










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista odontológica mexicana
Print version ISSN 1870-199X
Rev. Odont. Mex vol.19 n.1 Ciudad de México Jan./Mar. 2015
Original research
Range of mandibular movement in six-year old children with early mixed dentition
Fabiola Adriana García Dueñas,* María Leonor Alonzo Echeverría,* Gabriel Eduardo Colomé Ruiz,* Rubén Herrera Atocha,* Salvador Medina Peralta,§ Rocío Acosta Pech§
* Orthodontics and Maxillofacial-Dental Orthopedics, School of Dentistry.
§ School of Mathematics.
University of Yucatan, Mexico.
ABSTRACT
Measurement and examination of mandibular movements are procedures considered within any clinical diagnosis. Reports on these ranges are quite widespread for adult patients, but little has been written on the subject when dealing with children. The aim of the present study was to determine range of mandibular movements in six year old schoolchildren in Mexico. Data were collected on 52 six year old children. In this sample, 52% were female and 48% male. With the χ2 goodness of fit test to uniform distribution or equal proportions, differences between the following categories were examined: opening pattern, midline deviation and deviation in opening and closing. It should be noted that for the present test zero frequency category was excluded from the opening pattern. Due to the breach of normality assumption, Wilcoxon test was used for dependent samples in the comparison of unassisted and assisted maximum opening, t test for dependent samples was used to compare left and right laterality. Opening patterns differed significantly (χ2 = 60.9231, p < 0.0001, gL = 3) straight 71.1%. Uncorrected right lateral deviation 0%, right corrected «S» deviation 13.5%; uncorrected left lateral deviation 1.9%, and corrected left «S» deviation 13.5%. Average of non assisted maximum opening was 35.00 mm when compared to maximum assisted opening which was 39.11 mm (T = 0, p < 0.0001). Conclusion: Range of observed mandibular movements in Mexican six year old children with primary mixed dentition was different from same- age children in other regions. This was probably due to the fact that ranks were under the influence of craniofacial, weight, height and size characteristics of each different population.
Key words: Range, mixed dentition, mandibular movement.
INTRODUCTION
In order to establish suitable and healthy masticatory function of permanent dentitions, normal development of primary and mixed dentition is indispensable.
Assessment of mandibular movements is a simple and objective means for the diagnosis of the masticatory system.1-3 Nevertheless, used reference ranks mainly correspond to adult population; information on children population is rather scarce.1,4,5
Range of mandibular movements is influenced by many factors, among which the following can be included: temporomandibular joint, circumstances of muscle structure, ethnic background, age, weight gender and height.1,2,4-9
During growth and development processes, the articular eminence experiences changes in height and inclination. In children with primary dentition, its height is 3.5 mm, it increases with time, reaching 9.4 mm in children and 13.3 mm in adults.10
Some authors have assessed mandibular movement in specific populations: Dr Agerberg undertook to examine Scandinavian children with ages ranging 1-2 years and 5-6 years. Dr Rothenberg did the same with children of ages ranging 4-14 years.6 Dr. Vanderas studied Greek children with ages ranging from 6-10 years. Dr. Cortese examined Argentine children of ages ranging 3-11 years.1 Dr Melo studied Brazilian children ages 6 and 14 years.2
Nevertheless, only Dr H. de Vis undertook a study on mandibular movement ranges in Belgian children with ages comprised between 3 and 6 years, with incorporation of opening and closing pattern analysis.7
The aim of the present study was to record mandibular movement ranges and patterns in six year old children with primary mixed dentition. The reason for the present study was the lack of research on the subject.
METHODS
Measurements were taken of 52 six year old school children who attended 3 different primary state schools in Yucatan, Mexico. Inclusion criteria were children lacking oral appliances.
Establishment of the following factors was sought according to measurung instrument used in the present study: identification of opening pattern, measurement of maximum oral opening (assisted and unassisted), laterality and protrusion, establishment of articular noise present, recognition of type of noise during opening and closing movements as well as during protrusion and laterality movements. Rothenberg6 methodology was used to establish measurement of maximum mandibular opening. This method was considered to be reliable in vertical plane movements. The children were guided into placing the mandible in a comfortable position, they were then asked to open the mouth to their utmost might, without causing pain. The digital vernier caliper ridge was located at the incisive edge of the upper central incisor which was in the most vertical position. At that point, distance between this tooth and the incisive edge of the lower incisor was measured (inter-incisive distance). The specific incisor taken as reference was noted.
DC/TMJD methodology(Diagnosis Criteria for Temporomandibular Joint Disorders) was used to record maximum opening, horizontal protrusion movements and lateralities as well as the pattern of mandibular opening and closing.11
In order to establish recording of maximum assisted opening, the child was requested to place his mandible in a comfortable position, then he was instructed to open his mouth as much as possible, and once the child reached that position, the clinician's thumb was placed cross-wise at the edge of the mandibular central incisors. When in this position, sufficient leverage was obtained to force greater mandibular opening, which finally, with a digital vernier caliper, was vertically measured from the incisive edge of the upper central incisor (reference) to the incisive edge of the lower incisor.
In order to record right and left laterality movements, the child was requested to slightly open the mouth and move the mandible as far as it would go to the right and then to the left. With the help of the vernier caliper, the space from the incisive embrasure of upper central incisors to the interdental space of mandibular incisors was measured. The same instructions were carried out to record protrusion movements: the child was requested to move the mandible to the front, to his utmost might; this was measured with a vernier caliper.
In order to record the opening and closing pattern, the child was requested to position the mandible in a comfortable position ( with teeth in light contact) The clinician's thumb was placed on the child's lower lip, moving it so that lower teeth could be seen; this enabled observation of mid-line deviation. In order to observe opening and closing patterns, the child was requested to open and close his mouth three times. In cases when deviation pattern was not evident, a millimeter rule was used. This rule was vertically held between upper and lower inter-incisive edges (when lines did not match, midline was marked in lower central incisors) as a guide.
Straight: absence of perceptible deviation during opening and closing.
Uncorrected lateral deviation to left or right: unilateral deviations at maximum opening point, direction of mandible deviation was determined.
Corrected deviation to left or right («S» deviation): Unilateral deviation perceptible to one side, nevertheless it was corrected towards the midline before or upon reaching maximum opening.
Other: Presence of irregular movements (not uniform, not continuous) or opening patterns different from the aforementioned; type of deviation was indicated. If the patient exhibited more than one opening pattern, category was used with notation «more than one».
With the χ2 goodness of fit test to uniform distribution of equal proportions,12,13 differences were analyzed among categories of: opening pattern, mid-line deviation, and closure. For this test, zero frequency category was excluded from the opening pattern. Due to the failure of the normality assumption, Wilcoxon's test was used for dependent samples,12 in the comparison of unassisted and assisted maximum opening whereas «t» test was used for right and left laterality for dependent samples.12
Tests were considered significant when p < 0.05; statistical packages used were SPSS 1514and STATGRAPHICS Centurion v. 15.2.06 (StatPoint, 2007).15
RESULTS
Out of the 52 school-age, six year old children which met inclusion criteria, 48% (n = 25) were male and 52% (n = 27) were female. Opening pattern differed significantly (χ2 = 60.9231, p > 0.0001, gL = 3) (Figure 1).
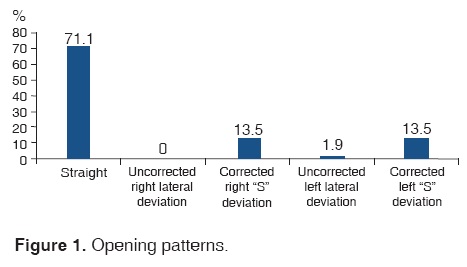
Most children exhibited a straight opening pattern, followed by right and left corrected deviation.
Average of maximum non-assisted opening was 35 mm, when compared with maximum assisted opening which was 39.11 mm (T = 0, p < 0.0001, (Table I). Only one child reported pain when performing assisted maximum opening.
In two children, articular noises were recorded upon right side opening, one child exhibited the same upon left side opening, average opening was 20.80 mm (SD 2.01 mm). One child exhibited a click upon left side closing, with 14.3 mm opening.
Average movement range between right and left laterality was not significant in movement between laterality (t = 0.1431, p = 0.8867, gL = 51) and protrusion movement (Table II).
DISCUSSION
Maximum opening capability found in our study showed concordance with values reported by Ingervall,4 who in his study reported maximum mandibular opening ranges of 37-38 mm in six year old children.
Drs. Okeson, Rothenberg, Cortese, De Vis and Melo de Sousa mentioned that in children from six years onwards, maximum opening ranges were 40 mm or more.
Our results revealed that average of non assisted maximum opening was 35.00 mm when compared with assisted maximum opening which was 39.11. These lower ranges could be attributed to the different methodology we used as well as to the fact that in the present study only six year old children were included. This differs from Dr. Rothenberg6 studies, where children were in age groups 4-14 years, Dr. Cortese1 studies with 3-11 year old children and Dr. Melo de Sousa 2 studies which encompassed children with ages ranging 4-14 years.
Drs. Melo de Sousa, Saitoh and Bonjardim2,10,16 mentioned that differences in mandibular movement ranges were higher in children than in adults. This could be due to variations in weight and stature, which bear strong influence especially in children between 6 and 7 years of age.
We were unable to find extensive data in scientific literature on protrusion and laterality horizontal movements.
In the present study we encountered difficulties when taking laterality and protrusion recordings, since our six year olds found it hard to follow instructions to perform those movements. Other authors equally reported difficulties when recording the aforementioned movements in children under eight years of age.4,16,17
With respect to protrusion and laterality, our study revealed ranges far below the 8-12 mm range reported by Bonjardim in his studies.16
We suggest measurement of the aforementioned movements following Grummons6 methodology. In this methodology, in order to measure protrusive lateral and excursive movements, it is suggested to use the flat section of the tongue as a bite plane in order to allow lateral and protrusion movements in that area, equally allowing preservation of stable vertical dimension.
Nevertheless, Baqaien9 found that previous training was a reliable method undertaken before taking measurements. Both techniques are recommended when taking measurements in small children.
During assessment of mandibular opening and closing patterns, presence and/or absence of one or several lateral movements must be ascertained, since presence of these deviations could indicate a pathological sign of the adult masticatory system. Nevertheless, Nishijima3 mentioned the fact that there was a lateral deviation decrease in mandibular opening and closing movements. This takes place during the child's growth and developments stages, since there is a strong relationship between dentition development stages and neuromuscular development. Baqaien M and Bomjardin9,16 emphasized changes which occur in the condylar sagittal route during protrusion movements in 6-12 year old children. He mentioned that, at age six, inclination of condylar route was 43o to 44o; with a yearly increase of 1o to 3o, proportionate with the child's development. At year 11 inclination was 48o-49o. Therefore, this inclination increase of the condyle's sagittal route will reduce condylar mobility in all directions. In adults this will elicit a straight pattern of mandibular opening. Therefore, in children with early mixed dentition we found deviations as well as straight opening patterns.
In the present study, opening patterns differed significantly. Most children exhibited a straight opening pattern, followed by greater prevalence of corrected left and right deviation.
During mandibular movements recording we found signs of temporomandibular dysfunction such as «click» noises when opening and closing.
Several signs and symptoms have been used to define the circumstances of temporomandibular articulation in children, nevertheless, it has yet not been clearly established whether these signs have normal variations of special characteristics.
Previous studies report low prevalence of temporomandibular dysfunction in children, when compared to adult patients. Nevertheless, prevalence of these signs and symptoms increase with age. The aforementioned notwithstanding, those studies were not able to establish whether, in children, measurements of mandibular movements could be used as a diagnostic factor of temporomandibular dysfunction. This could be due to the fact that, when undertaking studies of mandibular movements in children afflicted with temporomandibular dysfunction, mandibular movement ranges obtained were the same as those of children not afflicted with dysfunction.5,16,18,19
We suggest a similar study should be conducted in 7 year old children, since, taking into consideration theories exposed by Drs. Baqaien and Bonjardim, it is quite probable that range of mandibular movements might change due to the increase of articular eminence angulation as well as of articular fossa depth.9,16
Lack of reports and discrepancies found in studies conducted on mandibular movements in children could be attributed to changes the children experience during growth. These changes do not allow for a simple way of obtaining a reference table, contrary to the situation present when dealing with adult patients.
Due to ethnicity, weight and stature differences, mandibular movements found in six year old Mexican child population differed from similar studies conducted on same age children in other regions. In the present study only six year old children were assessed, which differed from other mentioned studies, where assessed children were grouped according to age. We would consider significant to continue the present study with the same group of children in order to observe changes that might occur during their growth and development stages.
REFERENCES
1. Cortese SG, Oliver LM. Determination of range of mandibular movements in children without temporomandibular disorders. Journal of Craniomandibular Practice. 2007; 25: 200-205. [ Links ]
2. Sousa LM. Evaluation of mandibular range of motion in Brazilian children and its correlation age, height, weight, and gender. Braz Oral Res. 2008; 22 (1): 61-66. [ Links ]
3. Nishijima N, Hayasaki H. Difference in tracks between habitual open and close mandibular movements at the condyle in children. J Oral Rehabil. 2000; 27: 999-1003. [ Links ]
4. Ingervall B. Range of movement of mandible in children. Scand J Dent Res. 1970; 78: 311-322. [ Links ]
5. Ingervall B. Variation of the range of movement of the mandible in relation to facial morphology in children. Scand J Dent Res. 1970; 78: 533-543. [ Links ]
6. Rothenberg LH. An analysis of maxium mandibular movements, craniofacial relationships and temporomandibular joint awareness in children. Angle Orthodontist. 1991; 61(2): 103-112. [ Links ]
7. de Vis H, De Boever JA. Epidemiologic survey of functional conditions of the masticatory system in Belgian children aged 3-6 years. Community Dent Oral Epidemiol. 1984; 12: 203-207. [ Links ]
8. Sönmez H, Sari S. Prevalence of temporomandibular dysfunction in Turkish children with mixed and permant dentition. J Oral Rehab. 2001; 28: 280-285. [ Links ]
9. Baqaien MA. Changes in condylar path inclination during maximum protrusion between the ages of 6 and 12 years. J Oral Rehabil. 2007; 34: 27-33. [ Links ]
10. Saitoh I, Tokutomi J. Correlations between incisor and condylar movements during lateral excursion in children with primary dentition. J Oral Rehabil. 2007; 34: 800-806. [ Links ]
11. González YM. Criterios diagnósticos para la investigación de los trastornos temporomandibulares CDI/TTM. Journal of Cranio-mandibular Disorders. 1992; [ Links ]
12. Zar JH. Biostatistical analysis. 5a. Ed. Prentice-Hall. New Jersey, USA. 2010, pp. 944-948. [ Links ]
13. Wackerly DD, Mendenhall W, Scheaffer RL. Estadística matemática con aplicaciones. 7a. Ed. Cengage Learning. México, D.F. 2010, p. 909. [ Links ]
14. SPSS. SPSS Inc. (Windows) versión 15. Chicago, USA. 2006. [ Links ]
15. Statpoint, Inc. STATGRAPHICS Centurion XV version 15.2.06. 2007 www.statgraphics.com [ Links ]
16. Bonjardim L, Duarte M. Mandibular movements in children with and without signs and symptoms old temporomandibular disorders. J Appl Oral Sci. 2004; 12 (1): 39-44. [ Links ]
17. Mutahroğullari M, Demirel F. Temporomandibular disorders in Turkish children with mixed and primary dentition: prevalence of signs and symptoms. Thurk J Pediatr. 2004; 46: 159-163. [ Links ]
18. Egermark I, Carlsson GE. A 20-year longitudinal study of subjective symptoms of temporomandibular disorders from childhood to adulthood. Acta Odontol Scan. 2001; 59: 40- [ Links ]
19. Clinical Affairs Committee. Temporomandibular joint problema in children subcommitte. Guideline on acquired temporomandibular disorders in infants, children adolescents; Reference manual 2010; 6: 258-261. [ Links ]
Note This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam Mailing address:
Mailing address:
María Leonor Alonzo Echeverría
E-mail: aechever@uady.mx

