











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
The rapid spread of coronavirus disease-2019 (COVID-19), caused by a novel beta-coronavirus known as severe acute respiratory syndrome 2 (SARS-CoV-2), has had a dramatic impact on both people and health system worldwide1. The number of people infected with SARS-CoV-2 created intensive demand for health-care systems with limited resources resulting in decreased capacity, a rapid depletion of health-care service systems, and made the hospitals a source of viral transmission.
Risks of delayed diagnosis and treatment differ between different genitourinary tumors; some require more rapid intervention than others, including high-grade bladder cancer (BC), advanced renal cell carcinoma, testicular cancer, and penile carcinoma2. As urothelial cancer progresses rapidly, it is important to prioritize the timely care of these cancers. Urology associations and reference centers have released recommendations to give information about urological care during the COVID-19 pandemic. It is essential that urologists prioritize patient safety with a balance between potential delays in the diagnosis and treatment of urological conditions and the related additional burden on health-care resources and the risk of exposure to COVID-193. While it has been targeted to preserve health-care resources due to the burden created by the pandemic, the risk of delayed treatment of cancer has emerged. Consequently, the transformation of health-care services and increased interest of the population in avoiding disease exposure have resulted in reduced numbers of hospital presentations.
The effect of the outbreak on BC patients due to decreased presentation at emergency rooms and urology clinics is unclear. The European Association of Urology (EAU) Guidelines Office Rapid Reaction Group published a guideline to adapt the EAU recommendations for the COVID-19 period4. According to this guideline, four priority groups were established, and a certain time of delay to treatment was specified for each patient group based on their priority.
The aim of this study was to identify how the COVID-19 pandemic influenced the oncological outcomes of primary BC, tumor stage and grade, symptom duration, time to surgery from diagnosis, pre-operative clinical characteristics, and post-operative follow-up.
Material and methods
Approval for this single-center and retrospective study was granted by the Local Ethics Committee and all procedures were in accordance with the Declaration of Helsinki. It was planned to enroll all patients who underwent a transurethral resection of bladder tumor (TURBT) procedure for the primary BC between November 2018 and July 2021. Our center is a reference hub for COVID-19 patients and has been providing healthcare to a large patient population since the beginning of the pandemic. Bladder tumors were defined as urothelial carcinoma detected in post-operative pathology specimens. The study exclusion criteria were defined as a history of urinary system tumor, chronic kidney disease, or anemia.
The patients were allocated to one of the groups: Pre-COVIDBC or COVIDBC. The COVIDBC group consisted of patients diagnosed between March 2020 and July 2021 (during the COVID-19 pandemic), and the Pre-COVIDBC group consisted of patients diagnosed between November 2018 and March 2020 (before the COVID-19 pandemic).
After the pre-operative diagnosis of BC, all patients were prepared for surgery regardless of risk. No patient was referred to another center as our hospital was able to manage all BC cases during the pandemic. The surgery was performed under spinal anesthesia and by the same anesthesia team. All TURBT procedures were performed by an experienced surgeon (more than 100 cases).
A record was made of demographic baseline data and tumor characteristics, including gender, age, the American Society of Anesthesiologists score, body mass index, hydronephrosis grade, hemoglobin, serum creatinine, tumor side, tumor count, tumor size, and tumor localization. It was planned to repeat the initial cystoscopy at the end of the 3rd month in all patients. Patients without follow-up were defined as those who were not admitted for cystoscopy control within the first 6 months. Early cystectomy was recommended for suitable very high risk patients, and 3rd month cystoscopy follow-up was recommended for patients not suitable for surgery or those who declined surgical treatment. Incomplete resection was defined as visible tumor tissue left after the TURBT procedure.
In the patients who presented with primary bladder tumor, T-stage, tumor grade, and the presence of carcinoma in situ (CIS) were evaluated. The EAU non-muscle invasive bladder cancer (NMIBC) risk stratification was applied to NMIBC patients using these data and the two groups were compared. The 2006 European Organization for Research and Treatment of Cancer (EORTC) scoring model (tumor count, tumor size, number of recurrences in the last year, T-stage, presence of CIS, and tumor grade) was used for EORTC recurrence and progression scores. Comparisons were made between the groups in respect of time to TURBT operation from diagnosis, rate of follow-up, symptom duration, microscopic and macroscopic hematuria, incomplete resection, duration of surgery, duration of post-operative hospital stay, and complications.
The data were analyzed using IBM SPSS Statistics v.26®. Conformity of the continuous variables to normal distribution was assessed using the Kolmogorov-Smirnov tests and P-P plot tests. The variables showing normal distribution were presented as mean ± standard deviation values, and those not showing normal distribution as median (minimum-maximum) values. Categorical variables were presented as number (n) and percentage (%). Comparisons of categorical variables between the groups were made using Pearson's Chi-square and Fischer's Exact Test. The tests were specified according to the smallest theoretical frequency with Fisher's Exact Test used in case of < 5 and Pearson's Chi-square Test > 5. Continuous variables were compared using the Independent Samples t-test for normally distributed data, and the Mann-Whitney U-test was applied to non-normally distributed data. p < 0.05 was considered statistically significant.
Results
Evaluations were made of a total of 275 patients diagnosed with bladder tumor between November 2018 and July 2021 (147 before the COVID-19 pandemic and 128 during the COVID-19 pandemic). The demographic characteristics and pre-operative clinical data are listed in Table 1. Newly diagnosed BC cases showed a 13% decrease during the COVID-19 pandemic compared to before COVID-19.
Table 1 Demographic characteristics and pre-operative data
| Pre-COVIDBC (n = 147) | COVIDBC (n = 128) | p - value | |
|---|---|---|---|
| Age (years) | 64.7 ± 13.4-66 (31-87) | 63.5 ± 12.5-65 (22-92) | 0.4 |
| BMI (kg/m2) | 27.3 ± 2.6-27.6 (20.2-34.3) | 27.0 ± 2.3-27.5 (22.0-32.7) | 0.5 |
| Gender | 0.3 | ||
| Male | 123 (83.7) | 112 (87.5) | |
| Female | 24 (16.3) | 16 (12.5) | |
| ASA score | 0.1 | ||
| 1 | 11 (7.5) | 16 (12.5) | |
| 2 | 70 (47.6) | 67 (52.3) | |
| 3 | 66 (44.9) | 45 (35.2) | |
| Hematuria | 0.04* | ||
| Gross hematuria | 103 (70.1) | 106 (82.8) | |
| Mic. hematuria | 22 (15.0) | 12 (9.4) | |
| No hematuria | 22 (15.0) | 10 (7.8) | |
| Hydronephrosis | 0.05* | ||
| Grade 0 | 128 (87.1) | 100 (78.1) | |
| Grade 1 | 6 (4.1) | 12 (9.4) | |
| Grade 2 | 9 (6.1) | 14 (10.9) | |
| Grade 3 | 4 (2.7) | 2 (1.6) | |
| Hemoglobin (gr/dL) | 14.0 ± 2.3-14.5 (8.4-18.6) | 14.1 ± 2.0-14.4 (7.6-17.8) | 0.7 |
| Serum creatinine (mg/dL) | 1.26 ± 1.20-1.0 (0.6-9.1) | 1.20 ± 1.16-0.9 (0.5-8.8) | 0.7 |
| Time from diagnosis to treatment (day) | 12 ± 6-12 (3-34) | 30 ± 21-27 (3-96) | 0.001* |
| Symptom duration (weeks) | 7.3 ± 6.9-1 (0.5-12) | 9.1 ± 7.5-1 (0.5-18) | 0.04* |
(*) Statistically significant difference.
Data are shown as mean ± SD, median (minimum-maximum) values and number (n) and percentage (%).
BMI: body mass index; ASA: the American Society of Anesthesiologist.
Regarding the oncological outcomes of all the BC patients, the study results confirmed an overall significant increase in higher tumor stages (T2) during the pandemic compared to before the pandemic, with significantly fewer Ta tumors (p = 0.04). The incidence of higher stage tumors (T2) was 18.4% pre-pandemic compared to 31.3% during the pandemic, and the rate of Ta tumors decreased during the pandemic compared to the pre-pandemic period (36.7% vs. 42.9%) (Fig. 1). A significant difference was determined in tumor count between the pre-pandemic and pandemic periods (1.4±0.6 vs. 1.6 ± 1.0; p = 0.02). In patients with BC, no adverse oncological outcomes concerning tumor grading could be detected in the comparisons of the pre-pandemic and pandemic periods. The surgical findings, intraoperative data, and tumor characteristics are shown in Table 2.
Table 2 Surgical and tumor characteristics
| Pre-COVIDBC (n = 147) | COVIDBC (n = 128) | p - value | |
|---|---|---|---|
| Tumor size (cm) | 2.1 ± 1.4-2 (0.3-10) | 2.4 ± 1.8-2 (0.5-14) | 0.1 |
| Tumor count | 1.4 ± 0.6-1 (1-6) | 1.6 ± 1.0-1 (1-8) | 0.02* |
| Tumor site | 0.6 | ||
| Right | 58 (39.5) | 51 (39.8) | |
| Left | 51 (34.7) | 39 (30.5) | |
| Bilateral | 38 (25.9) | 38 (29.7) | |
| Tumor number | 0.5 | ||
| Solitary | 25 (49.0) | 30 (56.6) | |
| Multiple | 26 (51.0) | 23 (43.4) | |
| Tumor localization | 0.5 | ||
| Lateral | 106 (72.1) | 90 (70.3) | |
| Posterior | 11 (7.5) | 16 (12.5) | |
| Anterior | 10 (6.8) | 6 (4.7) | |
| Neck-Trigone | 13 (8.8) | 8 (6.3) | |
| Dome | 7 (4.8) | 8 (6.3) | |
| Tumor stage | 0.04* | ||
| Ta | 63 (42.9) | 47 (36.7) | |
| T1 | 57 (38.8) | 41 (32.0) | |
| T2 | 27 (18.4) | 40 (31.3) | |
| Tumor grade | 0.2 | ||
| PUNLMP | 62 (42.2) | 41 (32.0) | |
| Low | 30 (20.4) | 28 (21.9) | |
| High | 55 (37.4) | 59 (46.1) | |
| CIS (concomitant) | 0.3 | ||
| Present | 18 (12.2) | 21 (16.4) | |
| Not present | 129 (87.8) | 107 (83.6) | |
| Complete resection | 0.8 | ||
| Present | 132 (89.8) | 116 (90.6) | |
| Not present | 15 (10.2) | 12 (9.4) | |
| Complication | 0.9 | ||
| Hematuria | 8 (5.5) | 7 (5.5) | |
| Post-operative fever | 6 (4.0) | 6 (4.7) | |
| Not present | 133 (90.5) | 115 (89.8) | |
| Operation time (min) | 27.8 ± 14.0−25 (10-120) | 29.4 ± 15.3-25 (15-115) | 0.3 |
| Hospitalization time (days) | 1.3 ± 0.6-1 (1-6) | 1.2 ± 0.4-1 (1-4) | 0.001* |
(*) Statistically significant difference.
Data are shown as mean ± SD, median (minimum-maximum) values and number (n) and percentage (%).
PUNLMP: Papillary urothelial neoplasm of malignant potential; CIS: Carcinoma in situ.
Of the 208 NMIBC patients, the COVIDBC group included 88 and the Pre-COVIDBC group included 120. The clinical findings and follow-up results of both groups are listed in Table 3. Based on the EAU NMIBC risk stratification, these results demonstrate a significant increase in very high-risk patients during the pandemic compared to pre-pandemic, with a significant decrease in low-risk patients (p = 0.02). When NMIBC was evaluated, the incidence of very high-risk patients increased by 11.5% (18.2% vs. 6.7%) during the pandemic compared to pre-pandemic, and low-risk patients decreased by 14.2% (25.0% vs. 39.2%). In respect of the recurrence and progression scores of NMIBC patients, the study results showed a significantly higher EORTC recurrence (median [min-max], 9 [0-14] vs. 6 [0-13]) and progression score (median [min-max], 9 [0-19] vs. 5 [0-15]) during the pandemic than before the pandemic (p = 0.001) (Fig. 2). A significant difference was determined between the groups in respect of the follow-up rates (pre-pandemic: 80.8% vs. pandemic: 68.2%; p = 0.03) (Fig. 3).
Table 3 NMIBC clinical and follow-up data results
| Pre-COVIDBC (n = 120) | COVIDBC (n = 88) | p - value | |
|---|---|---|---|
| EAU NMIBC risk group | 0.02* | ||
| Low | 47 (39.2) | 22 (25.0) | |
| Intermediate | 19 (15.8) | 16 (18.2) | |
| High | 46 (38.3) | 34 (38.6) | |
| Very high | 8 (6.7) | 16 (18.2) | |
| EORTC recurrence score | 6.3 ± 3.9-6 (0-13) | 7.8 ± 3.0-9 (0-14) | 0.001* |
| EORTC progression score | 5.4 ± 4.1-5 (0-15) | 8.6 ± 3.4-9 (0-19) | 0.001* |
| Follow-up | 0.03* | ||
| Present | 97 (80.8) | 60 (68.2) | |
| Not present | 23 (19.2) | 28 (31.8) |
(*) Statistically significant difference.
Data are shown as mean ± SD, median (minimum-maximum) values and number (n) and percentage (%).
EAU: European Association of Urology; NMIBC: Non-muscle invasive bladder cancer; EORTC: European Organization for Research and Treatment of Cancer.

Figure 1 Tumor stage was Ta in 63 (42.9%), T1 in 57 (38.8%) and T2 in 27 (18.4%) of the 147 patents in the Pre-COVIDBC group, and Ta in 47 (36.7%), T1 in 41 (32.0%), and T2 in 40 (31.3%) of the 128 patients in the COVIDBC group (Chi-square test, p = 0.04). Each error bar is constructed using a 95% confidence interval of the count.
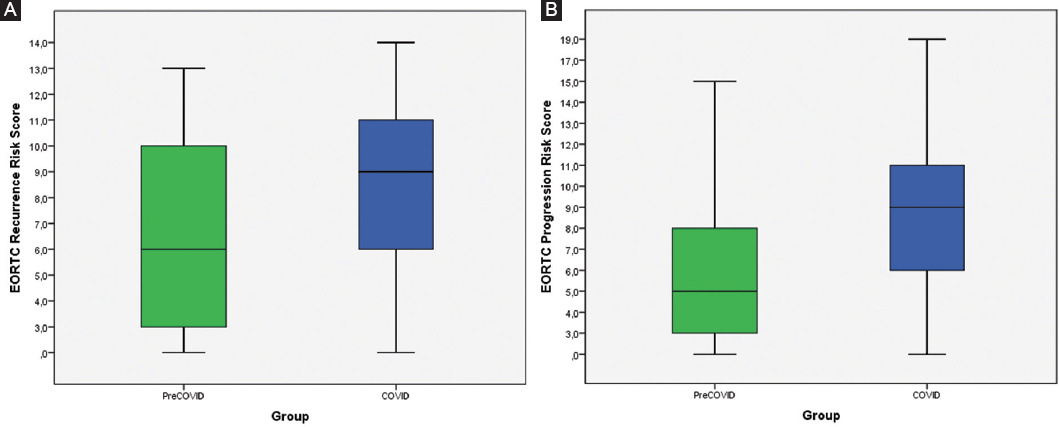
Figure 2 Scores of recurrence and progression of bladder cancer were assessed according to the EORTC scoring system. A: EORTC recurrence score was median (min-max, lower-upper quartile), 6 (0-13, 3-10) for the Pre-COVIDBC group, and 9 (0-14, 6-11) for the COVIDBC group (Mann-Whitney U-test, p = 0.001), B: EORTC progression score was median (min-max, lower-upper quartile), 5 (0-15, 3-8) for the Pre-COVIDBC group, and 9 (0-19, 6-11) for the COVIDBC group (Mann-Whitney U-test, p = 0.001).

Discussion
In this study, comparisons were made of patients with the primary bladder tumor who presented at hospital either during or before the COVID-19 pandemic. In the group that presented during the COVID-19 pandemic, T stage showed a significant increase in favor of T2 (MIBC) compared to the group that presented before the pandemic and there was a significant increase in the ratio of NMIBC high-risk patients according to the EAU risk stratification. The duration of symptoms and time to surgery from diagnosis at presentation were significantly prolonged. In contrast, the rate of follow-up showed a significant decrease during the COVID-19 pandemic.
The COVID-19 pandemic increased the burdens on health-care systems, primarily in the emergency rooms and intensive care units, leading to delays in many diagnoses and treatment procedures. Diagnostic pathways have been interrupted in cancers, especially in those that have screening programs such as prostate, colorectal, or cervical cancers. A decrease of 77%, 62%, and 26% has been reported in newly diagnosed prostate, colorectal, and breast cancers, respectively, during the COVID-19 pandemic compared to before the pandemic and for newly diagnosed BC, there has been seen to be a significant decrease of 66%5. In the present study, a 13% decrease was detected in newly diagnosed BC cases over the 17-month period during the pandemic compared to the same time span before the pandemic.
The TNM classification for BC was updated in 2017 by the Union for International Cancer Control6. In a study evaluating NMIBC patients using the new TNM classification, 5-year disease-specific survival (DSS) was found to be 98.5% in TaG1 patients and 88.7% in T1G3 patients7. In another study evaluating MIBC patients, 5-year DSS after radical cystectomy was found to be 75-80% in organ-restricted T2 patients8. Muscle invasion in BC is an important prognostic factor for mortality. In the present study, a significant difference was determined between the groups in terms of T stage (p = 0.04), but not for the presence of CIS (p = 0.2). There was an increase in the high grade rate, but this increase was not statistically significant (p = 0.3). A substantial proportion of the primary BC patients who presented during the COVID-19 pandemic had lower Ta and higher T2 (MIBC) stages. As a result, it was thought that such patients may have poor prognostic factors in the medium/long term in terms of progression and DSS due to hospital presentation at an advanced stage during the pandemic.
According to the EAU NMIBC risk stratification, a significant difference was detected between the groups in terms of EORTC risk stratification with a substantial increase in the rate of very high-risk patients observed during the pandemic (p = 0.02). There are scoring systems for estimation of recurrence and progression in NMIBC patients. In a previous study, tumor count, tumor size, number of recurrences in a year, tumor T class, presence of CIS, and tumor grade were reported as critical prognostic factors for risk scores9. In the present study, factors that influence recurrence and progression were evaluated and scores were calculated. The EORTC recurrence score was median (min-max), 9 (0-14) for the COVIDBC group, and 6 (0-13) for the Pre-COVIDBC group. The EORTC progression score was 9 (0-19) for the COVIDBC group and 5 (0-15) for the Pre-COVIDBC group, with a significant difference determined between the groups for both scores (p < 0.01 for both). A significant increase in NMIBC very high-risk patient rate, recurrence, and progression score can result in serious oncological consequences without the early treatment or regular follow-up.
In BC patients, the progression rate increases with disease duration, indicating that a delay in presentation or treatment may cause a progression in the disease stage. In the present study, symptom duration at initial presentation was found to be significantly longer during the COVID-19 pandemic compared to the pre-pandemic group (p = 0.04). The reasons for the delay in admission to the hospital during the 17-month pandemic period may have been patient anxiety, the prolongation of the referral period, and the longer waiting time in the hospital or the cancellation of appointments, but for whatever reason, further prolongation of this process may lead to the possibility of disease progression.
In the present study, the time between diagnosis and TURBT surgery in the COVIDBC and Pre-COVIDBC groups was 30 ± 21 days and 12 ± 6 days, respectively, and the difference between the groups was significant (p < 0.01). All patients diagnosed with pre-operative BC were prepared for surgery under the same conditions without risk classification, and no patient was referred to an external center. This eliminated the paradoxically more rapid access to care for some high-risk patients. All surgeries were performed in our center, but as in many centers, due to the decrease in the number of operation rooms during the pandemic period, there was a decrease in the average number of surgeries per day. This resulted in a prolongation of the time between diagnosis and operation. The literature on NMIBC investigating the effects of delayed intravesical treatment is limited, although in a study which compared early cystectomy with late cystectomy in high-risk NMIBC patients, it was found that a lengthy delay may influence survival and that cancer-specific survival (CSS) might be reduced in patients with cystectomy delayed for 13 months or longer10. However, in respect of MIBC, there are numerous studies which have investigated the potential outcomes of delayed surgery. In a study of MIBC patients, it was found that a delay in treatment of longer than 10 weeks is associated with poor CSS and overall survival (OS) outcomes11. These results suggest that even though the delayed times in the current study were shorter than the stage progression times in the literature, due to the limited surgical capacity during the COVID-19 pandemic, prolonging the time from diagnosis to surgery even more than stated in the available data may result in poor survival outcomes in BC patients.
The EAU Guidelines Office Rapid Reaction Group has published a guideline that evaluates disease priorities to adapt EAU recommendations for the COVID-19 pandemic4. In the present study, it was planned to repeat the initial cystoscopy at the end of the 3rd month in all patients and patients without follow-up were defined as those who were not admitted for cystoscopy control within the first 6 months. The rate of follow-up was 68.2% and 80.8% in the COVIDBC group and Pre-COVIDBC group, respectively (p = 0.03). The 3rd month control after TURBT is an important prognostic indicator for recurrence and progression12. Not implementing this may prevent the prediction of recurrence and progression during follow-up visits and may cause poor oncological outcomes by leading to delayed early diagnosis and treatment.
The diagnosis of BC is usually made after the examination of patients presenting with gross hematuria (GH) or microscopic hematuria. GH as the presenting symptom in newly diagnosed BC patients has been found to be associated with higher pathological stage13. In the present study, the rate of presenting with GH in the COVIDBC and Pre-COVIDBC groups was 82.8% and 70.1%, respectively, with a significantly higher rate detected during COVID-19 pandemic (p = 0.04). This was supported by the significantly higher pathological stages. Obstructive nephropathy (ON) is a common cause of acute kidney insufficiency (AKI), accounting for 5-10% of overall AKI cases, and up to 22% in an older population14,15. In cases where AKI is associated with malignancy, ON-induced AKI is seen in nearly 10% of cases16 with higher mortality than that seen in patients without ON17. In the present study, data on ON were investigated and a significant difference was detected between the COVIDBC and Pre-COVIDBC groups in terms of the degree of hydronephrosis (p = 0.04). These data suggest that the prevalence of ON may have increased in the diagnosis of primary BC during the pandemic period and higher morbidity and mortality rates may have been due to AKI. Although the rates of GH and ON substantially increased during the COVID-19 pandemic, no difference was determined in terms of presenting hemoglobin and creatinine values (p = 0.7 for both).
The most important limitations of the present study were the short follow-up period to standardize the factors that influence tumor recurrence and progression, and the retrospective evaluation of patients diagnosed before the COVID-19 pandemic. A larger population with longer follow-up is required to prove whether the pandemic had additional adverse effects on survival outcomes. Multicentric studies are needed to increase the sample size and obtain more conclusive results. However, during the pandemic, it was not possible to conduct a multicentric study, since only certain centers performed the surgery and follow-up of urological oncology cases and our center was a COVID-19 reference center.
Conclusions
The results of this study demonstrated that the number of newly diagnosed primary BC patients decreased during the COVID-19 pandemic compared to before the pandemic. BC patients diagnosed during the pandemic were mostly at higher stages (T2) and higher risk in NMIBC patients. The increase in muscle invasive (T2) BC and high-risk NMIBC patients can be considered to have increased subsequent morbidity and mortality rates. The recurrence and progression scores and time to surgery from diagnosis also substantially increased. Therefore, the importance of the early surgical intervention should be emphasized and care must be taken not to delay the treatment period. There is also a need for more awareness of alternative treatments for patients who do not accept or are not suitable for early cystectomy. Symptom duration on presentation was significantly longer, and there was a considerable increase in the prevalence of GH and obstructive nephropathy on presentation. During the pandemic, the rate of follow-up significantly decreased among BC patients. The transformation of health-care services and increased attention of the population to avoid disease exposure during the pandemic might have led to the decrease in hospital presentations and prolonged time to surgery from diagnosis.

