











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
According to the World Health Organization (WHO), cardiovascular diseases (CVs) continue to be the leading cause of non-transmissible diseases. CVs are the cause of 30% of the deaths reported in the world. Moreover, 68% of these deaths are due to ischemic heart disease of atherothrombotic etiology. Therefore, the main objective in patients with acute ST-segment elevation myocardial infarction (STEMI) is reperfusion of the responsible artery. Primary percutaneous angioplasty has shown superior benefit compared with thrombolysis.1 However, experimentally, the extent of rescued myocardial tissue has an inverse relationship with the time of evolution; hence, time is critical to preserve cardiac function.2
The CAPTIM study demonstrated that vessel patency improves the quicker the intervention occurs. The authors reported a lower incidence of cardiogenic shock and death within 30 days after the ischemic event when percutaneous coronary intervention (PCI) is performed within 2 hours of symptom onset.3 Developed countries have instituted initiatives focused on building governmental systems for comprehensive care in an acute myocardial infarction scenario because up to 30% of patients with the acute coronary ischemic syndrome do not receive a reperfusion strategy.4
By the end of 2019, local health care institutions in Wuhan city, Hubei province, China, had reported several clusters of an atypical, highly contagious pneumonia caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Given the rapid spread and severity, on January 30, 2020, the WHO declared that the COVID-19 outbreak an international public health emergency.5-7 The COVID-19 pandemic has placed international health systems in a serious overload situation, and with this, there has been inattention to other diseases, including those of cardiovascular origin. Given the urgent need for reperfusion treatment during acute coronary syndromes, be it pharmacological or invasive, in patients with and without COVID-19, various care protocols have been established and adapted to the capacities of hospitals around the world.8-12
The hospital where this research was carried out was converted to care for COVID-19 patients because it is a tertiary care setting. To guarantee the care of infarction code patients in the Bajío region, in addition to the hemodynamics room for patients with infarction code without respiratory symptoms, a hemodynamics room was set up for the exclusive care of patients with respiratory symptoms and suspected COVID-19 (Figure 1). This room included trained personnel equipped with personal protective equipment as well as a special path to transfer these patients from the emergency department to the hemodynamics room.
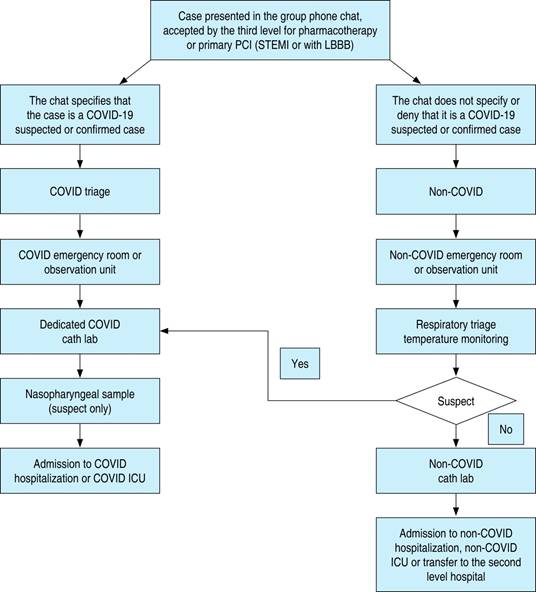
PCI = percutaneous coronary intervention. STEMI = ST-elevation myocardial infarction. LBBB = left bundle branch block. COVID = coronavirus disease. ICU = Intensive Care Unit.
Figure 1: Infarction code flow chart.
One year after the hospital had reopened all care services due to the significant decrease in the number COVID-19 cases, we wanted to evaluate the impact of the COVID-19 pandemic on infarction code functionality by comparing medical indicators of acute coronary syndrome with ST-segment elevation before and during the pandemic. We quantified the number of patients with ST-segment elevation acute coronary syndrome and the reperfusion strategies employed (fibrinolysis, primary angioplasty, and pharmacoinvasive angioplasty) during these periods.
Material and methods
An ambispective, analytical, comparative cohort study was performed, including the period from February to September 2019 (before the COVID-19 pandemic) and February to September 2020 (during the COVID-19 pandemic), for the High Specialty Medical Unit, Centro Médico del Bajío No. 1, Instituto Mexicano del Seguro Social (IMSS), Leon, Guanajuato, Mexico. Once approved by the local ethics and research committee with registration number R-2020-1001-086, all patients over 18 years old; of both genders; with clinical, electrocardiographic, and enzymatic data of acute coronary syndrome; accepted in the medical network as infarction code; and registered in the electronic case report form (eCRF) called Registro Nacional de Síndromes Isquémicos Coronarios Agudos (RENASCA) were included in the study. Patients with acute ischemic coronary syndrome without ST-segment elevation and patients who had not received tertiary medical care for any reason were not included. In addition, patients with incomplete records in RENASCA were eliminated.
The primary variables in this study were the number of patients with acute coronary syndrome, the reperfusion strategy, the needle-to-gate time, the balloon-to-gate time, and mortality. Other variables such as age, gender, body mass index (BMI), diabetes mellitus, systemic arterial hypertension, dyslipidemia, smoking, and the cardiac wall affected by infarction were also analyzed.
The Kolmogorov-Smirnov test was used to determine whether the continuous variables were normally distributed. Continuous variables are reported as mean ± standard deviation (SD) or median and interquartile range (IQR), as appropriate. Categorical values are presented as absolute values or percentages. The χ2 test and Fisher’s exact test were used to compare categorical variables, and Student’s t-test for independent samples was used to compare quantitative variables between groups. A p-value < 0.05 was considered significant. SPSS Version 23 software was used.
Results
A total of 212 patients were treated during the period of the COVID-19 pandemic, while 366 individuals were treated at the same time in previous year, representing a 42.1% reduction in the need for STEMI care. The characteristics of the patients were similar at both time points: a predominance of the male gender in 2019 (76.8%, 281) and 2020 (78.8%, 167), and a mean ± SD age of 62.34 ± 12.67 years in 2019 and 62.45 ± 11.73 years in 2020. The most predominant cardiovascular risk factors for 2019 and 2020 were systemic arterial hypertension at 65.57% and 62.7%, respectively; smoking at 55.2% and 51.9%, respectively; and diabetes mellitus at 46.2% and 49.1%, respectively. There were no significant differences between the two time periods regarding demographic variables, the presence of chronic degenerative diseases, and cardiovascular history (Table 1).
Table 1: Population characteristics.
| 2019 | 2020 | p | |
|---|---|---|---|
| Population | 366 | 212 | |
| Age (years)* | 62.34 ± 12.67 | 62.45 ± 11.73 | 0.072 |
| Male | 281 | 167 | 0.607 |
| Female | 85 | 45 | |
| Body mass index (kg/m2)* | 27.37 ± 4.07 | 27.48 ± 3.88 | 0.892 |
| Smoking | 202 | 110 | 0.489 |
| Diabetes mellitus | 169 | 104 | 0.545 |
| High blood pressure | 240 | 133 | 0.528 |
| Dyslipidemia | 92 | 49 | 0.616 |
| Previous heart attack | 58 | 25 | 0.218 |
* Mean ± standard deviation.
Note: none of the p-values are significant.
Concerning the acute coronary event, there were more patients with right ventricular extension in 2020 than in 2019 (24 vs 13, p = 0.01). More patients received the benefit of thrombolysis in 2020 (210 vs 154, p = 0.01), although there were no differences with respect to the presence of clinical symptoms or infarct location (Table 2).
Table 2: Location of the infarction.
| 2019 | 2020 | p | |
|---|---|---|---|
| Anterior wall | 136 | 83 | 0.657 |
| Inferior wall | 149 | 105 | 0.045 |
| Lateral wall | 53 | 35 | 0.549 |
| Right ventricle | 13 | 24 | 0.005 |
The data were analyzed with the χ2 test; p < 0.05 is significant.
During the COVID-19 pandemic, the time from symptom onset to hospital admission for medical care was longer (10.92 ± 16.57 h vs 6.95 ± 13.81 h, p = 0.02) as well as the door-to-electrocardiogram time (19.42 ± 30.75 h vs 15.25 ± 9.75 h, p = 0.01). However, there were no differences in relation to the other care indicators such as the door-to-needle, the door-to-balloon, and ischemia times (Table 3).
Table 3: Reperfusion time.
| 2019 | 2020 | p | |
|---|---|---|---|
| Door-to-needle time (minutes) | 17.55 | 25.95 | 0.131 |
| Door-to-balloon time (minutes) | 18.45 | 30.19 | 0.086 |
| Ischemia time (minutes) | 1377.96 | 1320.99 | 0.914 |
The data were analyzed with the independent samples t-test. None of the p-values are significant.
For 2019 and 2020, the most commonly affected segment of the heart wall during these events was the inferior wall at 40.7% and 49.5%, respectively; followed by the anterior wall at 37.2% and 39.2%, respectively; the lateral wall at 14.5% and 16.5%, respectively; and finally, the involvement of the right ventricle at 3.6% and 11.3%, respectively (Table 2).
The decision to perform thrombolysis as the initial reperfusion therapy was made in 210 patients (57.4%) patients in 2019 and 154 patients (72.6%) patients in 2020 (p = 0.001), achieving reperfusion criteria in 77 patients (21.0%) in 2019 and 75 patients (35.4%) in 2020 (p = 0.001). There were no significant differences between the time periods when the approach was invasive.
There were no significant differences regarding the time when reperfusion treatment was established. The average door-to-needle time was 17.55 minutes in 2019 and 25.95 minutes in 2020 (p = 0.131). The average gate-to-balloon time was 18.45 minutes in 2019 and 30.19 minutes in 2020 (p = 0.086). The ischemia time was also not different: 1377.96 minutes in 2019 and 1320.99 minutes in 2020 (p = 0.914) (Table 3).
Discussion
Acute myocardial infarction continues to be one of the main causes of morbidity and mortality worldwide. Hence, its timely and accurate diagnosis with the application of appropriate therapeutic management is vital.13
The benefits of the infarction code protocol have already been demonstrated in Spain, and this approach has been adapted to institutional medicine in Mexico, with a focus on emergency services. It complements the IMSS regulations, organizes the emergency and continuous admission services, and assigns specific activities to the personnel involved in patient care to guarantee the diagnosis and treatment of a patient who requires urgent care in an acute myocardial infarction scenario. With this protocol, patients receive reperfusion treatment with primary angioplasty in the first 90 minutes, or fibrinolytic therapy in the first 30 minutes after admission to the IMSS emergency services. Based on the most recent results for this national initiative, involving more than 21,827 cases, 71.4% of patients with the coronary ischemic syndrome were offered timely impact therapy, compared with 34.9% before the code had been instituted (p ≤ 0.0001), with a decrease in mortality from 21.1% to 9.4% (p ≤ 0.0001). The heart attack code initiative began formally in the High Specialty Medical Unit, Centro Médico del Bajío No. 1, IMSS, in December 2016. By 2018, mortality had decreased from 9.1 to 4%.14-17
By the end of 2019, local health care institutions in Wuhan city, Hubei province, China, had reported several clusters of an atypical, highly contagious pneumonia caused by a virus; it was suspected to be an airborne disease.18 The novel virus was first identified in January 2020, when Chinese scientists isolated it from patient samples. Its origin was suspected to be a local market for wild animals and seafood. On February 11, 2020, the virus was officially named SARS-CoV-2.5 In a matter of weeks, SARS-CoV-2 had reached pandemic proportions, affecting more than 100 countries.6,7 In Mexico, the first case was reported on February 27, 2020. Regarding the clinical manifestations of the disease, although they are predominantly respiratory, up to 19.7% of hospitalized patients develop some serious cardiovascular complication during their hospitalization.9 These complications include arrhythmias, myocarditis, pericarditis, heart failure, myocardial ischemia, and type 1 and type 2 acute myocardial infarction, or the exacerbation of an underlying cardiac disease, leading to higher mortality in hospitalized patients.19
In Western countries, in the presence of ST-segment elevation acute coronary syndrome, a rapid diagnostic test for SARS-CoV-2 should be performed and fibrinolytic therapy should be indicated as the first choice provided there are no contraindications,10 even in unstable patients. Only when there have been two negative COVID-19 tests should the necessary actions be taken.11 However, this approach is controversial because primary PCI is considered the standard of care for patients with STEMI in Europe, Canada, and the United States.20 On the other hand, access to rapid testing for COVID-19 is limited and in some countries such as Mexico it is not a procedure considered within the first line of screening to confirm or exclude SARS-CoV-2 infection.
The approach to a patient with COVID-19 and acute coronary ischemic syndrome with ST-segment elevation must be individualized, based on resources, exposure of health personnel, and the benefit of primary PCI. Therefore, during the COVID-19 pandemic, fibrinolysis in stable patients has been considered the best treatment option in most countries.8 In patients with STEMI and suspected COVID-19, which is defined as fever; respiratory symptoms; headache; cough; and some minor symptoms such as general discomfort, myalgias, arthralgias, and anosmia, primary or facilitated PCI is reserved for patients with clinical deterioration despite maximized treatment.21,22 In these patients, in addition to completing the protocol for the procedure, it is necessary to exclude the presence of SARS-CoV-2 by nasopharyngeal swab nucleic acid test and chest tomography, among other screening tests.
Contrary to conventional pharmacoinvasive approach, stable patients with confirmed COVID-19 infection who have undergone successful pharmacological thrombolysis should not be moved and scheduled for non-urgent cardiac catheterization. These patients should undergo appropriate follow-up and subsequent risk stratification and be relocated when they have defective fibrinolysis, especially if they are hemodynamically unstable.12 Given the changes implemented because of the overload of the hospital system, it is necessary to evaluate the effectiveness of the infarction code program as a viable initiative despite the limitations generated during this global event.
To provide timely care to patients with acute coronary syndrome with and without COVID-19, a care protocol was established to ensure the safety of health personnel and patients, with special care routes and a hemodynamics room exclusively for patients with severe respiratory symptoms.
The initial findings of our study agree with those reported in the international literature, with a reduction in patients treated for STEMI. Our 42.1% reduction is higher compared to reports of 22.7% in Spain and 38% in the United States.23,24
The duration of the ischemia is a major determinant of the size of the affected area in patients with STEMI, and timely recognition and early management are critical to reduce morbidity and mortality.25-27 Despite the logistic challenges associated with the COVID-19 pandemic, there was no significant difference in the delay in initiating reperfusion therapy. This demonstrates an excellent adaptation of the infarction code to the current crisis. The nonsignificant increase in the door-to-balloon time was likely due to protective measures required to carry out interventional procedures.
Some possible behavioral explanations for these findings could be the avoidance of seeking medical treatment due to social distancing measures, as well as concern about the risk of contracting SARS-CoV-2 in hospitals. The pandemic has received massive coverage in the media, with particular emphasis on the forms of infection and the most common places where SARS-CoV-2 is most easily spread.28,29 Fear is a well-known determinant of avoiding health care, and avoiding contact with the hospital environment is linked to a pandemic.30
The scientific community has developed recommendations for reperfusion strategies during the COVID-19 pandemic, with advice that may appear complex to apply, depending on the socio-economic status of each country. The Interventional Council of the American College of Cardiology and the Society for Angiography and Cardiovascular Interventions state that fibrinolysis should be considered for relatively stable patients with STEMI and active COVID-19 to prevent exposure of personnel. In Mexico, medical centers with catheterization rooms should favor primary PCI over justified fibrinolysis due to the high success rate, the lower risk of complications, and the shorter hospital stay. Fibrinolysis is the therapy of choice in centers that do not have a catheterization room available and/or in patients with pneumonia or severe COVID-19. It has been proposed to defer the conventional drug-invasive strategy to avoid transferring stable patients with confirmed COVID-19 who have had successful drug thrombolysis results.12
Previous publications have shown an increase in in-hospital mortality during the COVID-19 pandemic that is not explained by adjusting the data for COVID-19, age, gender, Killip class, and time from the onset of symptoms to the onset of reperfusion therapy.31 In the current context, patients avoid or delay going to the emergency room, a factor that could explain the increase in mortality in the out-of-hospital setting. This phenomenon has been described in Italy.31-35 Finally, in the long term, suboptimal revascularization and larger affected heart wall territories would increase the rate of complications related to worse ventricular remodeling, such as heart failure and the incidence of ventricular arrhythmias.
Limitations. This is an observational study, and our results reflect patients who arrived at the hospital alive. We do not have information of patients who died before or after hospitalization.
Conclusions
Although patients took longer to request medical care after they started having chest pain during the pandemic, medical indicators of care such as the door-to-needle and balloon-to-gate times were similar in both time periods, with similar mortality. These data reflect the proper functioning of the infarction code initiative during the COVID-19 pandemic in our hospital.

