











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
Echocardiogram is a non-invasive procedure to estimate the morphology and function of the heart; two-dimensional (2D) speckle-tracking echocardiography (STE) is an echocardiographic technique that is used as a tool to measure longitudinal, circumferential, radial and global deformation of both ventricles1-3. STE uses natural acoustic markers that are speckles in a gray-scale seen in 2D-mode images, as a consequence of the sound pulse random backscattering in a tissue plane explored by echography in structures smaller than the ultrasound wavelength4. With this technology, random noise is accurately filtered and these speckles are monitored and analyzed frame by frame. Its advantages with regard to other echocardiographic techniques include high spatial and temporal resolution, its independence from the sound beam angle of incidence (which allows analyzing segments that are not in parallel alignment with the ultrasonic beam), its availability, affordability, portability and safety. These principles are similar to those used in magnetic resonance imaging5.
STE allows rapid and accurate assessment of the myocardial function, where strain e describes myocardial deformation, i.e., the fractional change in the length of a myocardial segment. It has no unit and it is generally expressed as a percentage (%), and it can have positive or negative values that reflect lengthening or shortening, respectively. The term "global strain", or more precisely, "global longitudinal strain" or "global circumferential strain" generally refers to the average longitudinal or circumferential deformation components throughout the myocardium, which can be approached by the components of average segmental deformation in individual segments of the myocardial wall. Deformation values can be expressed for each segment (segmental strain, SLS) or as an average value for all segments (global strain, GLS)4.
In hemodynamic assessment with 2D echocardiography it is not usual for preload to be assessed; however, several animal studies have shown that assessment of the mechanics of left ventricle (LV) deformation with STE is sensitive to changes in loading conditions, and this should be emphasized, since the mechanics of LV deformation cannot be considered independent of the load, contractility indicators or lusitropism6.
STE has demonstrated its usefulness in the assessment of the RV in healthy subjects7 and in pulmonary hypertension8. Whether this technique is sensitive enough to assess changes in RV parameters without cardiopulmonary compromise with maneuvers that increase preload, such as raising the legs to 45°, is unknown. Leg elevation is a technique that has been used to increase preload in healthy subjects9-11, post-heart transplant12, and in states of shock and hypotension13.
Preload is one of the main determinants of cardiac output. Classically, it has been defined as the maximum degree of stretching or tension of the myocardial fiber prior to starting ventricular contraction, and is determined by end-of-diastole sarcomere mean length. Clinically, this definition is not practical and is difficult to apply; as a result, it is replaced by more accessible ventricular filling measurements, such as intracavitary pressures or end-diastolic volumes. Although none of these parameters reflects the elongation of cardiac muscle fiber, they offer an accepted approximation of preload real value14.
Changes in preload or afterload conditions have been shown to affect the mechanics of LV deformation15.
For this reason our objective was to describe with STE what the behavior of RV GLS and SLS would be in a four-chamber approach with a change of position of the legs as an estimate that would suggest preload changes in subjects without prior cardiopulmonary pathology.
Method
Using a case series design, consecutive subjects with no evidence of cardiopulmonary disease were assessed.
Inclusion criteria
Healthy subjects of both genders, with ages ranging between 16 and 53 years. Exclusion criteria: poor acoustic window, heart and lung disease diagnosis, not authorizing the performance of the echocardiogram.
Pulsed and continuous color Doppler 2D-mode transthoracic echocardiogram was performed. Subsequently, four, three and two-chamber 2D gray-scale images were acquired with a General Electric Vivid 7® equipment with a 3 MHz transducer. The STE images were post-processed using the EchoPac program.
Maneuver
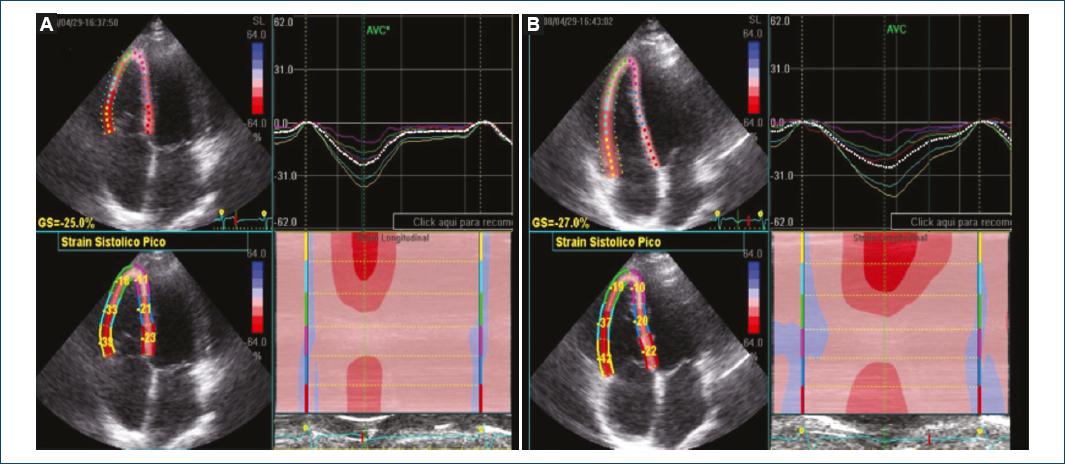
With the subjects at rest in the supine position and then with elevation of both legs to 45° for 5 minutes, 2D-mode images were acquired with a four-chamber approach before and after the maneuver, with basal RV free wall, middle RV free wall, apical RV free wall, basal lower septum, mid-lower septal and apical septal GLS and SLS being determined with STE. The variables that were obtained were: GLS and SLS before and after leg elevation.
Statistical analysis
Continuous variables are expressed as the mean ± standard deviation. The differences before and after the maneuver (leg elevation to 45°) were analyzed with Students t-test for dependent samples. A p-value < 0.05 was considered statistically significant. GLS and SLS intra-observer variability was estimated with the intra-class correlation coefficient and its respective 95% confidence interval. The statistical analysis was carried out with the Excel® and SPSS® version 16 statistical programs.
Results
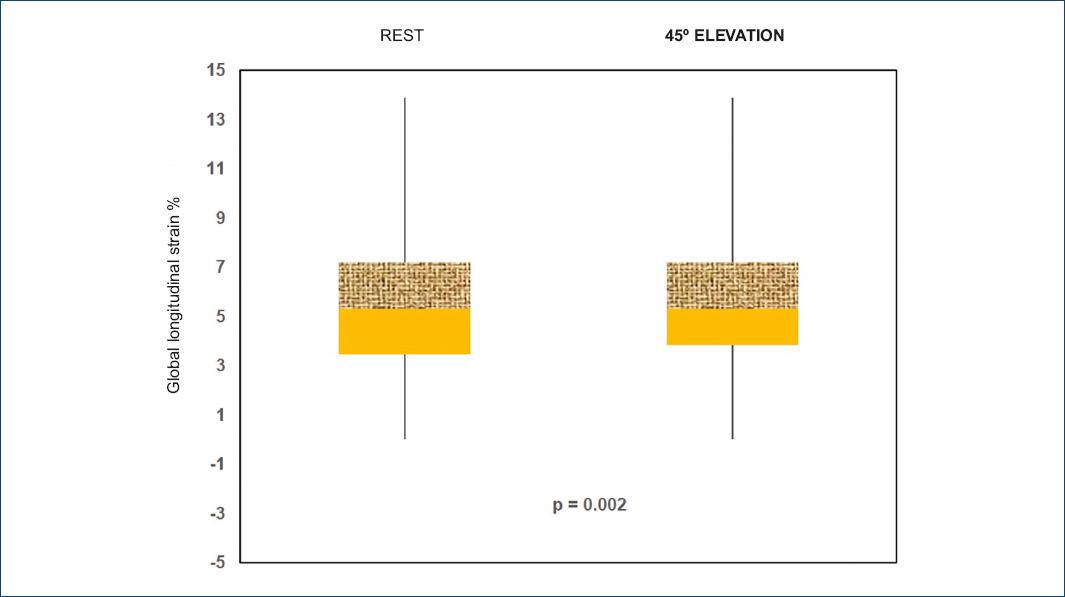
Thirty-one subjects were analyzed, 16 men and 15 women with ages ranging from 16 to 53 years. GLS and SLS behavior before and after leg elevation to 45° is shown in table 1 and figure 1; a box and whisker plot shows mean differences and the distribution is observed to be larger (i.e., higher dispersion), and there is also a positive bias for the subjects at rest (Fig. 2). The intra-class correlation coefficient was calculated: 0.773, with a 95% confidence interval (CI) of 0.534-0.890; p < 0.001.
Table 1 Percentage differences in segmental longitudinal strain and global longitudinal strain at rest and with leg elevation to 45º
| Assessed segment | Baseline SLS and GLS % n = 31 | SLS and GLS % with leg elevation to 45º n = 31 | p |
|---|---|---|---|
| Basal RV free wall | —29.1 ± 3.3 | —32.7 ± 5.5 | 0.0002 |
| Middle RV free wall | —28.6 ± 6.4 | —31.5 ± 4.9 | 0.001 |
| Apical RV free wall | —21.9 ± 6.5 | —23.3 ± 6.1 | 0.118 |
| Basal lower septum | —19.4 ± 3.2 | —18.9 ± 3.0 | 0.204 |
| Middle lower septum | —19.3 ± 3.2 | —19 ± 3.1 | 0.249 |
| Apical septal | —17.1 ± 5.1 | —17 ± 5.4 | 0.457 |
| GLS | —23.06 ± 3.4 | —24.5 ± 2.9 | 0.002 |
GLS: global longitudinal strain; RV: right ventricle; SLS: segmental longitudinal strain.
Discussion
2D STE measures RV GLS and SLS with a four-chamber approach. We measured it in healthy subjects at rest and with position changes (leg elevation to 45°), a maneuver that was used with the purpose to increase preload. There are no previous studies on RV performing this maneuver. There are studies on LV where STE-observed longitudinal and circumferential strain has been calculated to be affected by acute changes in saline infusion-induced preload16. We obtained significant GLS and SLS differences in the basal and mid-RV free-wall segment. We found that the strain is more negative with leg elevation to 45°, which supports that the greater the stretching of the myocardial fiber by increasing the preload, the more negative the generated deformation, indicating that there is a greater shortening of the fiber, and this method can measure those differences.
Conclusions
Despite the limitations of the method for analyzing the RV in subjects without cardiopulmonary compromise, this method was sensitive to detect differences in GLS and SLS in basal and mid-RV free-wall segments.
Ethical disclosures
Protection of people and animals The authors declare that no experiments have been conducted on humans or animals for this research.
Confidentiality of data The authors declare having followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent The authors declare that no patient data appear in this article.

