











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
Gallstone ileus is a mechanical obstruction of the intestine caused by the impaction of a gallstone in the gastrointestinal tract. This is due to a cholecystoenteric fistula more frequently in the ileum (60%) and secondly in the colon1,2. It is a rare complication of cholelithiasis, accounting for 1-4% of the causes of intestinal obstruction and occurring in 0.3-0.5% of cases of cholelithiasis3. The case, diagnostic and therapeutic approach in a patient with gallstone ileus from northeastern Mexico.
Case Report
The patient is a 69-year-old female with no history of chronic degenerative diseases with a history of umbilical plasty without mesh 15 years ago, smoking 20 packs/year, and no previous hospitalizations. She came to the consultation with a 6-day history of moderate cramping abdominal pain, progressive in the epigastrium that later became generalized, accompanied by nausea, vomiting, and constipation. She came to our unit for presenting 6 episodes of vomiting 24 hours prior to her admission with fecaloid characteristics. On physical examination, she was hemodynamically stable, neurologically intact, with signs of dehydratation. The abdomen was distended with abscence of peristalsis, a soft abdomen with diffuse pain on deep palpation, without signs of peritoneal and tympanic irritation on percussion. The rectal examination was normal.
In the laboratories without alterations except a creatinine of 3.67. The x-ray (Fig. 1) and simple abdominal tomography evidence a hyperdense image in the intestine (Fig. 2).
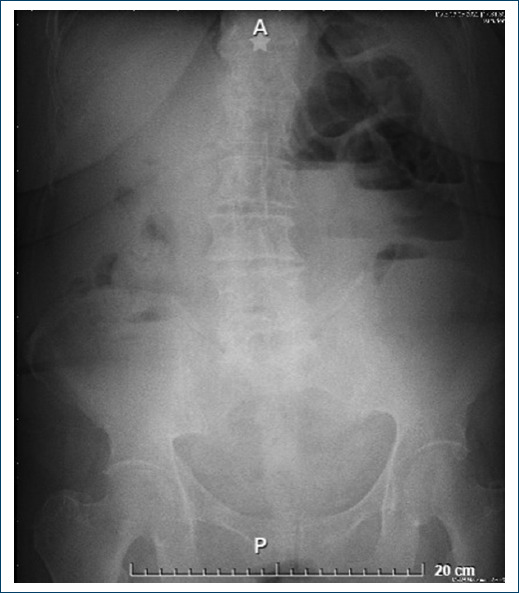

Figure 2 Simple abdominal CT shows a calcified mass in the intestine, without the presence of pneumobilia. A: axial. B: coronal section.
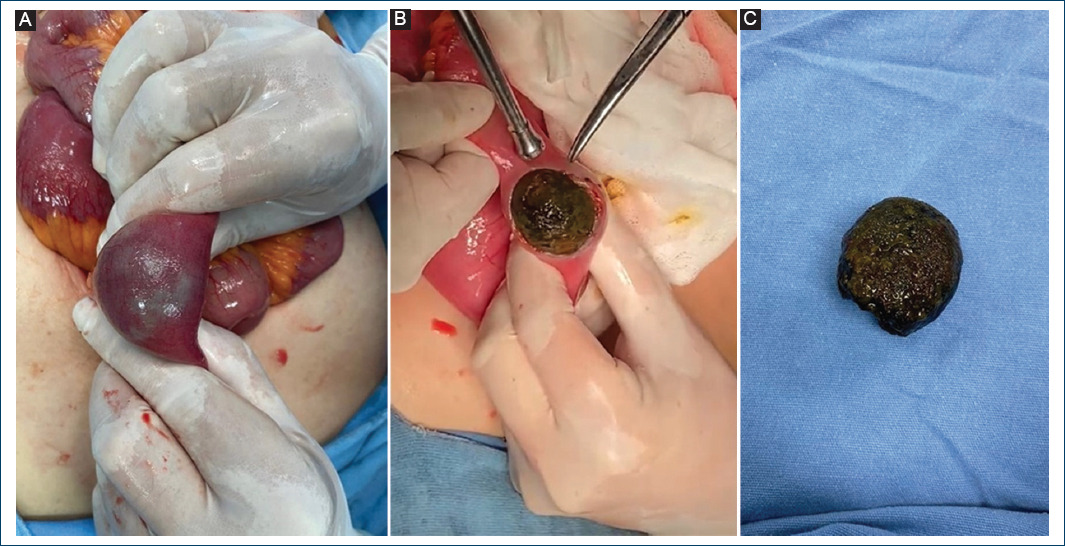
In the exploratory laparotomy, dilated intestinal loops were found 200 cm from the ileocecal valve. A longitudinal enterotomy was performed and a stone was removed that occludes 100% of the intestinal lumen, a site of occlusion without vascular compromise (Fig. 3). Subsequently, repair is performed in 2 planes, the first with 3-0 Connel Mayo vicryl and the second with 3-0 Lembert silk. The rest of the intestine and colon are explored without finding more stones. With adequate postoperative evolution, he was discharged home on the fifth postoperative day.
Discusion
Gallstone ileus is often preceded by an episode of cholecystitis. Inflammation in the gallbladder conditions the formation of adhesions. The gallbladder wall erodes under the effect of stone pressure and inflammation, causing the formation of a fistula between the gallbladder and the adjacent gastrointestinal tract, with subsequent passage of a gallstone. Less frequently, the stone may enter the duodenum through a dilated toilet papilla. Other causes of gallstone ileus are: complication of an ERCP or endoscopic sphincterotomy and the consequence of loose stones in the abdominal cavity after a laparoscopic cholecystectomy, although these are very rare cases4,5.
The duodenum is the most frequent site of origin of the fistula in 75 to 83% of cases due to its proximity to the gallbladder. However, the stomach, small intestine, and colon may be involved. The gallstone can spontaneously pass through the rectum, or become impacted and cause intestinal occlusion. Stones <2.5 cm mostly pass spontaneously without causing obstruction. Multiple stones have been reported in 3–40% of gallstone ileus cases. The most frequent site of impaction is the ileum (50 to 60%), jejunum (16 to 27%), duodenum (3.5 to 14.6%), and colon (3 to 4%), in that order. If the patient with gallstone ileus is not treated early, it can cause ischemia due to the pressure generated from distension, stone and inflammation. With subsequent perforation and peritonitis, with a mortality of 12 to 27% when it is not diagnosed in a timely manner4,5.
Up to 50% of patients with gallstone ileus have no history of gallbladder disease. Other related causes are previous gastric surgery, cholecystectomy, abdominal trauma.3,6 Our patient had no significant prior history.
Due to the insidious and non-specific presentation of signs and symptoms in patients with gallstone ileus, the diagnosis is delayed. Imaging studies have a crucial role in diagnosis. Radiography has a low sensitivity and specificity, Riegler’s triad (aerobilia, dilated loops and ectopic stone) is observed in only 15% of cases. In the CT scan, 96% show signs of intestinal obstruction, 88% pneumobilia, 14% air in the gallbladder, ectopic stones are observed in 81%, fistula is only detected in 11% and Riegler’s triad in a 77% of the cases. CT can define the site of obstruction and help in making therapeutic decisions, being the imaging study of choice2,5.
There are 3 options for surgical management of these patients (one-stage surgery, two-stage surgery, and only enterolithotomy). One-stage surgery consists of performing enterolithotomy, cholecystectomy, and closing the fistula. In two-stage surgery, cholecystectomy and fistula closure is performed 4-6 weeks after enterolithotomy. Currently, the management of choice is enterolithotomy, due to the high morbidity and mortality of one and two-stage surgery. The recurrence of gallstone ileus after enterolithotomy is 5-9% and complications are rare, due to the spontaneous closure of the fistula in most cases. The stone can be removed by colonoscopy, laparoscopic and open surgery1,6. Endoscopy is reserved for patients with high surgical risk where the stone can be reached by this means5.
Conclusion
Gallstone ileus is a rare cause of intestinal obstruction. The clinical picture is intestinal obstruction without characteristic data, the diagnosis is with a detailed analysis of the imaging studies. The diagnosis is confirmed in the intraoperative period. The imaging study of choice is CT and the treatment is enterotomy. Fistula repair and cholecystectomy are only performed in patients with justified indications.

