










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkSanus
On-line version ISSN 2448-6094
Sanus vol.8 Sonora Jan./Dec. 2023 Epub Sep 25, 2023
https://doi.org/10.36789/revsanus.vi1.403
Investigation
Relation of self-efficacy to weight control and resilience in Mexican women
1
 http://orcid.org/0000-0002-9997-9903
http://orcid.org/0000-0002-9997-9903
2
*
http://orcid.org/0000-0002-7626-8949
1Profesor Investigador, Posgrados en Enfermería, Universidad Popular Autónoma del Estado de Puebla, México.
2Profesor Investigador, Departamento de Salud Pública y Ciencias Médicas, Facultad de Medicina, Universidad Autónoma de San Luis Potosí, México.
3Profesor Investigador, Facultad de Enfermería, Benemérita Universidad Autónoma de Puebla, México.
4Profesor Investigador, Facultad de Enfermería, Benemérita Universidad Autónoma de Puebla, México.
Introduction:
Currently, obesity has become an emerging and complex public health problem whose mechanism is etiopathogenetic and multifactorial. Obesity has been studied from the biomolecular and genetic approach as well as through interventions to improve lifestyles. However, studies linking the concepts of self-efficacy and resilience have not been included in this issue.
Objective:
Evaluate the relationship between self-efficacy for weight control and resilience in Mexican women.
Methodology:
Correlational-cross-sectional study in 174 women, with or without obesity, enrolled in a job-training center of Puebla and San Luis Potosi, Mexico; non-probabilistic sampling was used. These two instruments Self-Efficacy Inventory for Weight Control and Mexican Resilience Scale, validated in the Mexican population were applied: with Cronbach's alpha .945 and .950, respectively. This study carried out in accordance with the General Health Act for Research. The results were analyzed using descriptive statistics, normality tests, and Spearman's r correlation.
Results:
The mean age was 34.6±14.7, mean BMI 26.4±4.5, 49.7% and 81.7% were high levels of self-efficacy and resilience, respectively. The relationship was positive, medium effect size and statistically significant p=.001, with an explained variance of 22.6%.
Conclusions:
The Mexican women shown that the greater the resilience, the greater the self-efficacy for weight control. We suggest integrating resilience in managing obesity, which allows the development of mechanisms for the acquisition of more sustainable healthy lifestyles.
Key words: Self-efficacy; resilience; weight control; women; nursing (DeCS)
Introducción:
Actualmente la obesidad se ha convertido en un problema de salud pública emergente y complejo, cuyo mecanismo es etiopatogénico y multifactorial. Ha sido estudiada desde el enfoque biomolecular, genético y mediante intervenciones para mejorar los estilos de vida; sin embargo, no se han incluido estudios que relacionen la autoeficacia y resiliencia en este problema.
Objetivo:
Evaluar la relación de autoeficacia para el control de peso con la resiliencia, en mujeres mexicanas.
Metodología:
Estudio correlacional transversal, en 174 mujeres, con o sin obesidad, inscritas en un centro de capacitación para el trabajo en Puebla y San Luis Potosí, México, se empleó muestreo no probabilistico. Se aplicó el instrumento validado en población mexicana: Inventario de Autoeficacia para el control de peso y Escala de Resiliencia Mexicana; con alfa de Cronbach .945 y .950 respectivamente; estudio realizado con apego a la Ley General de Salud en materia de investigación. El análisis de los resultados fue con estadística descriptiva, pruebas de normalidad y correlación r de Spearman.
Resultados:
El promedio de edad fue 34.6 ± 14.7, media de IMC 26.4 ± 4.5, un 49.7 % y un 81.7 % obtuvo niveles de autoeficacia y resiliencia altos respectivamente. La relación fue positiva, tamaño de efecto medio y estadísticamente significativo p=.001, con una varianza explicada del 22.6%.
Conclusiones:
Las mujeres mexicanas mostraron que a mayor resiliencia mayor autoeficacia para el control de peso. Se sugiere integrar la resiliencia en el manejo de la obesidad, que permita el desarrollo de mecanismos para la adquisición de estilos de vida saludables más sustentables.
Palabras clave: Autoeficacia; Resiliencia; Control de peso; Mujeres; Enfermería (DeCS)
Introdução:
Atualmente, a obesidade tornou-se um problema de saúde pública emergente e complexo, cujo mecanismo é etiopatogênico e multifatorial. Tem sido estudado a partir da abordagem biomolecular e genética e através de intervenções para melhorar os estilos de vida, no entanto, não foram incluídos estudos que relacionem autoeficácia e resiliência neste problema.
Objetivo:
Avaliar a relação entre autoeficácia para controle de peso e resiliência em mulheres mexicanas.
Método:
Estudo correlacional e transversal, em 174 mulheres, com ou sem obesidade, matriculadas em um centro de treinamento para o trabalho em Puebla e San Luis Potosí, México, amostra de conveniência. Foram aplicados os instrumentos validados na população mexicana: Inventário de Autoeficácia para o controle de peso e Escala de Resiliência Mexicana, com alfa de Cronbach 0,945 e 9,50 respectivamente, o estudo foi realizado de acordo com a lei geral de saúde sobre pesquisa. A análise dos resultados foi realizada com estatística descritiva, testes de normalidade e correlação r de Spearman.
Resultados:
A média de idade foi de 34,6±14,7, a média de IMC 26,4±4,5, 49.7% e 81.7% obtiveram níveis altos de autoeficácia e resiliência respectivamente. A relação foi positiva, de tamanho médio do efeito e estatisticamente significativo (p=.001), com uma variância explicada de 22,6%.
Conclusão:
Mulheres mexicanas mostraram que, quanto maior a resiliência, maior a autoeficácia para o controle do peso. Sugere-se integrar a resiliência na gestão da obesidade, o que permite o desenvolvimento de mecanismos para a aquisição de estilos de vida saudáveis mais sustentáveis.
Palavras-chave: Autoeficácia; resiliência; controle de peso; mulheres; enfermagem (DeCS)
Introduction
Obesity is considered a public health problem, which is related to some of the main causes of death such as cardiovascular disease, diabetes, and certain types of cancer standing out (1, 2). Worldwide, 39% of the adult population is overweight and 13% obese 2; it is estimated that by year 2025, global prevalence of obesity in women will exceed 21% 3. In Latin America, the situation is similar, for example, in Mexico, 51.2% of population are women 4, of which 76.8% is overweight and obese (5), which leads to identifying the problem as an epidemic due their prevalence rates.
In Mexico, these are strategies to address the problem of obesity, including prevention, control, and treatment 6,7,8, and even new policies for the creation of a front labeling system for food and drinks, which provides information for healthy food choices 9,10. Obesity has been analyzed with regulatory measures aimed at improving social, cultural, economic, and environmental determinants that favor physical activity 11, with exercise and dietary changes 12 and with surgical treatment 13. However, despite all these strategies, attention to the psychological factor continues to be undervalued to strengthen the programs, which can even be treated as protection mechanisms such as self-efficacy (SE) and resilience (RE).
Regarding SE, Bandura and other authors 14-16 mention it as the confidence that the individual has to carry out the necessary actions that allow him to achieve the desired results in a certain behavior. The author explains that SE is an important factor in health behaviors, because it allows recognizing the difficulty of motivating the adoption of behaviors that promote health and consists of a series of interactions of personal factors, behaviors, and events in the environment 17,18. Some concepts may be related to SE, for example, with RE, which is determined as a set of attributes of the subject, in interaction with family, social and cultural environments, which, under difficult conditions, will indicate a normal development 19-22. In other words, RE is a psychic process that presents itself as a mixture of strength and fragility, which allows one to navigate the torrents of extreme difficulties and come out stronger in the end to continue with life 23,25-28.
The relationship between these two concepts of interest is that SE is one of the factors that promote RE 24. However, despite the fact that SE has been shown to be a protective element that promotes motivation, persistence, and effort to promote beneficial behavior, its relationship with RE is not clear. Nevertheless, the theoretical reasoning is as follows: if there is no motivation in woman by the family and society, it will be difficult for her to have confidence in order to generate healthy behaviors to control her weight 20-23, then, the achievement of goals, perseverance in the face of difficulties and its resistance to failures is determined by the relationship between SE and RE.
Theoretically, SE and RE could be complementary elements. It would be interesting to identify the relationship between these concepts in overweight and obese women, given that it is important to encourage the promotion of RE skills to prevent damage to health, especially on issues related to healthy habits that imply in this case a benefit to weight control. The construct associated with RE is SE, since overcoming adversities means an experience that modifies SE's beliefs to exercise self-control in life. Nurses should consider integrating both concepts in nutritional treatment and the prescription of a dose of exercise, aimed at weight control, with a comprehensive vision in favor of the health of individuals.
The relationship between SE for weight control and RE has not been published. The studies carried out on these concepts in overweight and obese people have been done separately. Given the lack of evidence that relates the cognitive concepts of SE for weight control and RE, reason why the research question was enunciated as follows: What is the relationship of SE for weight control and RE in Mexican women? Thus, the objective of evaluating the relationship of SE for weight control with RE in Mexican women was raised.
Methodology
In this correlational and cross-sectional study of SE for weight control and RE, the variables were defined based on their theoretical and psychometric principles 28-30. The participants were women enrolled in federal training centers for adult education in the states of Puebla and San Luis Potosi, Mexico. In Puebla, 90 women participated and in San Luis Potosi there were 85 participants, with a total of 175 women.
Women of legal age were included, who were registered in the chosen educational institution and who agreed to participate. Those with nutrition treatment for weight control, but who reported suffering from chronic diseases and pregnancy were excluded.
To measure the level of SE, the Perceived SE Inventory for weight control, validated in the Mexican population, was applied 29. The instrument contains 37 items distributed in three domains: diet with 20 statements, exercise with 9, and physical activity with 8. The items are designed on a Likert-type scale, with response options ranging from 1= incapable of doing so, 2 = little capable of doing so, 3= quite capable of doing so, up to 4= quite sure to do so. The maximum score was 148 points and the minimum was 37 points, with Cronbach's α coefficient values for this study of 0.916, 0.904 and 0.830 respectively.
To measure RE, the Mexican Resilience Scale (RESI-M) 30 was used. It contains five dimensions, a) strength and self-confidence, which are the positive perceptions about oneself or the ability to accept or cope with stressful events, b) Social competence, or the subject's ability to interact successfully with her environment and achieve legitimate satisfaction of her needs, c) Family support, which is the time shared by family members, the existing loyalty and the strength of their ties, d) Social support, which are the links between the subject and a defined group of people, with whom there is communication, solidarity and trust, and e) Personal structure, or the activities that facilitate organization and order in life. The scale is made up of 43 items, on a Likert-type scale, with response options ranging from 1= totally agree, 2= agree, 3= disagree to 4= totally disagree. A score of 0 to 33 is categorized as a low level of RE, a medium level of 34 to 66, and a high level of 67 to 100. Studies in the Mexican population reported Cronbach's Alpha of 0.87. Sociodemographic variables such as age, education in years, marital status and occupation were evaluated, in addition the Body Mass Index (BMI) was measured.
To collect data, authorization was requested from each campus. Subsequently, a written informed consent was obtained from the participants. The procedures followed the regulations of the General Health Law on Health Research 31; additionally, the research was approved by the Ethics and Research Committee. The data were processed using the statistical program named Statistical Package for the Social Sciences (SPSS) version 18. Descriptive statistics were used through measures of central tendency, as well as inferential tatistics for non-parametric variables, Student's T test for SE for weight control and BMI and Mann-Whitney U for RE, Spearman correlation and linear regression (SE dependent variable and independent RE).
Results
The average age of the participants ranged from 34.6 ± 14.7 years, with years of schooling of 11.9 ± 3.10. Regarding the BMI, 26.4 ± 4.5 showed overweight, (Table 1).
Table 1 Sociodemographic and anthropometric variables of the participating women, 2016. (n=175).
| Variable | x± SD | Minimum | Maximum |
| Age | 34.6 ± 14.7 | 18 | 69 |
| Schooling in years | 11.92 ± 3.10 | 6 | 19 |
| Body mass index | 26.4 ± 4.5 | 16.6 | 44.7 |
Source: Own development
In SE for weight control, the highest percentage showed a high level with 49.7%, as well as in RE with 81.7% (Table 2). Regarding the reliability of the instruments, SE for weight control and RESI-M had a general Cronbach's alpha of 0.945 and 0.950 respectively.
Table 2 Level of self-efficacy and resilience of the participating women, 2016 (n=175).
| Cut-off points | Level | Self-efficacy | Resilience |
| f % | f % | ||
| 0-33 | Low | 7 4.0 | 0 0 |
| 34-66 | Medium | 81 46.3 | 32 18.3 |
| 67-100 | High | 87 49.7 | 143 81.7 |
Source: Own development
In the correlation of variables, a medium effect size is shown, a moderate magnitude and statistically significant (p=0.001). In the relationships of each of the domains and factors of the instrument used, statistical significance is shown in all relationships (p=0.001), except social support regarding diet (r=0.134, p=0.078). However, diet is the domain with the highest and most significant correlations with the other RE domains (Table 3).
Table 3 Relationship between Self-efficacy and Resilience, 2016.
| SE | D | Ex | PA | RE | S & C | SC | FS | SS | |
| Self-efficacy (SE) | 1 | ||||||||
| Diet (D) | 1 | ||||||||
| Exercise (Ex) | .618** | 1 | |||||||
| Physical Activity (PA) | .614** | .561** | 1 | ||||||
| Resilience (RE) | .454** | 1 | |||||||
| Strength and Confidence (S & C) | .464** | .361** | .375** | 1 | |||||
| Social Competence (SC) | .387** | .259** | .297** | .514** | 1 | ||||
| Family Support (FS) | .316** | .254** | .327** | .560** | .471** | 1 | |||
| Social Support (SS) | .134 | .182** | .249** | .464** | .422** | .607** | 1 | ||
| Structure (St) | .396** | .283** | .272** | .570** | .511** | .531** | .392** |
Source: Own development
Figure 1 shows a scatter graph with a positive direction, some of the subjects with SE and low RE are the most dispersed; however, the majority tend to form clusters, indicating a statistically significant correlation.
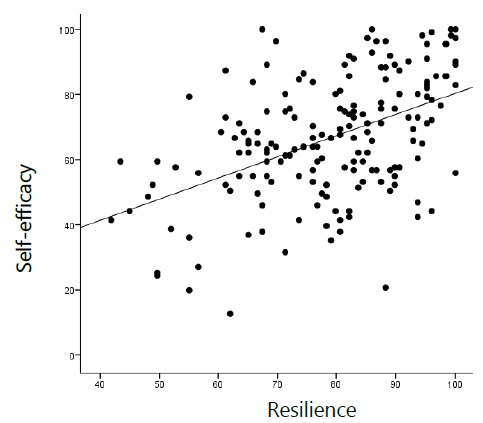
A simple linear regression model was adjusted, where RE was introduced as the independent variable and SE as the dependent variable, an adjusted R² of 0.226 was obtained; therefore, the percentage of the explained variation of SE over the variability of the RE is 22.6 %, (Table 4).
Table 4 Simple linear regression
| Model Summary | |||||||||
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate | Change Statistics | ||||
| R Square Change | F Change | df1 | df2 | Sig. F Change | |||||
| 1 | .475a | .226 | .222 | 16.454 | .226 | 50.533 | 1 | 173 | .000 |
a. Predictors: (Constant), Index
Given that the sample was drawn from two geographical areas (Puebla and San Luis Potosi), it was decided to carry out an additional analysis to make comparisons of the arithmetic means of the study variables of the States; with respect to the RE, a range difference of 4.26 points was seen, presenting the highest score for women from San Luis Potosi, compared to women from Puebla. When performing the comparison of ranges through the Mann-Whitney U, it was possible to see that there was no statistically significant difference with respect to the two study groups (p˃0.05). Therefore, the SE variable for weight control and RE are not different in women from the State of San Luis Potosi compared to women from the State of Puebla (Table 5).
Table 5 Contrast statistical tests.
| Variable | Levene's test of equality of variance | Student's t-test for unrelated samples | |||
| F | Sig. | 95% Confidence interval | t | p | |
| Self-efficacy | 0.293 | 0.589 | -3.997, 7.159 | 0.579 | .577 |
| Variable | State | Middle range | Sum of ranges | Mann–Whitney U | p |
| Resilience | SLP | 90.19 | 7666.00 | 3639.00 | .579 |
| Puebla | 85.93 | 7734.00 | |||
Source: Own development SLP: San Luis Potosi
Discussion
The objective was to evaluate the relationships of SE for weight control with RE, in Mexican women from Puebla and San Luis Potosi, Mexico, in addition to determining if there were differences between the study groups. The descriptive data showed an arithmetic mean of age that tends to represent young adults, although the standard deviation is wide and covers other age groups (adolescence and adulthood), matching the studies from Brazil 13 and Mexico 27. The average age presented is an economically productive stage. This was expected because the school where the study was carried out offers training courses for industrial work and courses with a certain occupation identified in the labor market. The results presented represent the demographic transition process in Mexico, one of its consequences is that the current population structure presents a higher proportion of people in productive ages 6. Regarding schooling, the majority had completed secondary and upper middle education, similar to the study in Brazil 13; in contrast to a research carried out in Baja California, Mexico 27, such coincidences are due to the fact that this study was carried out in a job-training center where one of the entry requirements is to have high school degree. Regarding marital status, in general the majority was single, a fact that contrasts with the study in Brazil 13; the results reflect the national Mexican situation, since 31.5% of women are single and 15% of women are without a partner once they left a marital union 4. Regarding BMI, the arithmetic mean showed overweight according to the WHO classification 2, which corresponds to overweight and obesity that are present in more than 70% of the Mexican population 5.
In SE for weight control, the highest percentage was at the high level, results that theoretically present possibilities to control their weight 27. However, the results must be considered with reservation, since the SE only represents the confidence or the intention and is not the action itself. However, literature mentions the relationship between appropriate behaviors and high RE, which suggested the impact of RE on the ability to manage treatment and healthy lifestyle habits 20,24,25.
The RE scores showed a high level for the most part, women are more resilient 30, even in adverse conditions, because the RE is the result not only of protective and risk factors, but also of protective mechanisms that are triggered 26. The RE is then the manifested result in the development of the well-being and health of people, since it allows them to face adversity in a better way 25.
This work showed that, if RE is high, SE for weight control will also be high, since as a protective factor it promotes it, creating strength and confidence to generate healthy behaviors, as mentioned by various authors 24 such as a positive impact on physical and mental health. As long as the woman is accepted by significant others and has informal support networks in the community, there are positive family and social conditions to favor RE, a situation that was clarified given the results of the correlation 25,26.
The SE correlations for weight control with diet, exercise, and physical activity, RE factors with strength and self-confidence, social competence, family support, social support, and personal structure, from the theoretical point of view the relationships were found with a medium effect size, statistically significant and more indicators are those carried out with each one of the domains of SE, with the strength and self-confidence factor of RE. These relationships may be due to the fact that women produce their efficacy beliefs through the processes: cognitive, motivational, affective and selective, they are self-regulatory of their own behavior that mediate between intentions and actions, even with the presence of environmental factors or biological, the volitional process contains plans and action control and is strongly influenced by the expectations of SE, so that it can carry out actions in favor of her health such as dieting, exercising or physical activity 24.
The relationship between the RE dimensions and the SE domains refers to a set of positive expectations, participating cognitive and affective protective factors such as self-esteem, motivation to achievement, the feeling of self-sufficiency and confidence that makes them think that problems will be solved; so, these results agree with a study 30 being the most important factor to measure the RE since it explained a greater percentage of the variance of the concept in relation to the SE.
In this context, if the SE principles are activated in women, acting as a protective factor to promote RE, motivation, persistence, effort, goal achievement, the time they persevere in the face of difficulties, and their resistance to failures increase 24, theoretically the subject overcomes adversities to build strength and self-confidence, generating healthy behaviors to control her weight. This work confirms that SE may be a variable that favors adherence to changes in food intake and consequently weight loss.
Diet relationships with social competence, family support and structure have a medium and statistically significant effect size. It is possible that this positive relationship is due to the woman's ability to interact with her environment and achieve the legitimate satisfaction of her priorities by influencing her peers. This is related to emotional adjustment (social competence), loyalty and strength among the members of her family who provide her with the support to carry out a healthy diet (family support), the rules and organization carried out by women, makes it easier for them to carry out a personal structure represented by carrying out a diet 30. This has a positive impact when having emotional activation and verbal persuasion by the family, principles to achieve the SE beliefs that regulate significant goals 24.
Within the correlation model, only one interaction was not significant, social support with diet, if there is no interaction with these personal and behavioral factors, the thoughts that a person has about her ability and self-regulation to implement healthy behaviors will not be favorable, since the perceived SE is related to positive thoughts and aspirations about performing the behavior successfully 24,27. If a woman is not motivated, the perception of her actions will not be effective, if she does not have the conviction of having skills to regulate actions that allow her to carry out a healthy diet, she will not be able to control her weight. This may be due to the stigma society places on people who are overweight and obese, indicating that they are not capable of healthy diet and exercise behaviors. Regarding social support, it is likely that the existing links between a woman and the people she lives with do not provide her with that solidarity to carry out actions in favor of her health, such as weight control.
The relationships of exercise with social competence, family support, social support and structure are positive with a medium and statistically significant effect size, given that they receive family and social support to carry out the exercise, coinciding with studies that report the influence of the sociocultural environment that overweight and obese people have to exercise 12. If women are influenced by other people's behaviors or achievements (vicarious experience) along with verbal persuasion and emotional activation, SE expectations are stronger, believing they have capabilities to perform exercise and diet successfully 24, a situation that can explain resilient behaviors, emotional motivation, beliefs about the ability (performance achievements) thus achieving actions in favor of their health.
The limitations of this research were the cross-sectional design, the sample size and that it was only carried out on women. It would be interesting to make correlations between these two cognitive variables in men and in school-age children. It should be noted that correlation of variables has been little explored by researchers. For this reason, the study provides preliminary data to carry out intervention work.
Conclusions
The findings show that the higher the RE, the higher the SE for weight control. The effect size of the correlation was average; the percentage of variance explained was high. These results suggested the importance of integrating the promotion of RE pillars in the care and weight control of the client or user, in such a way that it allows her to obtain coping tools for a more efficient weight control and therefore improve her health through the inclusion of healthier lifestyles. RE is a process that can be learned and developed allowing the individual to face adversity and come out stronger, as a result of a combination of individual characteristics and the environment. That is why its inclusion in nursing care plans is highly relevant, since it promotes other protective mechanisms, such as SE in this case.
Referencias bibliográficas
1. Organización Mundial de la Salud (OMS). Marco global de vigilancia en nutrición: directrices operacionales para el seguimiento de los progresos hacia el logro de las metas para 2025. [Internet]. Ginebra; 2018 [citado 09 jun 2021]. Disponible en: Disponible en: https://apps.who.int/iris/bitstream/handle/10665/272262/9789243513607-spa.pdf [ Links ]
2. Organización Mundial de la Salud (OMS). Obesidad y sobrepeso. Noticias [Internet]. 2018 [citado 09 jun 2021]. Disponible en: Disponible en: http://www.who.int/es/news-room/fact-sheets/detail/obesity-and-overweight [ Links ]
3. NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from1975 to 2014: a pooled analysis of 1698 population-based measurements studies with 19.2 million participants. Lancet [Internet]. 2016 [citado 04 jul 2021]; 387:1377-96. Disponible en: Disponible en: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(16)30054-X/fulltext [ Links ]
4. Instituto Nacional de Estadística y Geografía. Población. Temas [Internet]. 2020 [citado 20 sep 2021]. Disponible en: Disponible en: https://www.inegi.org.mx/temas/estructura/ [ Links ]
5. Instituto Nacional de Geografía e Informática. Encuesta Nacional de Salud y Nutrición. [Internet]. 2018 [citado 17 agosto 2021]. Disponible en: Disponible en: https://ensanut.insp.mx/encuestas/ensanut2018/doctos/informes/ensanut_2018_presentacion_resultados.pdf [ Links ]
6. Comisión Nacional de Derechos Humanos. Norma Oficial Mexicana NOM-043-SSA2-2012 Servicios básicos de salud. Promoción y educación para la salud en materia alimentaria. Diario Oficial de la Federación [Internet]. 2012 [citado 15 ago 2021]. Disponible en:Disponible en: https://www.cndh.org.mx/DocTR/2016/JUR/A70/01/JUR-20170331-NOR37.pdf [ Links ]
7. Diario Oficial de la Federación. Norma Oficial Mexicana NOM-008-SSA3-2017 Para el tratamiento integral del sobrepeso y la obesidad. Diario Oficial de la Federación. [Internet]. 2012 [citado 16 ago 2021]. Disponible en: Disponible en: https://dof.gob.mx/nota_detalle.php?codigo=5523105&fecha=18/05/2018 [ Links ]
8. Secretaria de Salud. Estrategia nacional para la prevención y el control del sobrepeso, la obesidad y la diabetes. [Internet]. 2013 [citado 15 ago 2021]. Disponible en Disponible en https://www.gob.mx/cms/uploads/attachment/file/276108/estrategia_sobrepeso_diabetes_obesidad.pdf [ Links ]
9. Hernández-Nava LG, Egnell M, Aguilar-Salinas CA, Córdova-Villalobos JÁl, Barriguete-Meléndez JA, Pettigrew S, et al. Impacto de diferentes etiquetados frontales de alimentos según su calidad nutricional: estudio comparativo en México. Salud Pública Méx [Internet]. 2019 [citado 18 ago de 2021];61(5):609-18. Disponible en: Disponible en: https://www.saludpublica.mx/index.php/spm/article/view/10318 [ Links ]
10. Kaufer H, Tolentino M, Jáuregui A, Sánchez B, Bourges H, Martínez S, et al. Sistema de etiquetado frontal de alimentos y bebidas para México: una estrategia para la toma de decisiones saludables. Salud pública Méx [Internet]. 2018 [citado 21 sep 2021];60(4):479-486. Disponible en: https://doi.org/10.21149/9615. [ Links ]
11. Organización Panamericana de la Salud. Plan de acción mundial sobre actividad física 2018-2030. Más personas activas para un mundo sano. Iris.paho.org [Internet]. 2019 [citado 15 ago 2021]. Disponible en: Disponible en: https://iris.paho.org/bitstream/handle/10665.2/50904/9789275320600_spa.pdf [ Links ]
12. Cuadri-Fernández J, Tornero-Quiñones I, Sierra-Robles A, Sáez-Padilla JM. Revisión sistemática sobre los estudios de intervención de actividad física para el tratamiento de la obesidad. Retos [Internet]. 2018 [citado 21 sep 2021];33:261-266. Disponible en: Disponible en: http://hdl.handle.net/10272/16258 [ Links ]
13. Silva TP, Porto AC, Mendes LL, Gomes FS, Araujo LP, Matozinhos FP. Calidad de vida de los pacientes sometidos a cirugía bariátrica: estudio transversal. Enf Global [Internet]. 2020 [citado 22 sep 2021];19(2):305-50. Disponible en: Disponible en: https://revistas.um.es/eglobal/article/view/362191 [ Links ]
14. Bandura A. Social foundations of thought and action. A Social Cognitive Theory. New Jersey, EE. UU: Prentice Hall; 1986. [ Links ]
15. León HR, Gómez PM, Méndez SG, Torres CY. Predictores de autoeficacia para el control de peso en estudiantes adolescentes. Revista de Psicología de la Universidad Autónoma del Estado de México [Internet]. 2022 [citado 15 feb 2022];11(22):188-207. Disponible en: https://doi.org/10.36677/rpsicologia.v11i22.17733 [ Links ]
16. Matar KS, Ortiz MJ. La autoeficacia en la salud y en el control del peso. Desbordes [Internet]. 2020 [citado 15 feb 2022];11(1):114-137. Disponible en: Disponible en: https://hemeroteca.unad.edu.co/index.php/desbordes/article/view/4080/5231 [ Links ]
17. De la Cruz M, Guzmán S, Gómez P, Platas A. Diferencias por sexo en la autoeficacia para el control de peso en preadolescentes de la ciudad de Pachuca, Hidalgo. Gaceta Hidalguense de Investigación en Salud [Internet]. 2018 [citado 15 feb 2022];6(3):6-11 Disponible en: Disponible en: https://s-salud.hidalgo.gob.mx/contenido/informacion/gaceta/Gaceta18_3_Autoeficacia.pdf [ Links ]
18. Trujillo HP, Flores PY, Gómez MD, Lara RB, García JA, Gutiérrez VJ. Análisis de las propiedades psicométricas de la escala de autoeficacia de la conducta alimentaria en adolescentes mexicanos. Nutr. Hosp., Supl [Internet]. 2021 [citado 15 feb 2022];38(4):821-826 Disponible en: Disponible en: https://www.nutricionhospitalaria.org/articles/03501/show [ Links ]
19. Vergel OM, Gómez VC, Gallardo PH. Resiliencia en mujeres universitarias en norte de Santander, Colombia. Rev. latinoam. cienc. soc. niñez juv [Internet.] 2021 [citado 21 sep 2021];19(3):1-19. Disponible en: https://doi.org/10.11600/rlcsnj.19.3.4590 [ Links ]
20. Sanjuan-Meza X, Landeros-Olvera E, Cossío-Torres P. Validade de uma escala de resiliencia (RESI-M) em mulheres indígenas do México: Cadernos de Saúde Pública [Internet]. 2018 [citado 21 sep 2021];34(10)11. Disponible en: https://doi.org/10.1590/0102-311X00179717 [ Links ]
21. Benavente-Cuesta H, Quevedo-Aguado P. Resiliencia, bienestar psicológico y afrontamiento en universitarios atendiendo a variables de personalidad y enfermedad. Journal of Psychology and Education [Internet]. 2018 [citado 23 sep 2021];13(2):99-112. Disponible en: https://doi.org/10.23923/rpye2018.01.161 [ Links ]
22. Gómez ED, Delgado SU, Martínez FF, Ortiz RM, Avilés RR. Resiliencia, género y rendimiento académico en jóvenes universitarios del estado de Morelos. RCCEPG [Internet]. 2021 [citado 01 oct de 2021];6(1):36-51. Disponible en: Disponible en: https://revistaconcienciaepg.edu.pe/ojs/index.php/55551/article/view/108 [ Links ]
23. Ruiz-Román C, Juárez PJ, Molina CL. Evolución y nuevas perspectivas del concepto de resiliencia: de lo individual a los contextos y relaciones socioeducativas. ESXXI [Internet]. 2020 [citado 22 sep 2021 ];38(2):213-232. Disponible en: Disponible en: https://revistas.um.es/educatio/article/view/432981 [ Links ]
24. Bandura A. Self-Efficacy in Changing Societies. Edinburgh, United Kingdom: Cambridge University Press; 1999. [ Links ]
25. Asensio-Martínez A, Magallón-Botalla R, García-Campayo J. Resiliencia: impacto positivo en la salud física y mental. Revista INFAD de Psicología [Internet]. 2018 [citado 21 sep 2021];2(1):231-242. Disponible en: Disponible en: https://revista.infad.eu/index.php/IJODAEP/article/view/1096/965 [ Links ]
26. García del Castillo JA, García del Castillo-López A, López-Sánchez C, Dias PC. Conceptualización teórica de la resiliencia psicosocial y su relación con la salud. Salud y drogas [Internet]. 2016 [citado 21 sep 2021];16(1):59-68 Disponible en: Disponible en: https://www.redalyc.org/articulo.oa?id=83943611006 [ Links ]
27. Aguiar-Palacios L, Magallanes-Rodríguez A, Martínez-Alvarado J, Negrete-Cortes A, García-Gomar M. Autoeficacia para control de peso en estudiantes universitarios del área de la salud. PSIENCIA Revista Latinoamericana de Ciencia Psicológica [Internet]. 2017 [citado 21 sep 2021];9(1):1-14. Disponible en: Disponible en: https://www.redalyc.org/pdf/3331/333152921001.pdf [ Links ]
28. Aguiar-Palacios L, Negrete-Cortés A, Martínez-Alvarado J, Magallanes R A, García-Gomar M. Propiedades psicométricas del inventario autoeficacia percibida para el control de peso en estudiantes universitarios del área de la salud. Nutrición Hospitalaria [Internet]. 2018 [citado 21 sep 2021];35(4):888-893. Disponible en: http://dx.doi.org/10.20960/nh.1557 [ Links ]
29. Landeros-Olvera E, Salazar-González B, López-Alvarenga J. Validation and standardisation of the weight control perceived self-efficacy inventory in a Mexican college population. Aquichan [Internet]. 2015 [citado 21 sep 2021];15(1):44-51. Disponible en: Disponible en: https://www.redalyc.org/pdf/741/74137151005.pdf [ Links ]
30. Palomar-Lever J, Gómez-Valdez N. Desarrollo de una escala de medición de la resiliencia con mexicanos (Resi-M). Interdisciplinaria [Internet]. 2010 [citado 21 sep 2021];27(1):7-22. Disponible en: Disponible en: https://www.redalyc.org/articulo.oa?id=18014748002 [ Links ]
31. Diario Oficial de la Federación. Reglamento de la Ley General de Salud en Materia de Investigación para la Salud. Cámara de Diputados del H. Congreso de la Unión, Secretaría General, Secretaría de Servicios Parlamentarios [Internet]. 2014 [citado 15 ago 2021]. Disponible en: Disponible en: http://www.liconsa.gob.mx/wp-content/uploads/2015/11/Reglamento-de-la-Ley-General-de-Salud-en-Materia-de-Investigación-para-la-Salud.pdf [ Links ]
Received: October 13, 2022; Accepted: January 26, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
