










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista odontológica mexicana
versión impresa ISSN 1870-199X
Rev. Odont. Mex vol.28 no.3 Ciudad de México jul./sep. 2024 Epub 01-Sep-2025
https://doi.org/10.22201/fo.1870199xp.2024.28.3.91065
Clinical case
Class II treatment with auto transplantation at the maxillary central site: Case report
1 Departamento de Estomatología, Servicio de Ortodòncia del Hospital Infantil de México Federico Gómez, Ciudad de México.
2 Cirujano Dentista especializado, adscrito al servicio de ortodoncia del Hospital Regional de Alta Especialidad de Ixtapaluca, Estado de México.
3 Profesor de Asignatura A de la Facultad de Estudios Superiores Iztacala, UNAM.
4 Residente de 3er año de la especialidad de ortodoncia Hospital Infantil de México Federico Gómez, Ciudad de México.
5 División de Estudios de Posgrado e Investigación, Facultad de Odontología, Universidad Nacional Autónoma de México, Ciudad de México.
Introduction: Dental autotransplantation as a therapeutic alternative to the loss of a central incisor represents a great challenge for the orthodontist, proper planning and execution of treatment can provide aesthetics, function and long-term stability. Objective: To illustrate the treatment of an adolescent patient with skeletal Class II malocclusion, who had a history of trauma in the anterior maxillary region. Case Presentation: A 14-year-old male, apparently healthy, presented for consultation due to dissatisfaction with the different heights of his maxillary central incisors as a consequence of previous trauma and the lack of progress in his ongoing treatment. During the clinical and radiographic examination, a Class II skeletal pattern was determined, along with vertical growth, a retrusive chin, increased inter-labial distance, and bimaxillary protrusion. The right maxillary central incisor showed evidence of a previous inadequate endodontic treatment, in addition to external root resorption and localized periodontal disease, with an unfavorable prognosis for the tooth. The parents were informed about the therapeutic complexity and risks involved in resolving this issue. We proposed to initiate a new orthodontic treatment with fixed appliances, perform four premolar extractions, and extract the right maxillary central incisor. An autotransplant of the left lower first premolar was performed to replace the central incisor due to its poor prognosis. The treatment plan was accepted and executed as planned. The results, in terms of stability, functional permanence, and proper prosthetic characterization as the right maxillary central incisor, along with favorable radiographic control of endodontic treatment and periodontal health over 12 years, demonstrate the success of this case. Conclusions: The transplant favors function, aesthetics, and long-term stability. Monitoring the transplant of developing premolars is essential during follow-up appointments.
Keywords: Dental autotransplantation; Class II malocclusion; Functional occlusion; Periodontal health
Introducción: El autotransplante dental como alternativa terapéutica ante la pérdida de un incisivo central, representa un gran desafío para el ortodoncista, una adecuada planeación y ejecución de tratamiento puede brindar estética, función y estabilidad a largo plazo. Objetivo: ilustrar el tratamiento de un paciente adolescente de clase II esqueletal, con antecedente de traumatismo en la región maxilar anterior. Presentación del caso: se presentó masculino de 14 años, aparentemente sano. El motivo de consulta fue su inconformidad al respecto de las diferentes alturas que tenían sus incisivos centrales maxilares como consecuencia del traumatismo que sufrió anteriormente y por la falta de avances en su tratamiento hasta ese momento. Durante el examen clínico y radiográfico, se determinó un patrón esqueletal de clase II, crecimiento vertical, mentón retrusivo, distancia inter-labial aumentada y biproquelia. El incisivo central superior derecho radiográficamente evidenciaba un tratamiento endodóncico previo deficiente. Además, presentaba resorción radicular externa y enfermedad periodontal localizada, con pronóstico no favorable para la pieza dental. Se les informó a los padres del menor la complejidad terapéutica y riesgos que representaba resolver este problema. Se les propuso realizar un nuevo tratamiento de ortodoncia con aparatología fija, 4 extracciones de premolares y la extracción del incisivo central superior derecho. Se realizó autotransplante del primer premolar inferior izquierdo hacia el sitio del central maxilar para sustituir a éste, ya que su pronóstico era malo. El tratamiento fue aceptado y ejecutado conforme a lo planeado. Los resultados en términos de estabilidad, permanencia funcional y la adecuada caracterización protésica como incisivo central superior derecho, control radiográfico del tratamiento endodóntico favorable y la salud periodontal a través de 12 años, evidencian el éxito de este caso. Conclusiones: el trasplante favorece la función, estética y estabilidad a largo plazo. El monitoreo del trasplante de premolares en desarrollo es obligatorio durante las citas de seguimiento.
Palabras clave: Autotrasplante dental; Maloclusión clase II; Oclusión funcional; Salud periodontal
Introduction
The loss of a permanent maxillary central incisor in a young patient is a therapeutic challenge for dental professionals1. Dental transplantation is defined as the transplantation of included or erupted teeth from one site to the extraction site or surgically prepared alveolus in the same person2-4. Adequate therapeutic management favors the restoration of a normal alveolar process, oral health, esthetics, and long-term stability as reported by some authors. Premolar transplantation has been reported since the 1970s and premolar teeth are recommended for autotransplantation since their morphology can be easily adapted to simulate incisor teeth5-8.
Czochrowska et al.9 reported the gingival and periodontal results of 45 auto-transplanted premolars in the maxillary anterior region to replace maxillary incisors, 39 central incisors, and six lateral incisors in 11-year-old children evaluated at four years after transplantation. On the other hand, Bowden10 reported results of 34 transplanted premolars evaluated at periods of 3.3 and 8.7 years, and only two showed signs of root resorption, the rest remained in place with vitality and formed roots.
With recent advances in technology and a better biological understanding, autotransplants have become more predictable. These treatment alternatives have been very successful from a biological and clinical point of view, thus presenting this therapy as a good option5,6,11-15.
In patients with missing maxillary incisor teeth, these can be replaced by moving the upper lateral incisor orthodontically and then restoring it prosthetically. Another good option is the autotransplantation of an extracted mandibular premolar. This treatment method can replace the missing maxillary central incisor successfully, due to morphological similarity (shape, size, and root canal)10,16. According to Akhlef17, premolars are the most donated teeth; they can be beneficial when replacing missing teeth, because of the survival and success rate. After evaluating autologous transplants 22 years after autotransplantation, they showed a success rate of 93%.
Periodontal ligament formation, and proprioceptive rehabilitation, allow for continued bone and gingival formation as reported by Park18. These biological considerations allow orthodontically transplanted teeth to be moved safely19. Early application of orthodontic forces may improve the prognosis of autotransplanted teeth20. Consequently, these tooth transplantation protocols are useful for orthodontists because the transplanted tooth can move after three to six months post-transplantation. The premolars can provide an optimal and more favorable width at the gingival level, unlike the lateral incisors, which is an important factor for future restoration, since similarity to the lost central incisor is sought1,18,20. Patients with Class II malocclusions can be treated with two or four premolar extractions, although there is evidence of possible slight changes in occlusion after removal of appliances associated with treatment with four extractions21,22.
The purpose of this case report was to illustrate the treatment of an adolescent patient with skeletal Class II malocclusion, moderate crowding in the lower arch, and a history of avulsion in the upper central incisor with external root resorption treated with autotransplantation, endodontics, and fixed orthodontics.
Clinical case presentation
A 14-year-old adolescent patient attended the clinic. His reason for consultation was a complaint about the different heights of his anterior teeth and unsatisfactory results from his previous orthodontic treatment. This was particularly evident when smiling, he also showed gingivitis associated with bacterial plaque and incomplete orthodontic appliances. Extraoral analysis revealed an oval face with disproportionate facial thirds and hyperactive chin muscle; Facially, he showed a disproportionate face, with increased lower facial third, lip incompetence, and excessive exposure (Stm-Incisal Edge=5mm) of the upper incisors during the smile, as well as a smile arch in line with the lower lip, slightly convex and obtuse nasolabial angle, the chin slightly retrusive. It was also observed that the interlabial distance was increased and both lips presented protrusion when evaluated with the vertical to subnasal line (LS-LVs=5mm).
Intraoral analysis revealed the presence of incomplete orthodontic appliances, the right upper central incisor showed an evident unevenness and gingivitis; the dental relations were molar class I and bilateral canine class I. The relationship between overbite and overjet was altered and the lower dental midline was deviated 1.6 millimeters to the left from the facial midline. The maxillary arch presented a normal transverse dimension, the occlusal plane was leveled, and the right central incisor had problems with position and color. Specifically, the analysis of the maxillary arch revealed the presence of an upper right central incisor with a history of avulsion and endodontic treatment, with retrograde obturation technique, which was reimplanted by the previous treating dentist (Figure 1).

Figure 1 Initial photographs. A. Extraoral at different angles. B-C. Intraoral with and without the appliance, where the malposition of tooth 11 is evident.
The orthopantomography showed complete dentition, with the presence of the upper central incisor with external root resorption and endodontic seal material. This finding was corroborated with the dentoalveolar radiography. The cephalometric analysis revealed a Class II intermaxillary relationship (ANB 6°), with the mandible in retro position, a slight excess of mandibular body length, maxillary dentoalveolar inclination. In addition, the vertical facial pattern was hyper-divergent (385°) with clockwise growth and brachyfacial pattern. He also had palatalization of the upper right central incisor and proclination of the upper left central incisor (incisor to palatal plane = 112.6°) and the lower central incisor (mandibular plane = 100.1°), increasing the overjet and overbite. Together, these characteristics pointed to a dental malocclusion that needed correction by the values shown in Table 1.
Table 1 Pre-treatment, Post-treatment and Cephalometric Measurements 12 years after treatment. These measurements can be compared to the normal cephalometric values of column 4.
| Cephalometric Measurements | Pre-treatment Values T1 | Post-treatment Values T2 | 12 years after treatment T3 | Normal values |
|---|---|---|---|---|
| Horizontal Skeletal | ||||
| SNA, (°) | 86.4 | 83.5 | 81.9 | 82 |
| SNB, (°) | 80.4 | 80.4 | 78.8 | 80 |
| ANB, (°) | 6 | 3.1 | 3.2 | 2 |
| Maxillary Depth (°) | 94.1 | 90.5 | 91.9 | 90 |
| Maxillary Skeletal (A-Na Perp) (mm) | 3.7 | 1.8 | 0.5 | 0.0 |
| Vertical Skeletal | ||||
| Md - SN Plane (°) | 34.4 | 34.9 | 32.1 | 33.0 |
| SN - GoGn (°) | 33.2 | 34.5 | 30.7 | 32.0 |
| FMA (MP-FH) (°) | 26.8 | 24.9 | 25.0 | 22.9 |
| Lower facial height (°) | 47.6 | 45.3 | 46.7 | 45 |
| Facial Axis, (°) | 91.6 | 90.7 | 89.7 | 90 |
| Occlusal plane to SN (°) | 12.7 | 14.3 | 12.7 | 14.4 |
| Anterior Dental Relationship | ||||
| U1-SN (°) | 112.6 | 103.8 | 103.5 | 104 |
| U1 - NA (mm) | 6.5 | 2.9 | 3.4 | 3.4 |
| L1 - NB (mm) | 7.7 | 3.6 | 4.4 | 4.4 |
| L1- NA (°) | 26.1 | 21.6 | 20.4 | 22.8 |
| IMPA, (°) | 100.1 | 90.3 | 91 | 90 |
| Interincisal Angle (°) | 112.9 | 133.8 | 130.6 | 136 |
Table footnote: Comparison of linear and angular values between T1, T2, and T3.
As for the sagittal dental relationships, these were right molar class I, left molar class I, right canine class I, and left canine class I. The inclinations of the maxillary incisors and mandibular incisors were altered concerning their bony bases (Figure 2).
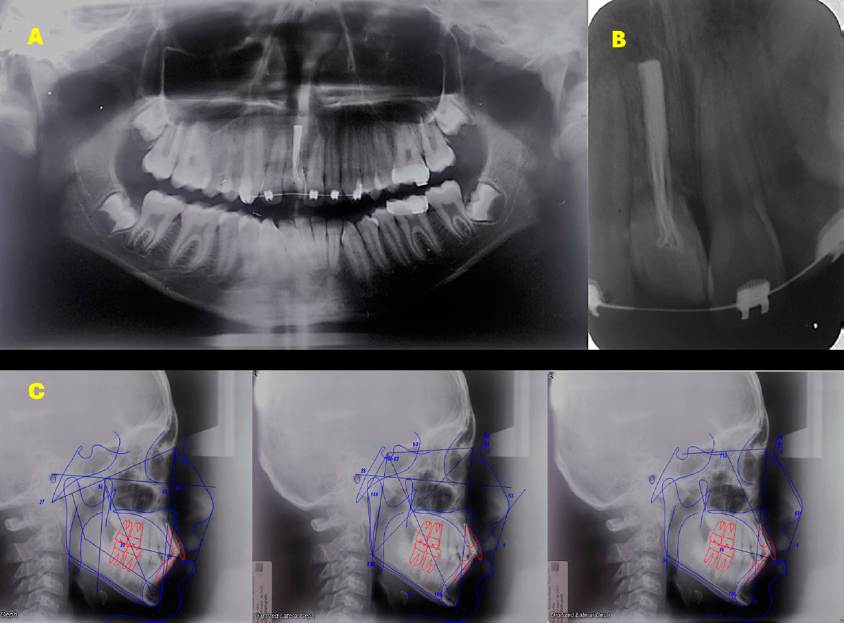
Figure 2 Radiographs. A. Orthopantomography. B. Dentoalveolar of tooth 11, showing external root resorption and root canal treatment. C. Initial cephalometric tracings.
With the list of problems described above, the following objectives were proposed: to extract the upper right central incisor and transplant the lower left first premolar immediately to the recipient site, raising the occlusion to avoid occlusal loads -according to Bowden10, these protocols have 97.4% success rate-, to eliminate crowding in both arches, improve the lower midline to the left, and restore dental function and esthetics; it was also desired to preserve the position of the first molars of quadrants 1 and 2 with maximum anchorage and retract the anterosuperior segment to improve the overbite, allowing the coordination of both arches and thus maintain the stability of the transplanted maxillary central incisor.
In the first phase of treatment, bands were placed on the upper first molars, an anchorage device was used, and the bite was lifted with an acrylic plate to avoid occlusal contact. Subsequently, the upper right central incisor was extracted, following the protocol for the extraction of the lower left first premolar, preparation of the surgical site, and the process of dental transplantation and splinting for four weeks (Figure 3). In the second phase, GAC© prescription Roth 0.022” Ovation brackets were placed. They were first placed in the lower arch to reduce the inclination of the incisors and improve the position of the teeth while the repair and healing of the peri-implant tissue of the auto-transplanted tooth was being performed (Figure 4).
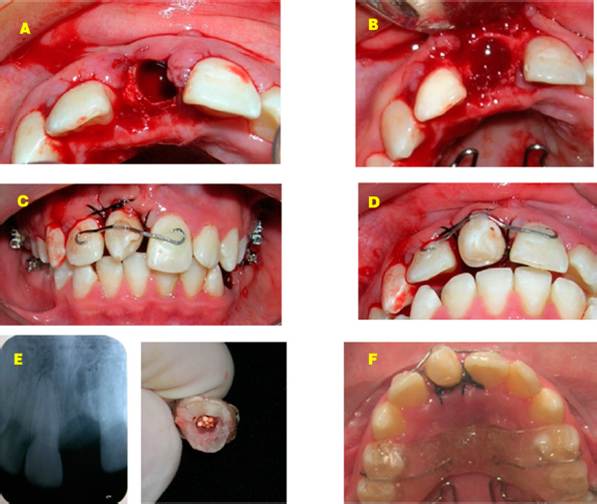
Figure 3 First phase of treatment. A-B. Preparation of the receptor niche. C-D. Fixation of the transplanted tooth in the maxillary central site. E. Post-extraction dentoalveolar radiograph. F. Use of the acrylic plate to promote bite opening.

Figure 4 Progress photographs. A. Extraoral. B. Intraoral with lower appliance. C. Series of dentoalveolar radiographs showing the transplanted tooth without apical reaction.
Root canal treatment was performed at week four to reduce the risk of developing complications related to pulp tissue detachment, its nerves, and vascular support24. As for occlusal refinement, this was performed by placing fixed appliances, extractions of upper first premolars, alignment, leveling, space closure, and completion of the orthodontic stage, to comply with the principles of stable occlusion and respect the esthetic demands of the patient. During appliance placement, we took care of the position of the brackets, since it is of utmost importance to provide root parallelism. Leveling and alignment is a complex process in which all crowns, including tooth 11 with a temporary crown (Figure 5) move at the same time and in different directions developing reciprocal forces between them, which can be of great help to direct the movements in our favor and thus achieve the characteristics of a natural occlusion and improve the soft tissue characteristics of the facial profile.

Figure 5 Treatment progress. A. Adjustment and placement of temporary restoration on tooth #11. B. Placement of upper appliances.
At the end of orthodontic treatment, fixed appliances were removed and retainers were placed. In panoramic radiographs and lateral head films, the periodontal and endodontic health of the transplanted tooth can be identified, as well as the root integrity.
In this case, no occlusal changes were found and the irregularity index was 2 mm in the lower arch 12 years after the end of treatment. Class I relationships were achieved in molars and canines on both sides; the overjet and overbite were ideal. Long-term follow-up (12 years) of the transplanted tooth at the # 11 tooth site has remained stable and functional (Figure 6). The root of the transplanted tooth was found to have deficient cortical bone at the beginning of the treatment, so light forces were used throughout the treatment to avoid root resorption and to obtain maximum stability (Figure 7).


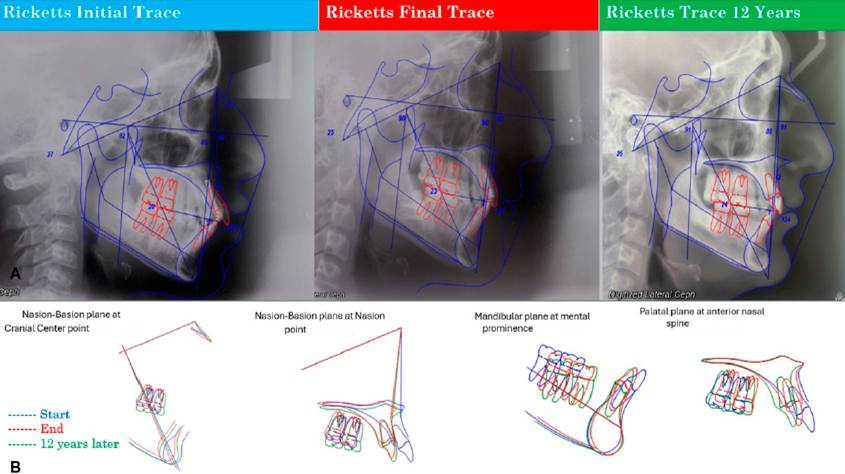
The cephalometric values for pre-treatment, post-treatment, and cephalometric evaluation 12 years after orthodontic treatment are shown in Table 1. Superimpositions between the three cephalometric tracings show changes in cephalometric measurements at the beginning of T1, T2, and T3. The post-treatment cephalometric analysis highlights the dental effects, with retroclination of the upper arch and lower incisors, and an increase in the interincisal angle. In the 12-year after treatment evaluation, no changes were observed in the position of the upper and lower incisors (Figure 8).
Discussion
Malocclusions can be treated in several ways, according to the characteristics associated with the problem, such as anteroposterior discrepancy, age, and complications of each patient26. The success of treatment in corrective Class II malocclusion in adolescents depends on the proper choice of timing and methods of therapy27. One of the treatment alternatives for these cases is to perform extractions of the upper and lower first premolars, in addition to extracting the upper right central incisor and maintaining the space for future rehabilitation with dental implants. Although it is well known that the main disadvantages of this procedure are the high cost and the time they must wait for rehabilitation23. According to Kokai20, dental transplants have a success rate of 71.0% after 5.7 years of being transplanted. In the case hereby presented, the survival is 12 years. The selection of the donated tooth, the recipient site, and the surgical technique are fundamental for the success of this therapy1-3.
Some authors agree that this technique mainly seeks function and then esthetics6-9. In this case, the proposed objectives were met. The main factors associated with the success of dental autotransplantation are the donor tooth, the recipient site, the integrity of the periodontal ligament cells of the donor tooth, the duration, the type of fixation, and the root canal treatment if necessary1,10,24,25. Consideration was also given to placing a 0.018 x 0.018” GAC brand stainless steel rigid wire splint® over the lateral incisors and upper central incisor to maintain the stability of the transplanted lower right first premolar.
After achieving the stability of the transplanted tooth, the orthodontic force was applied as suggested by Kokai20, and then extractions of the upper first premolars were performed for the correction of the horizontal and vertical overbite. For the correction of class II, extractions of the four first premolars were performed to achieve the functional objectives. In addition, one of the four premolars was considered suitable for transplantation, as suggested by Stange5 and Czochrowska6 -although for Janson21, the treatment of Class II malocclusion with four premolar extractions may present poor occlusal results due to the incomplete correction of the molar relationship in comparison with Class I. In this case, no occlusal changes were found and the irregularity index was 2 mm in the lower arch as evaluated 12 years after the end of treatment.
REFERENCES
1. Czochrowska EM Plakwicz P. Guidelines for autotransplantation of developing premolars to the anterior maxilla. Semin Orthod 2020; 26(1): 61-72. DOI: 10.1053/j.sodo.2020.01.007 [ Links ]
2. Aparicio Morales P, Brasili Esbry A, Castellón Zirpel L. Autotrasplante dentario: Revisión de literatura y casos clínicos. Rev Odont Mex. 2008; 12(4): 224-230. https://revistas.unam.mx/index.php/rom/article/download/15631/14844/18617 [ Links ]
3. Picco Díaz MI, González Rebattú y González M, Ramírez Melgoza J, López Haro ML, Hernández Chávez PI. Autotrasplante dental de canino. Reporte de un caso y revisión de la literatura. Rev Mex Cir Bucal Maxilofac. 2013; 9(3): 94-101. https://www.medigraphic.com/pdfs/cirugiabucal/cb-2013/cb133d.pdf [ Links ]
4. Vinitzky Brener I, Weihmann Sánchez EP, Aguilar Rojas AM, Peña Anaya E. Autotrasplante dental. Revisión de la literatura y presentación de dos casos. Rev ADM. 2016; 73(4): 212-217. https://www.medigraphic.com/pdfs/adm/od-2016/od164j.pdf [ Links ]
5. Stange KM, Lindsten R, Bjerklin K. Autotransplantation of premolars to the maxillary incisor region: a long-term follow-up of 12-22 years. Eur J Orthod. 2016; 38(5):508-515. DOI: 10.1093/ejo/cjv078 [ Links ]
6. Czochrowska EM, Stenvik A, Zachrisson BU. The esthetic outcome of auto transplanted premolars replacing maxillary incisors. Dent Traumatol. 2002; 18(5): 237-45. DOI: 10.1034/j.1600-9657.2002.00094.x [ Links ]
Slagsvold O, Bjercke B. Autotransplantation of premolars with partly formed roots: A radiographic study of root growth. Am J Orthod. 1974; 66(4): 355-366. DOI: 10.1016/0002-9416(74)90046-3 [ Links ]
Slagsvold O, Bjercke B. Applicability of autotransplantation in cases of missing upper anterior teeth. Am J Orthod. 1978; 74(4): 410-421. DOI: 10.1016/0002-9416(78)90063-5 [ Links ]
9. Czochrowska EM, Stenvik A, Album B, Zachrisson BU. Autotransplantation of premolars to replace maxillary incisors: a comparison with natural incisors. Am J Orthod Dentofacial Orthop. 2000; 118(6): 592-600. DOI: 10.1067/mod.2000.110521 [ Links ]
10. Bowden DE, Patel HA. Autotransplantation of premolar teeth to replace missing maxillary central incisors. Br J Orthod. 1990; 17 (1):21-28. DOI: 10.1179/bjo.17.1.21 [ Links ]
11. Di Guida LA, Collares KF, Borba M, Matias M, Benetti P. Predictors of orthodontic treatment conclusion: A historical cohort study. Am J Orthod Dentofac Orthop. 2021; 159(2): e179-e185. DOI: 10.1016/j.ajodo.2020.09.018 [ Links ]
12. Fiorentino G, Vecchione P. Multiple congenitally missing teeth: treatment outcome with autolo-gous transplantation and orthodontic space closure. Am J Orthod Dentofacial Orthop. 2007; 132(5): 693-703. DOI: 10.1016/j.ajodo.2006.05.035 [ Links ]
13. Vilhjálmsson VH, Knudsen GC, Grung B, Bardsen A. Dental auto-transplantation to anterior maxillary sites. Dent Traumatol. 2011; 27(1): 23-29. DOI: 10.1111/j.1600-9657.2010.00952.x [ Links ]
14. Paulsen HU, Andreasen JO, Schwartz O. Pulp and periodontal healing, root development and root resorption subsequent to transplantation and orthodontic rotation: A long-term study of auto transplanted premolars. Am J Orthod Dentofac Orthop. 1995; 108(6): 630-640. DOI: 10.1016/s08 89-5406(95)70009-9 [ Links ]
15. Espona Roig J, Abella F, Durán-Sindreu F, Pineda K, Alvarado Barrios C, Roig-Cayón M. Autotrasplan-te dental. Una opción terapéutica contrastada. Endodoncia. 2018; 36(3): 22-30. https://www.researchgate.net/profile/Carlos-Alvarado-Barrios/publication/331718080_Autotransplante_Dental/links/5c895cb392851c1df93ff33d/Autotransplante-Dental.pdf [ Links ]
16. Tankittiwat P, Thittiwong R, Limmonthol S, Suwannarong W, Kupradit P, Prajaneh S, et al. Mandibular premolar transplantation to replace missing maxillary anterior teeth: A multidisciplinary approach. Am J Orthod Dentofac Orthop. 2021;160(3): 459-472. DOI: 10.1016/j.ajodo.2020.06.035 [ Links ]
17. Akhlef YS, Schwartz O, Andreasen JO, Jensen SS. Autotransplantation of teeth to the anterior maxilla: A systematic review of survival and success, aesthetic presentation, and patient-reported outcome. Dent Traumatol. 2017; 34(1): 20-27. DOI: 10.1111/edt.12379 [ Links ]
18. Park JH, Tai K, Hayashi D. Tooth autotransplantation as a treatment option: a review. J Clin Pe-diatr Dent. 2010; 35(2): 129-135. https://citeseerx.ist.psu.edu/document?repid=rep1&type=pdf&doi=fcb439bcb94fcab85d575bde0bd035da30d26cea [ Links ]
19. Tovío-Martinez E, Del Valle SU, Gamarra-García, J. Autologous transplant of the mandibular third molar into a post-extraction tooth socket. Case report. Duazary. 2020; 17(4), 81-87. https://www.academia.edu/download/65041904/3603_Texto_del_articulo_11158_1_10_20201002.pdf [ Links ]
20. Kokai S, Kanno Z, Koike S, Uesugi S, Takahashi Y, Ono T, et al. Retrospective study of 100 auto transplanted with complete root formation and subsequent orthodontic treatment. Am J Orthod Dentofac Orthop. 2015; 148(6): 982-989. DOI: 10.1016/j.ajodo.2015.06.018 [ Links ]
21. Janson G, Leon-Salazar V, Leon-Salazar R, Janson M, de Freitas MR. Long-term stability of Class II malocclusion treated with 2- and 4-premolar extraction protocols. Am J Orthod Dentofac Orthop. 2009; 136(2): 154.e1-154.e10. DOI: 10.1016/j.ajodo.2009.01.020 [ Links ]
22. Freitas KMS, Massaro C, Miranda F, de Freitas MR, Janson G, Garib D. Occlusal changes in orthodon-tically treated subjects 40 years after treatment and comparison with untreated control subjects. Am J Orthod Dentofac Orthop. 2021; 160(5): 671-685. DOI: 10.1016/j.ajodo.2020.05.027 [ Links ]
23. Al-Khanati NM, Kara Beit Z. Reconsidering some standards in immediate autotransplantation of teeth : A case report with 2-year follow-up. Ann Med Surg (Lond). 2022; 75: 103470. DOI: 10.1016/j.amsu.2022.103470 [ Links ]
24. Boschini L, Plotino G, Melillo M, Staffoli S, Grande NM. Endodontic management of an auto transplanted mandibular third molar: A simplified approach. J Am Dent Assoc. 2020; 151(3): 197-202. DOI: 10.1016/j.adaj.2019.10.025 [ Links ]
25. Barrientos Sánchez S, Cardozo LA, Rojas Ruiz LM. Autotrasplantes dentales: revisión sistemática de la literatura / Autologous Dental Transplants: A Systematic Review of Literature. Univ Odontol. 2012; 31(66): 133-143. http://revistas.javeriana.edu.co/index.php/revUnivOdontologica/article/view/2721/2378 [ Links ]
26. Esquivel Alvirde A. Tratamiento de una maloclusión clase II división 1 en un paciente adulto: Reporte de un caso. Rev Mex Ortodon. 2015; 3(1): 39-46. DOI: 10.1016/j.rmo.2016.03.011 [ Links ]
27. Fang B. Diagnosis and treatment of class II malocclusion in adolescents. Zhonghua Kou Qiang Yi Xue Za Zhi. 2024; 59(9): 879-885. DOI: 10.3760/cma.j.cn112144-20240527-00220 [ Links ]
28. Janson G, Nakamura A, Barros SE, Bombonatti R, Chiqueto K. Efficiency of Class I and Class II malocclusion treatment with four premolar extractions. J Appl Oral Sci. 2014; 22(6): 522-527. DOI: 10.1590/1678-775720130544 [ Links ]
Cite as:
Martínez-Suárez G, Maldonado-Moreno JA, Tovar-Martínez ME, Mora-Canela CE, Cruz-Hervert LP. Tratamiento clase II con autotrasplante en sitio del maxilar central: Reporte de un caso. [Class II Treatment with Autotransplantation at the Maxillary Central Site: Case Report]. Rev Odont Mex. 2024; 28(3): 26-36. DOI: 10.22201/fo.1870199xp.2024.28.3.91065
Received: June 16, 2022; Accepted: October 15, 2024
 Este es un artículo publicado en acceso abierto bajo una licencia
Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia
Creative Commons
