











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
The first paraganglioma (of the carotid body) was described by Marchand in 1891 and it was not until 1955 that Balnchard and Saunders reported the first laryngeal paraganglioma1,2.
Generically called "paraganglioma" is those tumors of neuroendocrine origin of chromaffin cells in the paraganglia of the sympathetic and parasympathetic nervous system regardless of their location, which can comprise any part of the economy, the most common being: carotid body, jugular foramen, middle ear, aorticopulmonary region, posterior mediastinum, and abdominal paraortic region including organ of Zuckerkandl (clusters of neuroendocrine tissue in the posterior thoracoabdominal and paravertebral area), the only exception being the adrenal medulla which is called pheochromocytoma1.
Head and neck paragangliomas are rare, more frequently benign, with a slow growth pattern and non-secreting, of these, laryngeal paragangliomas are particularly rare, originating from paraganglionic cells within the supraglottis or subglottis, of which there have been reported around 76 cases3. These laryngeal tumors of non-epithelial neuroendocrine origin, although they are usually benign in nature, can metastasize to lung, liver, bone, and skin lymph nodes (extremely rare)4.
Given their origin in the neural crest, paragangliomas can arise along the migratory routes of said tissue, with their normal distribution being neurovascular structures5. Most paragangliomas are solitary and arise sporadically, they can be multicentric and their family occurrence is well-recognized (40% of head and neck paragangliomas are associated with a hereditary predisposition and 60% arise sporadically)5, so given the character of autosomal dominant transmission with incomplete penetrance, a meticulous family history is necessary1.
Paragangliomas are found in association with multiple endocrine neoplasms (MEN IIA and IIB) and neuroectodermal syndromes (tuberous sclerosis, neurofibromatosis, and Von Hippel–Lindau disease). Paragangliomas can occur as part of Cartney's triad (gastric leiomyosarcoma, pulmonary chondroma, and extra-adrenal paraganglioma)1.
Paragangliomas have the same morphological characteristics, regardless of the anatomical site of presentation. The histological findings are characterized by the presence of stem cells in a "Zell Balen" nest configuration (polygonal main cells surrounded by elongated fibrous sustainable cells) are usually hypervascular with conjugates with typical vascular channels of this type of tumor with great vascularity1,2.
Chromogranin is a protein structure within stem cells specific to neuroendocrine tumors. The S100 protein is a specific marker that in combination with chromogranin demonstrates the biphasic cellular behavior of paragangliomas1.
Epidemiology
The global incidence of head and neck paragangliomas is 1: 30,000 to 1: 100,0005, of all cases, familial paragangliomas constitute 10% and 35-50% of these are multicentric1. The location of the paragangliomas is 80% abdominal, 12% thorax, and 3% in the head and neck. In total terms, 90% of the cases correspond to pheochromocytoma and of the remaining 10%, 75% are located in the aorta (Zuckerkandl organ), 10% chest, 10% bladder, and only 5% head and neck1.
Head and neck paragangliomas are closely related to the parasympathetic nervous system, the most common being those of the carotid body, followed by lesions of the jugular foramen, middle ear, and vagus nerve. Less common locations are the orbit, nasal cavity, thyroid, pituitary, and larynx1. Laryngeal paragangliomas contribute 0.6% of laryngeal tumors emanating from the superior paraganglia (located in the false vocal cord, associated with the superior laryngeal nerve and artery) or inferior (located near the lateral margin of the cricoid cartilage in the cricotracheal membrane, associated with the recurrent laryngeal nerve). Most laryngeal paragangliomas have a supraglottic location and only 3% have a glottic location6. Laryngeal paragangliomas can present at any age, being older between the fourth and sixth decades of life (mean age 44 years), having a male-female ratio of 3:1, respectively.
Clinic and diagnosis
Hormonally functioning paragangliomas secrete catecholamines conditioning sudden hypertension, headache, sweating, anxiety, flushing, and hyperthermia during seizures1, it should be noted that laryngeal paragangliomas are usually non-secreting. The symptoms of non-functioning paragangliomas are consistent with the size of the tumor mass, and may or may not be painful, and 10% of paragangliomas are clinically silent of incidental detection1. In laryngeal paragangliomas, the symptoms depend on the location of the tumor, which generally includes dysphonia, dysphagia, stridor, or a foreign body sensation. Although these tumors occur in a wide variety of anatomical locations, computed tomography (CT) images have almost identical characteristics, such as soft-tissue masses with well-defined contours with homogeneous or heterogeneous enhancement in the presence of necrosis and hemorrhage1,7 and in the case of Laryngeal paragangliomas, a laryngoscopy is essential.
Laboratory tests can aid detection by determining catecholamines and their metabolites in plasma and urine; vanilmandelic acid will be twice above the normal value (VN: 2-10 mg/24 h); urinary and serum norepinephrine will be eight times the normal value > 2,000 Pg/ml; chromogranin at levels of 111 ng/ml (VN: 143 ng/ml)1. Arteriography is useful to define the tumor extension, the mass effect, the proximity to important vessels, and the degree of collateral circulation for the purpose of meticulous surgical planning7, so in the presence of hypervascular masses, the possibility of a paraganglioma should always be considered also considering the autosomal dominant character when having a family history of paraganglioma1. Radionucleotide techniques (indium-labeled pentetreotide or iodomethabenzylguanidine) are reserved in cases of diagnostic doubt, follow-up, and synchronous lesions7. Octreotide examination can further confirm the diagnosis, and urine collection of catecholamines and metanephrines can identify vasoactive secretory tumors. As a complementary test, fine-needle aspiration-puncture is a controversial indication technique; classically, it has been contraindicated due to the risk of bleeding7, although with endolaryngeal microsurgical methods, it can be considered with greater safety in case of suspected malignancy.
The differential diagnosis should rule out other endolaryngeal submucosal masses such as carcinoid tumors, small cell tumors, or medullary thyroid carcinoma7.
Results
We present the case of a 68-year-old female patient with a history of dysphonia, foreign body sensation, and dysphagia of 8 months of evolution associated to episodes of bronchoaspiration, being evaluated by the otolaryngology service who performs flexible nasolaryngoscopy observing glottic tumor that occupies arytenoid without If possible observation of the vocal cords (Fig. 1) managed with prednisone 50 mg every 24 h without improvement in symptoms, a biopsy is taken by laryngoscopy whose histopathological report concludes the presence of epidermoid metaplasia, for which it is scheduled for tumor resection by the otorhinolaryngology service who, due to significant bleeding during laryngoscopic resection, performs only partial resection of said tumor whose pathology report indicates tissue compatible with paraganglioma with chromogranin immunohistochemistry: (+) focal, enolase NE: (+) Diffuse, S-100: (+) in supporting cells, confirming the diagnosis of laryngeal paraganglioma. Hence, he decided to send it to the oncosurgery service.
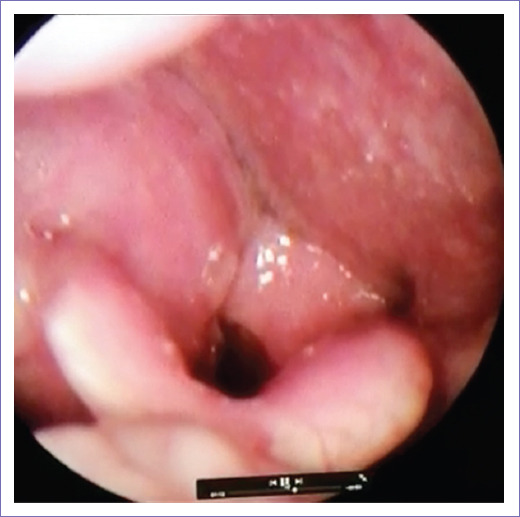
Figure 1 A glottic tumor that occupies arytenoid without being possible to observe the vocal cords, corresponding to a paraganglioma.
Our service assesses the patient 9 months after her first visit to this unit, requesting a cervical CT scan showing a 27 × 25 × 25 mm tumor superior to the right side thyroid cartilage that conditions a 3 mm narrowing of the airway (Fig. 2). It is scheduled for tumor resection through the anterior open approach, which is completely resected, with a satisfactory evolution 3 months after the procedure.

Discussion
Laryngeal paragangliomas are exceptional neuroendocrine tumors whose origin is the neural crest (3-5% of paragangliomas are located in the head and neck). The diagnosis should begin with a thorough anamnesis and physical examination, including family history (since germinal susceptibility is around 40%), fiberoptic laryngoscopy, and CT images, with the possibility of adding magnetic resonance imaging. In our case, the patient had a glottic laryngeal paraganglioma, which makes it extremely rare (3% of laryngeal paragangliomas). On histological examination, the main and support cells in these neoplasms are immunoreactive to staining of neuroendocrine markers such as chromogranin and synaptophysin, but not epithelial markers such as cytokeratin, as well as the classic "Zell Balen" nest configuration3.
The presenting symptoms associated with laryngeal paraganglioma include hoarseness, dysphagia, dyspnea, or a foreign body sensation, the same characteristics that our patient presented3.
Therapeutic techniques include laryngoscopic excision, which was not possible in this patient given the significant tumor bleeding (a complication widely described in the literature) and open resection using a transcervical approach. Endoscopic techniques are indicated in small lesions; however, they are associated with high rates of recurrence; In contrast, open techniques allow excellent access to dissection in the submucosal plane, favoring better exposure and less damage, as well as direct control of the vascular supply, which is why it was the best option in this case considering the history of bleeding and to a great extent tumor size.
Conclusion
Paragangliomas are extremely rare tumors, and particularly laryngeal paragangliomas are among the rarest. These tumors have an important hereditary component, so the family history must always be kept in mind. The symptoms of laryngeal paragangliomas are quite nonspecific and mostly silent, presenting with dysphagia, stridor, dysphonia, or a foreign body sensation. The CT images as well as the histopathological report with immunohistochemistry establish the diagnosis. Curative treatment consists of surgical resection and the prognosis is directly linked to its quality, being excellent with complete resection, granting a low risk of recurrence.

