (L.) Burm. F. (0.46), Citrus × aurantium L. (0.44), Marrubium vulgare L. (0.39), Heterotheca inuloides (0.29), and Rosa gallica L. (0.29). The species with the lowest UVs were Ipomoea murucoides in SAN (0.02) and Morus nigra L. and Rubus adenotrichos Schltdl. in SPT (each 0.02) (Table S2). In SAN, 48 of 64 medicinal species were native (75 vs. 25 % introduced), while in SPT, 39 of 81 medicinal species were introduced (48 vs. 52 % native). Three of the four species with the highest UV in SAN were native, while in SPT, four of the five species with the highest UV were introduced.
In SAN, there were three introduced species, Ruta chalapensis, Leucaena leucocephala (Lam.) de Wit and Chamomilla recutita (L.) Rauschert, which were used for health problems of five body systems (cultural diseases, general problems, eye, nervous and digestive), for which there was no native medicinal plant as an alternative (Table S3). In SPT, a greater number of introduced plants (26 species) were used for health problems where there was no native plant as a medicinal alternative; these introduced plants were used for diseases related to skin, blood, nerve, endocrine, bone, female reproductive, digestive, eye, circulatory and general problems; the species were Aloe vera, Aloysia triphylla, Apium graveolens, Calendula officinalis, Chamomilla recutita, Citrus × aurantium, Cynara scolymus, Eriobotrya japonica, Iris germanica, Juglans regia, Lactuca sativa, Malva parviflora, Marrubium vulgare, Mentha × piperita, Pelargonium citrosum, Petroselinum crispum, Piper auritum, Plantago major, Punica granatum, Ricinus communis, Rosa gallica, Rosmarinus officinalis L., Stevia rebaudiana Bertoni, Taraxacum officinale F.H. Wigg. and Tropaeolum majus L. (Table S3).
Hot-cold dichotomy. Key collaborators from SAN mentioned 58 species that they use as medicinal plants as having a hot-cold property and stated that there were no intermediate categories. In SAN, 35 plant species (55 %) had a hot property and were used to treat cold health problems; another 23 species (36 %) had a cold property and were used to treat a hot condition. Six species did not have hot or cold properties: Agave nussaviorum, Juniperus flaccida, Leucaena leucocephala, Phytolacca icosandra, Ruta chalepensis, and Tagetes lucida Cav.
In comparison, in SPT, key collaborators agreed that all medicinal plants used had a hot or cold property; 39 species (48 %) had a hot property, and 42 (52 %) had a cold property. Sixteen species had the same property in both communities, but there were five species that differed: Justicia spicigera, Sambucus nigra and Adiantum capillus-veneris are cold plants in SAN, but in SPT, they were hot; Calendula officinalis and Cymbopogon citratus (DC.) Stapf were hot plants in SAN, but in SPT, they were cold. Table S2 shows the hot or cold properties of each medicinal plant mentioned in a consensual manner by key collaborators in each community, as well as the conditions treated with these plants. Table S3 includes information on local conceptions about qualities for medicinal plants, where plants were classified by key collaborators following an emic perspective according to ICPC-2, indicating which cold plants were used for a hot disease and which hot plants were used for a cold disease. Species identified as having a hot property were used to treat illnesses associated with bathing after birth and coughing, whereas species with a cold property were used to treat conditions such as anemia and depression.
Discussion
Richness of medicinal plants. The number of medicinal species reported (119) represents a lower richness in comparison with other similar studies, such as Frei et al. (1998a) and Arrazola-Guendulay et al. (2018) in Oaxaca, Magaña-Alejandro et al. (2010), Can-Ortíz et al. (2017) and Méndez-González et al. (2014) in Yucatán, and Geck et al. (2017) in Chiapas. However, the medicinal flora documented is greater than the richness reported by Juárez-Vázquez et al. (2013) in Guerrero; Canales-Martínez et al. (2005), Martínez-Moreno et al. (2006) and Vázquez-Medina et al. (2011) in Puebla; Alonso-Castro et al. (2012) in San Luis Potosí; and Giovannini & Heinrich (2009), Valdés-Cobos (2013), Nambo-Camacho (2015), and García-Hernández et al. (2015) in Oaxaca. On the other hand, Caballero et al. (2004) reported 203 species as medicinal plants used in Oaxaca, while Caballero & Cortés (2001) documented 145 medicinal plants in the Mixteca region. The richness of medicinal plants recorded here represents 58.6 and 82 % of the medicinal flora documented for Oaxaca state and the Mixteca region, respectively.
Among the medicinal flora reported here, the families represented by the greatest number of medicinal species in both communities were Asteraceae and Lamiaceae. This is not uncommon since Asteraceae and Lamiaceae are cosmopolitan families, both of which are among the most diverse worldwide (Heywood 1993), and they are among the eight richest families in Mexico, with 3,057 and 601 species, respectively (Villaseñor 2016). Because of its species richness, Asteraceae (856 species) turns out to be the most diverse family in Oaxaca, while Lamiaceae (139 species) occupies eleventh place (García-Mendoza & Meave 2012). Caballero et al. (2004) mentioned that Asteraceae and Lamiaceae are among the four families with a greater selection of species for medicinal uses in Oaxaca and that in this state, 16.7 % of their medicinal plants are Asteraceae and 5 % are Lamiaceae.
Five of the medicinal species reported here were documented with medicinal uses in two other communities from Oaxaca state, Santa María Tulancingo (García-Hernández et al. 2015) and Ayoquesco de Aldama (Arrazola-Guendulay et al. 2018), as well as in both communities in the present study. These species are Arctostaphylos pungens Kunth, Equisetum hyemale, Juniperus flaccida, Pinaropappus roseus, and Solanum lanceolatum; although in Santa María Tulancingo and Ayoquesco de Aldama, they were used for different conditions than those reported here.
The medicinal uses of most plants mentioned here have already been reported elsewhere; however, there were 24 species for which these uses were not mentioned in the literature about ethnomedicinal flora from Mixteca or Oaxaca (García-Mendoza et al. 2004, Valdés-Cobos 2013, García-Hernández et al. 2015, Nambo-Camacho 2015). These species are Acourtia reticulata (Lag. ex D. Don) Reveal & R.M. King, Agave nussaviorum, Boussingaultia sp., Cirsium mexicanum DC, Cirsium ehrenbergii Sch. Bip., Chimaphila maculata (L.) Pursh, Donnellsmithia cordata, Eryngium monocephalum, Geranium oaxacanum H.E. Moore, Ipomoea murucoides, Laennecia filaginoides DC, Malvastrum coromandelianum (L.) Garcke, Neogoezia gracilipes Hemsl., Penstemon campanulatus Willd., Phoradendron carneum Urb., Phytolacca icosandra, Psacalium paucicapitatum (B.L. Rob & Greenm.) H. Rob. & Brettell, Ruellia lactea Cav., Salvia lavanduloides, Salvia leucantha Cav., Salvia nana Kunth, Stevia salicifolia, Verbesina crocata and Verbena fastigiata Brandegee. For the other ten species, we reported at least one novel medicinal use: in SPT, a gel obtained from crushed Aloe vera, and in SAN, minced fruits from Leucaena leucocephala to treat stomach cancer. In SAN, the roots and stems were associated with a decoction as a preparation form, as reported by Giovaninni & Heinrich (2009), Alonso-Castro et al. (2012), and Valdés-Cobos (2013).
Among the 26 species that were common in both communities, four had different local names: Solanum lanceolatum Cav. was “venenillo” in SAN and “tabaquillo” in SPT; Justicia spicigera was “hierba tinta” in SAN and “muicle” in SPT; Ageratina petiolaris was “chanda” in SAN and “hierba de angel” in SPT; and Agave nuusaviorum was “maguey de pasmo” in SAN and “maguey papalome” in SPT.
Informant consensus factor and relative value. Medicinal plants from SPT had a lower average number of citations per species in comparison to SAN (15.36 vs. 17.73), as well as more preparation forms (12 vs. 10 forms). The highest ICF values for some categories of health problems in both communities were for digestive (stomachache and deworm), respiratory (cough and flu) and skin systems. These values indicate that knowledge about medicinal plants was similar among informants of each community and shared among people within the same community, as suggested by Juárez-Vázquez et al. (2013) and Baydoun et al. (2015). This ethnobotanical index is important since it could be useful to identify culturally important plants (Heinrich et al. 1998) but it also allows us to select medicinal species for a certain category of diseases when validating traditional knowledge about them through phytochemical and pharmacological studies (Canales-Martínez et al. 2006, Juárez-Vázquez et al. 2013, Nambo-Camacho 2015). High ICF values for digestive, respiratory and skin systems have also been reported in other Mexican indigenous communities, such as Nahua (Andrade-Cetto 2009, Juárez-Vázquez et al. 2013), Zapotec (Cervantes-Servín & Valdés-Gutiérrez 1990), Purepecha (Hurtado-Rico et al. 2006), Otomi (Sánchez-González et al. 2008) and Maya (Méndez-González et al. 2014), as well as in other countries (Kayani et al. 2015, Sadat-Hosseini et al. 2017). Respiratory and diarrheal illnesses are among the ten most common causes of death in communities in Oaxaca (SSA 2020).
A low ICF value for a disease category can be attributed to the tendency of people to use allopathic medicines at the same time as medicinal plants for health care (Upadhyay et al. 2011, Sadat-Hosseini et al. 2017) or the choice of species is random (Alonso-Castro et al. 2012, Juárez-Vázquez et al. 2013). In the two communities studied here, low ICF values were mentioned for a few species used in SAN and SPT to treat health problems associated with male-specific diseases/male reproductive systems.
The number of health problems designated cultural illnesses, classified here as social problems by key collaborators from both communities (eleven in SAN and six in SPT), have generally been considered in the literature to be unidentified (Rangel de Almeida et al. 2010), unspecified (García-Hernández et al. 2015), indefinite (Alonso-Castro et al. 2012, Juárez-Vázquez et al. 2013), or affecting different body systems (Ribeiro et al. 2017). We think that by considering these social diseases, we are recognizing the value of indigenous knowledge associated with health care and differentiating this knowledge from that of contemporary Western medicine (Heinrich et al. 1998).
Versatility and availability hypotheses. UV is an important index for identifying the most versatile medicinal species, which can then be selected for future pharmacological evaluations because the plants that have more usage reports have a higher UV (Gaoue et al. 2017, Hoffman & Gallaher 2007, Kayani et al. 2015, Zenderland et al. 2019, Sadat-Hosseini et al. 2017). When comparing the UV indices (an estimation of species versatility) of medicinal plants between SAN and SPT, differences were observed in the appreciation by the inhabitants for each species in each community. In SAN, three of the four species with the highest UV were native (Solanum lanceolatum, Achillea millefolium and Ageratina petiolaris), and one was introduced (Ruta chalepensis). In SPT, four of the five species with the highest UV were introduced (Aloe vera, Citrus × aurantium , Marrubium vulgare, and Rosa gallica), and one was native (Heterotheca inuloides). On the other hand, the species with the lowest UV (and versatility) were Ipomoea murucoides in SAN and Erythrina americana, Morus nigra and Rubus adenotrichos in SPT.
Among the introduced species recorded in this study, Aloe vera, Chamomilla recutita, Rosa gallica, Ruta chalapensis, and Lactuca sativa are considered cosmopolitan of European and/or Asian origins that were introduced to Mexico during the colonial period (Lozoya 1984). These plants became popular in the country, can grow in diverse climatic zones and their uses were extended to medicinal ones (Leonti et al. 2010). Therefore, these introduced species have now been included in local pharmacopoeias, as documented by several ethnobotanical studies (Martínez-Moreno et al. 2006, Hurtado-Ulloa & Moraes 2010, Magaña-Alejandro et al. 2010, Juárez-Vázquez et al. 2013, Can-Ortíz et al. 2017).
Interestingly, in the study communities, some introduced species were used to treat health problems where there was not a native plant as a medicinal alternative. In SAN, Ruta chalapensis was used to treat cultural (tantrums in children and bitter mouth due to anger in adults), nervous (migraine and embolism) and general (flea repellent) health problems. In SPT, Chamomilla recutita was used for skin problems (grains on the face) and eyes (eye wash); Aloe vera was used for skin conditions (clarifying and cleaning the face) and digestive (stomach cancer); Lactuca sativa was used for nervous (as a sedative), endocrine (for its contribution of folic acid) and circulation (to treat varicose veins) problems; and Rosa gallica was used for health problems of the digestive system (intestinal washes) and eyes (eye wash).
Our results contribute to the knowledge of medicinal resources in the Mixteca Alta region, and they could provide a primary source for research seeking natural remedies for health problems in zones where medical services are scarce or absent, medications are expensive, and the local economy is mainly based on self-consumption. But access to medicinal plants is high and they are available in socioecological systems in the community (home gardens, milpas, pathways or forest).
The number of species by socioecological system was used to test the hypothesis of availability of medicinal plants in the studied communities, as has been suggested by previous studies (Albuquerque 2006, Voeks 2004). In SAN, the socioecological system where the inhabitants obtained a higher percentage of plant species with medicinal use (58 % of 64 species) was the community forest, which was almost 60 minutes away from the community. Alternatively, home gardens within SAN only provided 23 % of their medicinal plants. Conversely, people from SPT obtained almost two-thirds of their medicinal plants (62 % of 81 species) from their home gardens compared with those provided by the community forest (19 %).
In SPT, inhabitants speaking an original language were scarce (1.97 %), and there was a lower percentage of households lacking drainage and using charcoal and firewood as fuel in comparison with SAN (Table 1). Traditional SPT medicine has been enriched with introduced species that grow in home gardens, which guarantees immediate access (Cordero et al. 2020). People from SPT employed almost the same percentage of introduced and native plants for medicinal use (48 vs. 52 %, respectively). Compared with native plants, the introduced ones were equally abundant and available in SPT, and several of them had a UV that was among the highest for this community. Among introduced plants were Aloe vera and Citrus × aurantium, which are cosmopolitan species used in popular phytotherapies worldwide (Ribeiro et al. 2017).
In SAN, most inhabitants still speak an original language (43 %), and there was a higher percentage of households lacking drainage and using charcoal and firewood as fuel compared with SPT (Table 1). In SAN, there was a lower percentage of introduced species with medicinal use compared with native plants (25 vs. 75 %, respectively); most native species were obtained from the community forest, and several of them had a UV that was among the highest for the community, such as Solanum lanceolatum and Achillea millefolium. This situation seems to be due to a greater dependence of the SAN inhabitants on the forest, where in addition to medicinal plants, they obtain wood and charcoal for domestic use or sale, as well as food products (Hurtado-Ulloa & Moraes 2010). This highlighted the importance of forest conservation in peasant communities as a means of preserving the natural landscape and traditional knowledge, since human-environment interactions are fundamental for learning about biological resources (Berkes (2003), such as plants for medicinal use (Turreira-García et al. 2015).
Some species reported as medicinal in both communities have been the subject of pharmacological studies or evaluation of their biological activity. Among the native species uses include antioxidant (Candan et al. 2003, Dolwitsch et al. 2016) and gastroprotective (Potrich et al. 2010) uses for Achillea millefolium; hypoglycemic (Bustos-Brito et al. 2016) uses for Ageratina petiolaris; cytotoxic (Egas et al. 2017), anti-inflammatory (Delgado et al. 2001) and hepaprotective (Coballase-Urrutia et al. 2010) uses for Heterotheca inuloides; and cytotoxic (Frei et al. 1998b) and anti-inflammatory (Herrera-Salgado et al. 2005) uses for Solanum lanceolatum. For introduced species, uses include antimicrobial (Gontijo et al. 2013), antibacterial (Salah et al. 2017) and antioxidant (Kumar et al. 2017) uses for Aloe vera; antioxidant (Wang et al. 2014), anti-inflammatory (Kang et al. 2011), hypoglycemic (Campbell et al. 2006) and anti-obesity (Verpeut et al. 2013) uses for Citrus × aurantium ; hepatoprotective (Akther et al. 2013), hypotriglycerides (Ibrahim et al. 2016) and antiseptic (Zarai et al. 2011) uses for Marrubium vulgare; and antimicrobial (Kacem et al. 2015) and anticonvulsant (González-Trujano et al. 2006) uses for Ruta chalepensis.
People of SAN depend to a greater extent on resources provided by the community forest for their daily life, which seems to explain why the forest continues to be the main source of plants for medicinal purposes. In contrast, people of the SPT community seem to be less dependent on their forest resources; instead, their home gardens have incorporated introduced plants that have acquired medicinal use, and they are cultivated there along with native species. According to Toledo (2003) and Saynes-Vásquez et al. (2016), the preservation of traditional knowledge can be related to the high prevalence of a native language and the practice of traditional self-consumption agriculture. A study in northern Mexico, where people do not speak a native language and agriculture is not for self-consumption, the medicinal plant that was the most versatile was an introduced species, Ruta graveolens L. (Alonso-Castro et al. 2012). However, in an indigenous community in Guerrero, the native Mimosa albida Humb. & Bonpl. ex Willd. was the medicinal plant that was the most versatile (Juárez-Vázquez et al. 2013). Other factors related to the local knowledge about the use of medicinal plants, not evaluated here, include age (Hurtado-Ulloa & Moraes 2010), gender, education (Saynes-Vásquez et al. 2016), and economic level (Carretero-Mendoza 2005).
Respect to the versatility hypothesis, the SAN community, where an original language (Mixtec) is still spoken and basic household services are scarce, uses more medicinal plants that are native to the region. While SPT, where speakers of an original language are scarce and households are provided with more basic services, uses similar percentages of plants native to the region as those that were introduced. On the other hand, for the availability hypothesis, SAN is a community that uses a higher percentage of species native to the region for medicinal use that are obtained from the community forest. In addition, SPT is a community that uses similar percentages of native and introduced plants for medicinal purposes, and most are obtained from home gardens. The traditional medicine of SPT turns out to be more dynamic than in SAN because the higher proportion of non-native species used in the former were originally introduced with different uses and were later incorporated into traditional medicine and maintained under cultivation in home gardens, as previously documented by Bennett & Prance (2000), Albuquerque (2006), Ceuterick et al. (2008), and Jernigan (2012). In this way, the incorporation of introduced plants generated an enrichment of traditional medicine in SPT.
Hot-cold dichotomy. The therapeutic concept of hot and cold properties is a fundamental part of the medicinal practices in the two communities studied here, where almost all plant species were classified with a hot or cold property by the key collaborators. Although this hot-cold concept is influenced by European humoral theory, an influence of medical beliefs and practices from Mesoamerican ethnicities is undeniable because the principle of binary opposition is incorporated into their medicinal systems, which evolved during colonial times by the incorporation of European medicinal theories and practices (Foster 1987, López-Austin 1980, Manderson 1987, Messer 1987, Tedlock 1987, Jackson 2001). This concept is based on the plant-disease relationship and involves selecting a plant for medicinal use and the balance of a healthy human body between a hot and cold state, in which an imbalance results in disease. A treatment based on medicinal plants has the objective of restoring health or balance to the body; the basic principle used to restore health lies in applying remedies with the opposite property to the disease (Foster 1986, Toledo 2003).
In the present study, the hot property predominates among native medicinal plants in comparison with the introduced ones (73 % in SAN and 62 % in SPT). Thus, traditional medicine in both communities presents a higher proportion of cold diseases. Few studies on the ethnobotany of medicinal plants provide information on their hot/cold properties, but those available agree in a higher proportion with a hot property (Hernández-López 1988, Vázquez-Medina et al. 2011, García-Hernández et al. 2015). The therapeutic selection of a plant with hot or cold properties can be determined by the healer’s experience and sensory perception (García-Hernández et al. 2015, Geck et al. 2017). However, studies focusing on this dichotomy and its relationships with phytochemical molecules and pharmacological activities are needed. This dichotomy has been documented for other ethnicities in southern Mexico, namely, Tzotzil (Holland 1963), Purepecha (Foster 1986), Nahua (Álvarez-Heydenreich 1987), Mazatec (Giovannini & Heinrich 2009), Chocholtec (García-Hernández et al. 2015), and Zoque (Geck et al. 2017). These beliefs are also held by Mexican migrants living in the United States (Manderson 1987, Waldstein 2010).
In summary, SAN and SPT are two communities close to each other, and their inhabitants are members of the same ethnicity (Mixtec), but there are differences between them in the selection of plants for medicinal use. In SAN, the highest proportion of medicinal plants corresponds to native species; the community forest is the socioeconomic system with the highest availability of medicinal plants, and among the most versatile species (those with the highest UV), native species predominate. In contrast, in SPT, similar proportions of native and introduced species are used as medicinal plants, home gardens are the socioecological system with the greatest availability of them and among the most versatile species are plants introduced to the community.
Supplementary material
Supplemental data for this article can be accessed here: https://doi.org/10.17129/botsci.2947.

