











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
With physical inactivity classified as a global pandemic since 2012, the World Health Organization (WHO) has established that increasing physical activity (PA) is of primary importance as a pathway to achieving health benefits and reducing risk factors, particularly chronic diseases such as arterial hypertension1. The main recommendations of the WHO for increasing the PA levels of the population include 150 minutes of moderate PA, 75 minutes of vigorous PA or an equivalent combination of both per week. Previous studies2 have concluded that PA effectively reduces blood pressure up to 5-7mmHg in hypertensive and 3-5mmHg in normotensive patients. Given this, clinical practice guidelines prescribe increasing PA either as part of the non-pharmacological treatment3 or alongside the pharmacological treatment of arterial hypertension2.
While physical inactivity is more prevalent in high-income countries, the burden of disease and related costs is higher in low-and middle-income countries, including Mexico4. This situation -coupled with the limited availability of resources that health systems require to manage the highly diversified phenomena to which they must respond-demands an efficient allocation of available resources in programs that reduce the burden of physical inactivity in the population. However, according to the National Institute for Health and Care Excellence (NICE)5, over 60% of the world’s population has yet to reach the minimum PA time recommended6. In Mexico, only 42.4% of the population aged 18 years and over played a sport for leisure in 2017, scarcely more than in 2016 (41%)7 and 14.4% of adults failed to comply with the PA recommendations of the WHO8. During that same year, insufficient PA cost healthcare systems around the world 53.8 billion international dollars and the Mexican healthcare system 885,614 international dollars4. It was also responsible for 13.4 million disability-adjusted life years (DALYs) worldwide, 41.5% and 33.3% of which were attributable to low-and middle-income countries, respectively. Latin America accounted for 8.6% of the global estimate, with 2.4 DALYs per capita.
Coupled with limitations in the health system, achieving changes in lifestyles as it is physical activity among the healthy population and even more in population with chronic health conditions requires a theoretical approach to understand underlying characteristics that determine a person’s behavioral change. Therefore, the challenge for physical activity promotion is to increase the engagement in PA programs addressing both the adherence and behavior- change barriers, incorporating psychological theories through behavioral models9, and adapting the intensity and variety of the programs to match the preferences of the individuals. Considering these main challenges, one of our PA programs was developed based on the Transtheoretical Model10 and Social Cognitive Theory11. On the other hand, the Brief Counseling PA program includes an approach tailored to health services12. In addition, and to reinforce the approach on which PA programs are based, we compared the Brief Counseling and Reference Scheme initiatives for achieving the WHO PA target at the primary level of care.
The need to make decisions in an environment marked by uncertainty, scarcity and competitive priorities renders cost-effective analysis (CEA) an attractive instrument for public health policy planning13. It allows for comparing the costs and benefits of health interventions, thus providing a valuable economic evaluation technique and a tool for developing maximum efficiency in allocating scarce health sector resources14. The economic evaluation programs designed by high-income countries to promote PA have not been adopted by low- and middle-income countries13,15,16,17. It is first necessary to generate conclusive evidence for decision-making in contexts where the population’s health behaviours and the structure of health systems are different.
The Mexican Social Security Institute (IMSS), which serves approximately 58 million affiliates18, faces a complex financial situation owing to the demographic and epidemiological transitions of the Mexican population18. Salient among its financial challenges are the high costs of health services required for chronic-degenerative diseases such as arterial hypertension18. Therefore, the IMSS emphasized prevention, mainly promoting healthy lifestyle changes as a pathway to positive health outcomes among its affiliates. The IMSS has its own resources to provide PA programs, which includes facilities designed to develop PA programs (sports fields, gyms, pools and outdoor spaces for PA) called Social Security Centers (SCC). The SCC have specialized staff to guide and assist on promotion and practice PA to the affiliated population interested in carrying out physical activity programs. In addition, physicians working at the primary care level should have knowledge and willingness to identify potential candidates for these PA programs. However, an effective link between the medical area and resources and staff working in the SCC is missing. Therefore, this study is part of a research project joining the efforts in the institution to address the physical inactivity of the hypertensive population through the assessment of two different PA programs proposing its organization and implementation using the resources available at the institution.
In light of the situation described above, the objective of this study was to perform a CEA of two programs designed to increase the PA of hypertensive patients at the primary- care level: the first based on the Reference Scheme (RS) and the second on the Brief Counseling (BC) approach, both within the context of a social security institution having the necessary infrastructure and personnel to implement them.
Material and Methods
We performed a CEA of two programs aimed at increasing the PA of hypertensive patients in IMSS primary-care facilities. The analysis was conducted from the perspective of service providers, with a time horizon of 24 weeks. We included direct costs only. Costs were adjusted with the 2018 Consumer Price Index19 and converted to US dollars (1 US$=19.65 Mexican pesos)20. Neither the costs nor the effectiveness of the programs was discounted given our brief one-year time horizon.
A detailed description of the programs can be found elsewhere21. Basically, under the RS intervention, patients were instructed to perform one hour of PA, adapted to their specific conditions and guided by a PA instructor at the Social Security Center (SSC), a sports facility within the IMSS service network. The Brief Counseling intervention (a 15-minute talk by a nurse on the benefits of PA) was implemented with patients exiting their regular medical consultations.
The programs were carried out in four randomly selected primary-care facilities (PCFs): two for the RS and two for the BC intervention. Patients assigned to the first received PA recommendations at their respective PCFs and executed the indications at the SSC. Our sample included 232 patients (RS= 117, BC= 115). None were compliant with the PA recommendations of the WHO, and all met the study inclusion criteria22.
We estimated two effectiveness metrics between the commencement (week zero) and the conclusion (week 24) of each program: minutes of moderate-vigorous PA (MVPA) and the percentage-point difference in patients performing MVPA for ≥150 minutes weekly22. We estimated both measures of effectiveness from primary data collected during the study mentioned above.
Based on the micro-costing technique, we counted, monetized and integrated the resources required for all intervention activities to estimate their total costs (TC)23. To calculate the cost of RS implementation, we applied the following formula:
We added the unit costs (UC) of four medical consultations (MC), the SSC admissions (SSCA) and examinations by a medical technical advisor (MTA), 48 PA sessions (PAS) and the collection of three blood samples for clinical laboratory tests (Labs). To estimate the TC of the BC intervention, we applied the following formula:
We used primary and secondary data to calculate the costs of personnel, supplies, utilities (e.g., water, electricity), and fixed assets (e.g., equipment, buildings) related to SSCA, MTA examinations, PAS and BCS. The MC and Labs unit costs were obtained from secondary data available at IMSS24. To estimate the cost of personnel, we multiplied the fraction of time spent on each program activity by earned wages, assuming an eight-hour working day journey and 20 working days a month. To estimate multiple salary categories, we used averages. We ascertained the time dedicated to the interventions through interviews with personnel. The fraction of salary earned was calculated according to the salary structure in force at IMSS during the study25.
We estimated the supply costs by multiplying the amounts used for each patient by their acquisition prices. Similarly to the time spent on intervention activities, the type and amount of each input were determined through interviews with the corresponding service providers. Input prices were obtained from the official 2017 procurement catalogs24. In the case of utilities, we prorated the annual expenditure on electricity, telephone, and drinking water among the different IMSS departments and patients using the SSC and PCFs. The IMSS administration department24 provided this information. To estimate the cost of the fixed assets, we calculated their equivalent annual cost23,26, gathering information on their categories, acquisition prices/year, useful lives, and resale values from the IMSS administrative files24.
After estimating the total costs and effectiveness for both programs, we calculated their average cost-effectiveness and incremental cost-effectiveness ratios (ICER). Uncertainty in the ICER -due to the multiple sources employed for its calculation- was propagated with a probabilistic sensitivity analysis using a Monte Carlo simulation with 5000 iterations27. In each iteration, the ICER was calculated based on the values taken by our parameters of interest, randomly sampled from a probability density function (pdf). This procedure was performed simultaneously for all parameters while recording the ICER results.
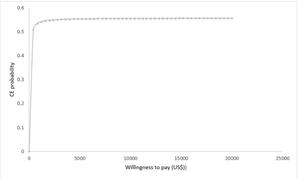
The effectiveness of the programs was represented with beta pdfs. These functions were empirically estimated using nonparametric resampling (i.e., bootstrapping) based on primary data28,29collected from patients during the study mentioned above22. The SSCA, MTA, PAS and BCS costs were represented by normal distributions30. We assumed fixed costs for MC and Lab; this is, we did not use pdfs to represent them. The results were presented graphically on a cost-effectiveness plane and a cost-effectiveness acceptability curve23,31,32.
Results
Costs
Table 1 shows the total costs of both programs. The unit cost (UC) of the RS was estimated at 456.50 US$, with the UC of the PA sessions being proportionally the most important (62.3%; 284.2 US$), followed by the medical consultations (31.7%; 144.6 US$). The BC program had a UC of 172.20 US$, with the UC of the medical consultations being the most important (84%). The UC of the counseling session represented 7% (12.10 US$) of the total. The TC of the RS was 2.7 times greater than that of the BC program.
Table 1 Unit costs of the Reference Scheme and Brief Counseling programs to increase physical activity of hypertensive patients.
| Activity | Unit cost* | |||
|---|---|---|---|---|
| RS | % | BC | % | |
| Medical consultation | 144.6 | 31.7 | 144.6 | 84 |
| Admission to the Social Security Center | 5.3 | 1.2 | NA | NA |
| Examination by a medical technical advisor | 6.8 | 1.5 | NA | NA |
| Physical activity sessions | 284.2 | 62.3 | NA | NA |
| Clinical laboratory tests | 15.5 | 3.4 | 15.5 | 9 |
| Brief counseling sessions | NA | NA | 12.1 | 7 |
| Total^ | 456.5 | 100 | 172.2 | 100 |
*In 2018 US dollars (1 USD=19.65 MXN) ^The figures for individual activities may differ from the totals because they were rounded. NA: Not applicable; RS: Reference Scheme; BC: Brief Counseling Source: Compiled and designed by authors
Effectiveness
On average, RS patients performed 14 minutes less of PA than BC patients by the end of the programs. That is, while RS patients performed 8.1 additional minutes of PA (week 24 = 169.29 minutes; week zero = 161.23), BC patients performed 22.1 additional minutes (week 24 = 154.12 minutes; week zero = 131.98). In analyzing the percentages of patients who performed ≥150 minutes of MVPA a week, we found that the percentage in the RS program was 45.29%, while those in the BC program were 44.3%. This implies that, on average, 0.95% more RS than BC patients completed ≥150 minutes of PA per week (see Table 2).
Table 2 Average and incremental cost-effectiveness ratios of PA promotion through the Reference Scheme programs
| Program | Total cost (TC)* | Incremental cost (TCRS - TCBC)* | Effectiveness (Ef)^ | Incremental effectiveness (EfRS -EfBC)^ | ACER (TC / Ef) | ICER (TCRS - TCBC) / (EfRS - EfBC) |
| 1. Increase in total minutes of PA | ||||||
| RS | 456.5 | - | 8.1 | - | 56.4 | Dominated |
| BC | 172.2 | 284.2 | 22.1 | -14 | 7.8 | |
| 2. Increase in patients performing ≥150 minutes of PA/week | ||||||
| RS | 456.5 | - | 45.29 | - | 10.1 | - |
| BC | 172.2 | 284.2 | 44.34 | 0.95 | 3.9 | 299.2 |
*In 2018 US dollars (1 USD=19.65 MXN) ^Effectiveness units: (1. Increase in total minutes of PA) minutes; (2. Increase in patients performing ≥ 150 minutes of PA/week) percentage points PA. Physical activity; RS: Reference Scheme; BC: Brief Counseling; ACER: average cost-effectiveness ratio; ICER: incremental cost-effectiveness ratio. Source: Compiled and designed by authors
Cost-effectiveness
The ratios for average and incremental cost-effectiveness are shown in Table 2. The BC program surpassed the RS program, i.e., it was more expensive (284.20 US$) and less effective (-14 minutes) in increasing the average number of minutes of PA among patients. On the other hand, given that the RS was slightly higher than the BC intervention in terms of the percentage of patients performing ≥150 minutes of MVPA (0.95%), we estimated the ICER at 299.20 US$ for each percentage point increase of patients complying with recommendations for PA.
Sensitivity analysis
After propagating the uncertainty associated with the cost and effectiveness parameters presented in Table 3, we generated the diagrams shown in Figures 1 and 2. Figure. 1 illustrates the ICER dispersion after 5000 iterations from the Monte Carlo simulation. Of the total, 56% (n=2,834) were in the northeast quadrant of the plane, meaning RS is a more effective and expensive program than BC. We found that the RS had a maximum probability of ≈55% of being cost- effective relative to BC (Fig. 2), which was reached at 247 US$ per percentage-point increase of patients performing ≥ 150 minutes of PA weekly.
Table 3 Parameters included in the sensitivity analysis
| Parameter | Point estimate | Distribution | SD / α, β | Source |
|---|---|---|---|---|
| Costs* | ||||
| Medical consultations | 144.59 | Fixed value | NA | IMSS, 2017 |
| Clinical laboratory tests | 15.53 | Fixed value | NA | IMSS, 2017 |
| Admission to the Social Security Center | 5.34 | Normal | 0.4 | Assumed¬ |
| Examination by a medical technical advisor | 6.82 | Normal | 3.01 | Assumed¬ |
| Physical activity sessions | 284.08 | Normal | 27.75 | Assumed¬ |
| Brief counseling sessions | 12.09 | Normal | 0.81 | Assumed¬ |
| Effectiveness Patients performing ≥150 minutes of PA/week after 24 weeks (%)^ | ||||
| Reference Scheme | 45.29 | Beta | α= 52.87; β= 63.87 | Empirical estimates based on primary data from Gallegos-Carrillo et al. 2017 |
| Brief Counseling | 44.3 | Beta | α= 66.04; β= 82.91 | Empirical estimates based on primary data from Gallegos-Carrillo et al. 2017 |
*In 2018 US dollars (1 USD=19.65 MXN) ^This value was taken only at week 24 of the programs given that, at week 0, the patients did not comply with ≥150 minutes of PA per week. --Briggs, 2002 °Standard deviation (SD) was used to simulate a normal distribution of costs; alpha and beta values were used to simulate beta distributions, as can be seen in the table. Source: Compiled and designed by authors
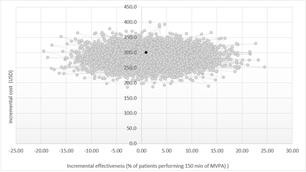
Figure 1 Percentage of patients complying with the WHO physical activity recommendation Costs in 2018 US dollars (1 USD=19.65 MXN) MVPA: moderate to vigorous physical activity. Note: The black dot indicates the point estimate of the ICER. The gray dots represent the simulated ICERs (in Monte Carlo simulations) after 5000 iterations. Source: Compiled and designed by authors
Discussion
The Reference Scheme program proved more expensive than the Brief Counseling program. This is consistent with studies conducted in other settings, such as the United Kingdom16, where the Reference Scheme program was more costly than brief counseling for hypertensive patients after a year. Additionally, the Reference Scheme program did not increase the minutes of physical activity compared to the Brief Counseling program. Finally, we estimated a maximum probability of around 55% that the Reference Scheme program would be cost-effective in increasing the percentage of patients performing ≥150 minutes of MVPA per week.
Although we were able to identify some differences between the RS and BC programs, there is a need to obtain further evidence on both strategies to complement these results, especially as in other contexts, RS was found to be more cost-effective than BC33. Moreover, evidence indicates that RS is cost-effective regarding alternative outcomes such as lessening depression and anxiety; accordingly, social contact and the support patients enjoy in the assistance offered by this scheme may be its beneficial features as opposed to an increase in PA per se33.
The cost-effectiveness estimate in RS is sensitive to small changes in its components, namely effectiveness and cost measures. Consequently, it is subject to a certain degree of uncertainty, mainly due to the limited evidence of effectiveness found in the present study17. The RS program ensures that patients comply with the recommended WHO guidelines. However, it does not increase the minutes of PA they perform. This discrepancy is not rare in cost-effectiveness analyses of physical activity programs, given the variety of outcomes used to obtain cost-effectiveness ratios. A particular strength of the present study is to account for uncertainty in all the parameters used in the ICER estimation probabilistically. By calculating empirical probabilistic functions for physical activity programs, our study also presents evidence to inform model-based economic evaluations on the long term consequences of implementing such programs. Nevertheless, future efforts might benefit by including clinical outcomes such as blood pressure lowering, more relatable to decision- makers in healthcare contexts.
Another strength of our study pertains to data acquisition. In previous studies33, participants have self-reported their physical activity levels using the International Physical Activity Questionnaire (IPAQ)34. In turn, we measured physical activity objectively, using accelerometry35,36. It has been previously shown that data collection relying on self- reporting may overestimate participants’ physical activity levels compared to more objective measures37. What is more, evidence also indicates that interventions using subjective data collection methods typically appear to be more effective than those relying on objective collection methodologies38, given that adults tend to over-report their physical activity levels on the IPAQ as compared with measurements from accelerometers39,40,41. Groups such as the Public Health Advisory Committee at NICE have highlighted the value of collecting more accurate data to inform their investment decision-making.
The duration of a physical activity program might influence its effectiveness38. Some authors42 have noted that PA levels show no significant gains in the short term and that the costs of these programs are higher than for programs with a longer timeframe. Our results indicate that the RS program is not cost-effective compared to BC, which adds to the mixed evidence on the cost-effectiveness of RS programs, albeit gathered through studies conducted in high-income countries43. This could be probably due to the various methodological designs of these studies, which have used different populations, outcome measures, and timeframes. These differences imply the necessity of obtaining further evidence from studies of both programs in low- and middle- income countries as they concern healthcare institutions in these contexts.
The present study offers information on the efficiency of using RS to foster PA in recently diagnosed hypertensive patients in a middle-income country. The environment in which people are embedded might determine whether they will undertake physical activity. For instance, evidence shows that low or decreasing physical activity levels are usually related to a high or growing gross national product6. Hence, beyond individual characteristics, consideration of institutional and contextual factors in the prevention and control of non-communicable diseases is crucial44.
The present study has some limitations. To the best of our knowledge, this is the first cost-effectiveness analysis of programs promoting physical activity among patients with a chronic illness in the primary level of care of a social security institution in a middle-income country. A crucial element of our evaluation was the analysis of costs using a highly accurate methodology based on micro-costing, which provides detailed quantification of resources for every stage in each program and includes the perspective of service providers. While the literature on economic evaluation recommends conducting analyses from a societal perspective, we had no data to estimate indirect costs for participants (i.e., productivity losses) in this study. Nevertheless, conducting an analysis from the third payer perspective is helpful as it contributes direct evidence for undertaking formal decision- making processes at the institution level. The leverage provided by the study might help IMSS and other similar institutions accounting for the resources needed to provide their affiliate base with interventions that address their organizational circumstance.
Secondly, baseline physical activity levels were self- reported by patients during the selection process and differed from the initial readings obtained via accelerometry. That is, in completing the IPAQ and an additional questionnaire administered to them by their attending physicians at the beginning of the program, patients reported not having complied with PA recommendations. However, upon performing the initial measurements using accelerometry, it was found that the selected patients who self-reported being sedentary had complied with the physical activity criteria. Previous studies of PA have established that the more active patients are at the beginning of a PA program, the less they will be found to have benefited from it at the end45. However, according to the Transtheoretical Change Model, patients who self-identified as physically inactive should not be excluded from PA programs.
Conclusions
Our results indicate that in the context of a social security institution such as the IMSS, it is not cost-effective to implement an RS-based program to increase physical activity levels in hypertensive patients. Given that physical activity has positive effects in reducing high blood pressure, we analyzed a population of patients recently diagnosed with hypertension (5 years or less), hoping that they would be more committed to increasing their physical activity levels than other individuals, and considering that the challenge for physical activity promotion is to increase the engagement in PA programs addressing both the adherence and behavior- change barriers. However our results cannot be extrapolated to a different type of population, given the nature of our sample. Although there is some uncertainty on the allocative efficiency of the Referral Scheme, it is crucial to continue analyzing physical activity programs to offset the economic burden imposed by physical inactivity on healthcare institutions in all contexts. Additionally, it is important to generate evidence from this type of analysis, addressing diverse measures of effectiveness in both improving the physical conditions of individuals and tackling disease. It is necessary to evaluate public health programs to keep balance between the spent resources and benefits obtained, to provide maximum health benefits for the population

