











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
Right coronary artery (RCA) absence is a rare congenital cardiovascular malformation with few cases reported in the literature.1-3 Congenital absence may result from agenesis or congenital occlusion of the RCA during embryonic development. It has also been shown to be associated with congenital heart disease.1 In most cases, the congenital absence of the RCA is asymptomatic. However, a small proportion of these patients develop life-threatening clinical complications, including acute myocardial infarction, stroke, or sudden death.3 The absence of RCA with chronic total occlusion (CTO) of the left coronary artery is extremely rare.
We present the case of a Mexican patient with a history of exercise-induced chest pain in which a congenital absence of RCA with CTO was confirmed by selective coronary angiography (CAG).
Case presentation
A Mexican man of 80 years old was admitted to our hospital following six months of exercise-induced chest pain. The chest pain was retrosternal, oppressive, lasting two minutes, and waned with rest. Over the past two months, he experienced an increase in the intensity and frequency of chest pain episodes. The patient denied any history of chronic diseases, including cardiovascular disease or a family history of coronary heart disease. A physical examination revealed a body temperature of 36.5 oC, a pulse rate of 86 beats per minute, a breathing rate of 20 breaths per minute, a blood pressure of 104/69 mmHg, and a body mass index of 28.5 kg/m2. There were no abnormal findings during the cardiac examination. It was decided to admit the patient for further investigation and treatment.
The electrocardiogram showed sinus rhythm, inversion of T wave in leads aVL, V2, and V3 with Q waves in lead aVR (Figure 1). In laboratory tests, a creatine kinase-MB (CK-MB) level of 7 IU/L was found (reference range, 0-10 IU/L) (Table 1).
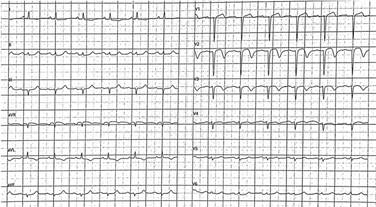
Figure 1: 12-lead electrocardiogram: sinus rhythm and inversion of T wave in leads aVL, V2, and V3 with Q waves in lead aVR.
Table 1: Laboratories on admission to hospital.
| Value | Reference range | |
|---|---|---|
| Leukocytes, [mm3] | 8,390 | 5,000-10,000 |
| Platelets, [mm3] | 220,000 | 130,000-400,000 |
| Hemoglobin, [g/dL] | 14.3 | 14-18 |
| Sodium, [mEq/L] | 138 | 136-145 |
| Potassium, [mEq/L] | 4.45 | 3.5-5.1 |
| Chlorine, [mEq/L] | 106 | 98-117 |
| Phosphorus, [mg/dL] | 3.2 | 3.7-7.2 |
| Calcium, [mg/dL] | 9.3 | 8.6-10.6 |
| Magnesium, [mg/dL] | 2.1 | 1.9-2.7 |
| Glucose, [mg/dL] | 94 | 74-106 |
| Creatinine, [mg/dL] | 0.94 | 0.7-1.3 |
| Urea, [mg/dL] | 48.79 | 18-50 |
| Blood urea nitrogen, [mg/dL] | 22.8 | 9-23 |
| Total creatine kinase, [IU/L] | 59 | 21-232 |
| Creatine kinase-MB, [IU/L] | 7 | 0-10 |
| Triglycerides, [mg/dL] | 160 | 0-150 |
| Total cholesterol, [mg/dL] | 99 | 100-200 |
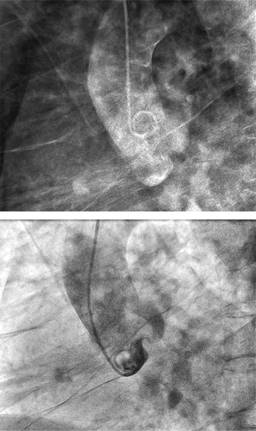
The coronary angiography revealed a CTO in the middle of the left anterior descending artery with a congenital absence of the right coronary artery and ectasia in the left circumflex artery, resulting in three posterolateral arteries and the posterior descending artery (Figures 2 and 3).

Figure 2: Coronary angiography: chronic total occlusion of the middle segment of the left anterior descending artery, the ectatic left circumflex artery in the proximal portion giving rise to three posterolateral arteries, subsequently originating posterior descending artery. A) Left anterior oblique view. B) Right anterior oblique caudal view. C) Left anterior oblique cranial view. D) Left anterior oblique caudal view.
The patient was then offered only symptomatic treatment. The patient was prescribed aspirin, atorvastatin, and metoprolol during his hospitalization. Hospitalization was uneventful. On the day of discharge, he was symptom-free and has continued to be symptom-free for the duration of his follow-up treatment.
Discussion
Coronary arteries develop in two stages during embryonic development. First, endothelial cells derived from venous sinuses form immature primary coronary vascular networks in the subepicardial and myocardial layers. Second, epicardial cells undergo an epithelial-mesenchymal transition to produce smooth muscle cells and fibroblasts, which are then remodeled to create a mature cardiac artery system. Coronary artery anomalies are the result of abnormal embryonic development.1,4,5
In 1882, Hyrutle published the first report of a single coronary artery in an autopsy study.6 According to Smith, it is an isolated coronary artery that arises from the aortic trunk and supplies the entire heart regardless of location.7 White and Edwards first described the congenital absence of the RCA in 1948.8 A prevalence of 0.014 to 0.066% has been reported in the literature for the congenital absence of RCA.1 At the time of diagnosis, the mean age of patients with congenital absence of RCA is 53 years, with 54 percent being females and 87% without any associated congenital heart defects.3
The angiographic classification of a single coronary artery was first proposed by Lipton in 1979 and is now widely used in clinical practice. It is first separated into types R and L based on the location of the coronary artery’s origin (right or left coronary sinus). Secondly, it is classified into groups I, II, and III according to its anatomical distribution of branches. In group I, one coronary artery extends to supply the heart that the contralateral coronary artery should have supplied; in group II, a single coronary artery that has transverse branches that extend to supply the heart that the contralateral coronary artery should have supplied; in group III, an LCX and LAD branch arise separately from the trunk of a coronary artery. Lastly, according to the route taken by the large transverse trunk as it crosses the base of the heart to reach the normal contralateral coronary artery, it is classified into three groups regarding the aorta and the pulmonary artery: A (anterior), B (between), and P (posterior).9 It has been reported that the L-I pattern is more likely to occur than the L-II pattern.3 In accordance with Lipton’s classification, this patient is classified as a type L-I.
Clinical manifestations vary; most patients present with symptoms of myocardial ischemia, such as angina pectoris, chest tightness, palpitations, and atypical chest pain. Symptoms such as these are caused by arterial stenosis and obstruction. It is important to note that the electrocardiogram manifestations vary and are non-specific; approximately half of these patients will have left coronary artery branch lesions, and approximately 60% will have ST-T changes; other findings include sinus bradycardia, third-degree atrioventricular block, or atrial fibrillation.10
The CAG remains the gold standard for diagnosing congenital absences of the RCA and is widely used in clinical practice. Nevertheless, it often confuses the operator during angiography, resulting in repeated non-standard angiographic projections, rapid consumption of contrast medium, a prolonged procedure time, and an increased risk of complications.3 CT angiography is a noninvasive examination commonly used for diagnosis, treatment, and follow-up; it can also detect anatomical variations in the cardiovascular structure and discover other cardiac conditions.10
As few cases have been reported, there are no standardized treatment guidelines for patients with single coronary arteries. However, medical therapy with anti-platelets, anti-coagulation, lipid-lowering agents, and revascularization therapy, including interventional or surgical procedures, are available as treatment options.1,2,3,10 The percutaneous coronary intervention (PCI) of CTO lesions has drawn considerable interest recently. The procedure, however, is technically challenging, and the complication rate is higher than when PCIs do not involve CTOs. Moreover, there are minimal data from randomized controlled trials comparing CTO-PCI with medical therapy. Most studies examining PCI outcomes for CTO are either observational single-center or multicenter registries. Clinical trials have not demonstrated an improvement in ventricular function, a difference in symptoms, or clinical outcomes with CTO PCI compared with optimal medical care. Therefore, all patients with CTO should receive optimal guideline-directed medical therapy, and revascularization should be considered only for those with refractory angina despite medical therapy and for whom benefits exceed the potential risk of the procedure.11,12
Conclusions
In the literature, there are a limited number of reports of congenital absence of RCA, which can sometimes lead to life-threatening complications. The absence of RCA with CTO of the left coronary artery is a rare condition. This case illustrates the importance of coronary angiography for diagnosis, which is considered the gold standard. Treatment options include conservative or revascularization therapy; in this case, we used antiplatelet and lipid-lowering agents without any symptoms during follow-up. Due to its extremely low incidence, it is difficult to determine the prognosis of this coronary anomaly. Further studies are needed to determine this condition’s most appropriate treatment and prognosis.

