












 (pdf)
(pdf)




 SciELO
SciELO  SciELO
SciELO 
 Permalink
PermalinkPompe disease (PD), was first described by Johannes Pompe in 1932. It is also known as acid a-glucosidase (GAA) enzyme deficiency, a severe progressive myopathy with autosomal recessive inheritance. GAA deficiency produces excessive glycogen storage in lysosomes, with secondary cell dysfunction, and progressive damage to cardiac, respiratory, skeletal, and smooth muscles. The incidence is estimated to be 1:40,000-1:300,0001,2.
The most severe form begins in the 1st months of life. It includes massive cardiomegaly, muscle hypotonia, mild hepatomegaly, and delayed motor milestone. Without treatment, these patients do not survive beyond the 1st year of life3.
The enzyme replacement therapy with recombinant human acid alpha-glucosidase is the specific treatment and is available at all ages4.
We present the case of a 5-month-old male, with positive family history for hypertrophic cardiomyopathy. The patient was diagnosed with hypertrophic cardiomyopathy at 3 months of life. The clinical presentation was characterized for dyspnea on exertion, diaphoresis, and heart failure.
The echocardiogram showed concentric biventricular hypertrophic without and decreased left ventricular function. Late intramyocardial low-septal, middle, and apex enhancement were detected in the magnetic resonance (Figs. 1 and 2). The Genetic screening reported Gene GAA variant c.1987del (p.Gln663serfs*33) compatible with PD. Fifteen days after admission, he died of ventricular fibrillation.
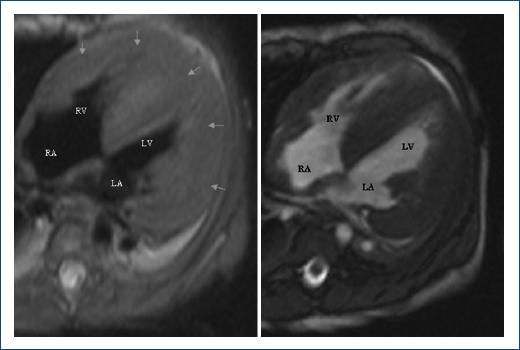
Figure 1 Magnetic resonance in four chambers shows biventricular hypertrophic cardiomyopathy (arrows). RA: right atrium; RV: right ventricle, LA: left atrium; LV: left ventricle.
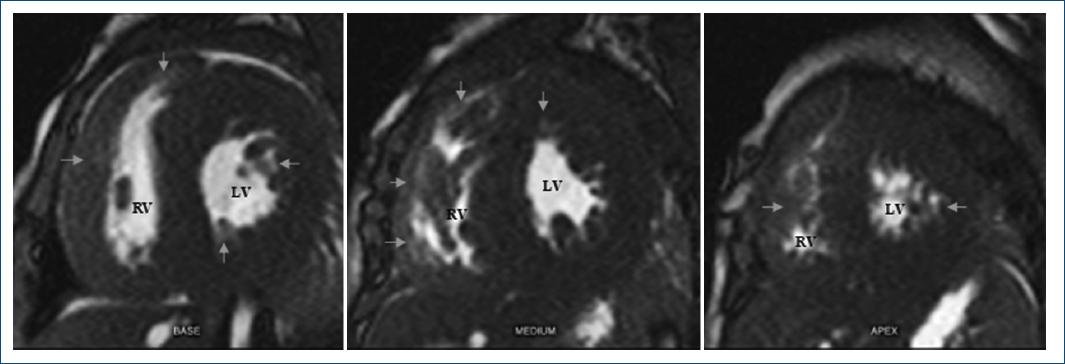
Figure 2 Magnetic resonance images in short-axis plane, present cardiomyopathy with late low, middle, and apex intramyocardial enhancement (arrows). RV: right ventricle; LV: left ventricle.
Performing timely detection is vital for patient survival, with the current support of imaging studies and genetic tests, the diagnostic is achieved. We suggest monitoring patients and performing interventions to avoid complications. Treatment is available in Mexico, so prompt action must be taken.

