











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
The clinical evaluation of a patient aged > 40 years who presents with a destructive bone lesion includes a detailed patient history, physical examination, imaging workup, biopsy strategy, and final staging. The differential diagnosis includes metastatic bone disease, multiple myeloma, lymphoma, primary malignant bone lesion, and non neoplastic conditions. Metastatic bone disease is the most common diagnosis of a destructive bone lesion in patients aged > 40 years.1
Clinical case
An 86-year-old woman, referred by her family doctor to our centre, presented with a 3-month history of persistent swelling and pain in her left arm. She was treated for myofibroblastic sarcoma of the maxilla a year before (surgical excision and radiotherapy). Three months before the beginning of the symptoms, she suffered a diaphyseal humerus fracture after a minor trauma, which was surgically treated in another centre (Figure 1). She did not have symptoms of a recent fever, chills or night sweats, but her family reported weight loss of more than 10 kg in the last 3 months.

Upon physical examination, the left arm was swollen and painful when palpated. There was no overlying skin abnormality such as erythema, ecchymosis or warmth. Pulses were palpable and the sensation was normal. There was a surgical scar in the posterior distal aspect of the arm.
The laboratory results, including complete blood count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), electrolytes and coagulation studies were completely normal.
X-ray at presentation showed a complete and angulated fracture of the humeral diaphysis within a poorly marginated lesion, which is a typical feature of a pathologic fracture (Figure 1). The second radiograph performed three months later, showed a complete destruction of almost all the left humeral diaphysis (Figure 2), with intramedullary pins inside the bone, and soft tissue enlargement.
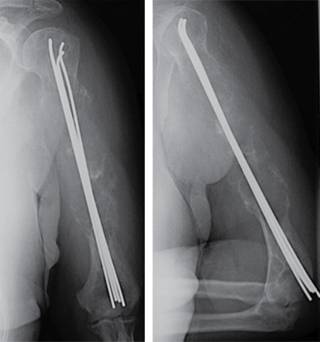
Figure 2: AP radiograph of the humerus which shows intramedullary pinning and gross bone destruction.
Computed tomography (CT) scans of the chest, abdomen and pelvis were obtained showing two nodules in the left lung likely consistent with metastatic disease.
Scintigraphy showed increased uptake in the third and eighth left ribs and the whole left humerus, consistent with bone metastases. At this point, the main clinical entities included in the differential diagnosis are:
Multiple myeloma
Lymphoma
Primary bone sarcoma
Non-neoplastic conditions such as osteomyelitis or brown tumor from hyperparathyroidism.
Metastatic bone disease
We decided to perform a core needle biopsy under X-ray control which was insufficient, so, we performed an open biopsy.
Histology interpretation
Macroscopically, the lesion was approximately 1.5 cm in diameter, grey-white, hard and fibrous. There was no necrosis. Microscopically, a bone involvement by spindle-shaped tumour with herringbone growth pattern was observed. Tumour cells have a pale or pink cytoplasm and fusiform nuclei with small nucleoli (H-E stain) (Figure 3). Most tumour cells showed low-grade atypia. The mitotic index was low (< 5/10 HPF). Tumour cells stained positively for smooth-muscle actin (Figure 3). The final diagnosis was metastatic low-grade myofibroblastic sarcoma of the maxilla.

Figure 3: Bone involvement by spindle-shaped tumor with herringbone growth pattern. Tumor cells have pale cytoplasm and fusiform nuclei with small nucleoli. H-E.

Evolution
Our patient was misdiagnosed at the time of the humeral fracture, and was treated for a typical humeral fracture using and intramedullary pinning (Hackethal technique), producing the progression of the disease within the humeral shaft. Due to the end state of the disease (multiple metastases), we decided to perform a palliative treatment with local radiotherapy and we put an arm brace after removal of the hardware. At nine months follow-up the patient showed an improvement of symptoms, with less pain. The radiological exam showed a good response to radiotherapy, with ossification of most of the humerus, although several fractures were observed as well as a shortening of the humerus (Figure 4).

Discussion
The initial presentation of a pathologic fracture may be misconstrued as a benign process,2,3,4 delaying a diagnosis of malignancy. After the initial radiographs, multiple imaging techniques such as CT and MRI, should be used for further evaluation.
Multiple myeloma (MM) is a systemic disease that affects the bone marrow. Occasionally, patients have solitary lesions without marrow involvement, called plasmacytomas. The bone lesions in myeloma are identified by skeletal survey and present as round, punched-out osteolytic areas in the extremities, pelvis, and spine. Laboratory studies including serum and urine electrophoresis with inmunofixation confirm the diagnosis. Moreover, patients present with anaemia and elevated beta 2 microglobulin and lactate dehydrogenase levels.1 However, our patient’s lab results were strictly normal. A technetium Tc-99m total body scan is helpful in identifying additional bony sites of disease, but it may indicate a false negative result in the patient with multiple myeloma because this study detects only osteoblastic activity, so, although multiple myeloma is typically occult on bone scan, some lesions can have uptake.
Lymphoma in bone can manifest as (1) metastases from systemic lymphoma or as (2) primary lymphoma of bone which is more uncommon and by definition should not have systemic disease. The metastatic form is usually radiographically occult; however, the B cell subtype of primary lymphoma often has extensive bone destruction and a large soft tissue component similar to the lesion in this case. In a typical scenario, the patient presents extensive lymphadenopathy and a soft tissue mass.1,5,6 In contrast, our patient had no lymphadenopathies and the bone lesion was unique.
Primary malignant bone tumours, such as chondrosarcoma, osteosarcoma and malignant fibrous histiocytoma can occur in the patient aged > 40 years. All these tumours have unique characteristics depending on the specific diagnosis.5,7
Much further down the list are destructive benign bone lesions, that can also occur in adults but more often in younger patients than our case.
Non neoplastic conditions, including hyperparathyroidism, osteoporosis, osteomyelitis, metabolic bone disease, and Gorham vanishing bone disease, can cause osteolytic lesions or pathologic fractures. Determination of erythrocyte sedimentation rate and C-reactive protein level may be helpful when osteomyelitis is included in the differential diagnosis.1
Metastases to bone are the most frequent cause of destructive lesions to the skeleton in adults.7 The tumours that are most likely to metastasize to bone are mainly carcinomas of prostate (32%), breast (22%), kidney (16%), lung and thyroid.6 The typical distributions of metastatic lesions are to the spine, ribs, pelvis, and proximal limb girdles.1 The humerus is the second most common site for long bone metastases, behind only the femur in its frequency of involvement.5,7,8 It represents 20% of all bony metastases.
Metastatic bone sarcomas are very uncommon. Unlike carcinomas, bone sarcomas disseminate almost exclusively through the blood. Hematogenous spread of extremity sarcomas is manifested by pulmonary involvement in the early stages (up to 20% of the cases) and by bony involvement in later stages.9 Low-grade soft-tissue sarcomas have a low (< 15%) rate of subsequent metastasis while high-grade lesions have a significantly higher (> 15%) rate of metastasis. Metastases from sarcomas to regional lymph nodes are infrequent; the condition is observed in only 13% of patients with soft-tissue sarcomas and 7% of bone sarcomas at initial presentation. The prognosis associated with such an event is similar to that of distant metastasis.10,11
Metastases to the long bones usually reflect an advanced disease state. It has been recommended that the majority of patients with metastatic bone tumours receive multidisciplinary care from a team including orthopaedic oncologists, radiotherapists, and oncologists.7,12,13
Diagnosis of metastatic humeral bone lesions and alternatives for treatment vary depending on whether the patient has a large impending lesion or complete fracture, which region of the bone is affected, the extent of the overall disease, the histologic diagnosis, and the nature of prior treatment.7 Intramedullary stabilization is a reliable method for fixation of pathologic fractures of the humerus for patients in the advanced stage of metastatic disease.14 Postoperative external beam irradiation is necessary to prevent progressive bone destruction and subsequent loss of fixation.15
Tumours of the jawbone are among the most uncommon of all types of neoplasms and represent a distinct group of lesions from the conventional type commonly occurring in long bones. Nonetheless, our present knowledge of this tumour allows us to affirm that its clinical behaviour and pathologic features differ markedly from those of its homologous in the long bones.15,16,17 Low-grade myofibroblastic sarcoma represents a rare entity, which mostly develops in the soft tissues of the head and neck.15 Within the oral cavity lingual lesions are the most common and they tend to recur locally rather than to metastasise. When this tumour spreads to the bones it produces a well-demarcated osteolytic lesion with no periosteal reaction.16 Diagnostic methods include immunohistochemistry and molecular investigations. We would like to emphasize the uncommon location of this tumour type (within the maxilla) and its aggressive evolution (metastasis) though the low-grade histopathologic pattern; Guillou, et al tried to predict the likelihood metastasis of low-grade myofibroblastic sarcomas:13 a high malignancy grade (high mitotic index), a tumour size of > 10 cm and a deep location increase the tendency for metastasis.
The prognosis for patients with metastatic disease of a myofibroblastic sarcoma appears to be determined largely by the site(s), the number of metastasis, as well as the surgical resectability of the metastatic disease.2,8,13,14
Conclusion
This particular clinical case does confirm that is very important to rule out a malignancy in cases of fractures after minor trauma or in cases of osteolytic or poorly marginated lesions, particularly in patients older than 40 years of age. Therefore, it is imperative that the treating physician has a rational and effective approach to the diagnostic evaluation and treatment of these patients in order to avoid a misdiagnosis.

