











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Univentricular physiology includes a series of cardiac malformations that result in systemic and pulmonary circulation depending on a single ventricular cavity (right, left or indeterminate ventricle), and there is usually a small accessory chamber that functions exclusively as a reservoir. According to the morphology of the systemic ventricle, ventricular failure will be earlier, as well as the presence of arrhythmias that can lead to deterioration of the functional class and death.1
Congenital heart defects are the most common congenital disorders, with an incidence of 1:100 in live newborns.2 The univentricular heart is a pathology with very low prevalence within congenital heart defects, a group of anomalies in the heart’s structure after a poor development that results in a single ventricular chamber. There are different types of morphologies depending on the dominant ventricle: right ventricle (50-57%), left ventricle (42-43%) or indeterminate type (0-2%).1,3 This anatomical change also has functional changes, including volume overload in the ventricle, a decrease in systemic oxygen saturation, and even non-restrictive systemic pressure flow increases the pressures of the pulmonary vasculature.4 The management of these patients is surgical at an early age, generally with the Fontan procedure, improving the survival of these patients. However, there is very little information about its medical management in adults.2
Case presentation
Important background
28-year-old man, known since his first year of life with cyanogenic congenital heart disease of the univentricular heart type with undetermined morphology with a double outflow tract, not having pulmonary restriction and developed pulmonary arterial hypertension, with a PAP of 41 mmHg and a PAWP of 35 mmHg, without previous measurements at the time of diagnosis. Therefore, it was not considered a candidate for corrective or palliative surgery and was maintained with medical treatment. Since he was 12 years old, he developed polyglobulia and has been monitored with a frequent saline exchange. So far, the patient has not presented complications that threaten the patient’s life.
Clinical presentation
The patient went to the cardiology department for a follow-up of single ventricular congenital heart disease. He referred to dyspnea (NYHA grade II/CG-WHO II) and intermittent headache. On admission, vital signs with a heart rate of 82 beats per minute, respiratory rate of 18 breaths per minute, blood pressure of 90/60 mmHg, temperature of 36.5 oC and oxygen saturation of 90% on room air.
Physical examination reveals a conscious and oriented patient with conjunctival hyperemia, jugular plethora (grade I), sustained apical impulse, displaced to the sixth intercostal space in the left anterior axillary line, pansystolic and diastolic murmur predominantly in the pulmonary area (Harvey-Levine classification IV/VI), S2 unfolded and reinforced in P2, in plateau configuration, irradiated to the left mid-axillary line, with tactile fremitus, in the thoracic and pelvic limbs with the presence of clubbing (Figure 1).

Clinical studies and imaging test
The electrocardiogram showed sinus rhythm, with a heart rate of 82 beats per minute and a deviated QRS axis to the right, with a wide and notched P wave in DI and the second negative P wave component in V1 suggesting left atrial growth. In DII, the P wave is acuminate, which suggests right atrial growth. Large voltages are also observed in the QRS complex, which can be measured in V2 with an R wave of 9 mV and an S wave of 43 mV, suggesting both ventricular hypertrophy, and systolic and diastolic overload. Analyzing the same QRS complex, the Katz-Wachtel sign is observed, characterized by voltages ≥ 50 mm in the intermediate precordial leads, generally observed when there is a ventricular septal defect (Figure 2).
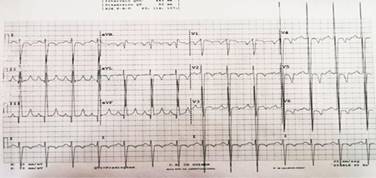
Figure 2: 12-lead electrocardiogram suggesting atrial chamber enlargement, ventricular enlargement and overload.
The transthoracic echocardiogram shows a single ventricle (Figure 3) that reveals a maximum ventricle dimension of 11 cm in diastole, a ventricular wall thickness of 2.02 cm, without abnormalities in its segmental mobility, with an absence of interventricular septum. Both atria were 5.7 cm, with moderate mitral and tricuspid valve regurgitation corroborated with the doppler effect. Dilatation of the root of the pulmonary artery of 4.49 cm, with pulmonary valve regurgitation, also corroborated with the Doppler effect. The chest X-ray shows grade III cardiomegaly, with a cardiothoracic index of 0.63 at the expense of the left profile, and with data that suggests PAH, such as a notably dilated arch of the pulmonary artery (Figure 4). Prior to this, right heart catheterization was performed at 17-years-old, where a PAP of 41 mmHg and a PAWP of 35 mmHg were found.

Figure 3: Transthoracic echocardiography with large single ventricle and myocardial hypertrophy evidence. A) Shows the single ventricle and its large dimensions; B) and C) show the right and left atrial, respectively, also with large dimensions.

Treatment
The patient is currently receiving pharmacological therapy with captopril 12.5 mg every 12 hours, digoxin 0.25 mg every 24 hours, sildenafil 20 mg every 8 hours and spironolactone 25 mg every 24 hours as a diuretic. He is also given supplemental oxygen with nasal prongs at 3 L/min as ambulatory management. In addition to this, he is given saline pheresis every 3 or 4 months. This procedure was done by placing the patient in a semi-fowler position, canalizing with a 0.9% saline solution with 500 cm3 for 4 hours and nasal prongs placed with oxygen at 3 L/min. Subsequently, approximately 700 mL of blood was drawn, the patient was observed, and vital signs were monitored every hour until discharge.
Discussion
The single ventricle is a complex congenital cardiac pathology of low incidence, found in approximately 1.5% of individuals with congenital heart disease.5 In a cohort study conducted in Wales and England between 2000 and 2018, among 53,615 patients born who went under intervention for complex congenital heart disease, only 3% had univentricular heart disease.6 This can have univentricular variations and typical characteristics, among which are: hypoplastic left heart syndrome, tricuspid atresia, Ebtein’s anomaly, double outlet right or left ventricle, or an atrioventricular canal defect.7 Right ventricular hypoplasia is the most common form of the single ventricle, seen in 2:10,000 births, with a higher incidence in men.8 When there is no early surgical intervention in the first three years of age, survival at 14 years is 50% in carriers of single ventricle left ventricle carriers and at four years in 50% of patients with ventricular indeterminate.2,9
Depending on the physiology of the single ventricle, a series of palliative surgical procedures is required. The first stage is the Norwood procedure performed in the first week of life, which consists of reconstructing the aortic arch at the right ventricle outlet, creating a stable and restrictive pathway for blood flow either from the systemic artery or from the functional ventricle. The second stage is the Glenn procedure between three and five months of age, which consists of removing the aortic shunt and performing an anastomosis of the superior vena cava to the pulmonary artery. The third and final stage is the Fontan procedure, which consists of anastomosis of the inferior vena cava to the pulmonary artery and a fenestration between the right atrium and the inferior vena cava, to reduce the load on the single ventricle.1 This procedure has an operative mortality of less than 5%, and the 30-year survival rate is 85%.2,9 Over time, the Fontan circulation impacts other systems by increasing systemic venous pressure, mainly resulting in hepatic congestion. However, the main causes of mortality change by not having a surgical process in patients with a single ventricle, the main ones being heart failure at an early age or arrhythmias.
The clinical presentation of a single ventricle will depend on its morphology since there may be a decrease in pulmonary outflow (Qp), differences in pulmonary vascular resistance (Rp), aortic obstruction, different functionality in the valves atrioventricular and right, left or indeterminate ventricular morphology. Pulmonary obstruction and Rp will determine Qp, which will impact the presentation of heart failure, complications and the patient’s prognosis.10 For example, patients with severe pulmonary obstruction will reduce Qp, leading to severe heart failure; in patients with moderate pulmonary obstruction, the Qp is near normal, and therefore heart failure may be mild. On the other hand, in patients without pulmonary obstruction, the Qp will depend on the Rp; if the Rp is low, the heart failure will be severe, but if the Rp is high (for example, in the Eisenmenger effect), as is the case with our patient, the heart failure will not be as severe, and survival will be greater.11,12
The aforementioned drugs have a specific reason for which they are administered, as the increase in diuresis, the improvement of cardiac output and the decrease in pulmonary pressures have contributed to lengthening the time of cardiac remodelling.
Currently, the patient is a professional. He goes every two months for a physical examination and laboratory tests, including hematology, renal and liver function. However, the patient has decided not to go to cardiac rehabilitation.
Conclusions
Unfortunately, being a rare congenital heart disease in adults, there are few references about medical management in this age group. It is necessary to develop and broadcast strategies for an early diagnosis, as a principal objective to identify pediatric patients with cardiovascular diseases, who’s, upon suspicion of a cardiovascular problem are references in time for a follow and treatment which improves the expectation and quality of life. If they are not managed during childhood, it is necessary to refer these types of patients for specialized follow-up of their underlying pathology, and the work of a multidisciplinary team to prevent aggravation or damage to other systems.

