










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista odontológica mexicana
Print version ISSN 1870-199X
Rev. Odont. Mex vol.19 n.1 Ciudad de México Jan./Mar. 2015
Original research
Assessment of two techniques for the recording of mandibular central relationship: gothic arch versus power centric relation
Juan Antonio Maldonado Moreno,* Luis Lombard Romero,§ Claudia Gutiérrez Camacho,II Joaquín Federico Canseco Jiménez,¶ Vicente Cuairán Ruidíaz**
* Graduate, Orthodontic Specialty.
§ Oral Rehabilitation Specialist, guest professor.
II Head of the Pre- and Graduate Department.
¶ Professor of the Orthodontics Specialty Course.
** Head of the Pediatric Department.
«Dr. Federico Gomez» Children's Hospital, Mexico.
ABSTRACT
The search for the true mandibular position with respect to the glenoid fossa and the relationship of the other components which constitute the temporomandibular joint known as centric relation (CR) are essential factors for its diagnosis, treatment and stability. The aim of the present study was to assess two techniques used for recording CR: power centric technique and gothic arch technique, with the purpose of determining the most effective method to confer greater accuracy to the recording. This was triggered by the fact that in our institution some inconsistencies had been detected when taking records of patients afflicted with considerable skeletal discrepancies or malformations. Fifteen healthy skeletal class II patients were assessed. Patients' ages ranged from 13 to 17 years. Eight patients were female (53.4%) and seven male (46.6%). Using both techniques, thirty mountings were performed in a semi-adjustable articulator, condylar changes were monitored using axial condylar position indicator (API). Results revealed no significant differences, nevertheless, observed transversal, vertical and saggital changes were greater with the gothic arch technique.
Key words: Centric relation, gothic arch, centric power relation.
INTRODUCTION
All along the years the concept of occlusion, condylar position and its relationship with orthodontics has been subject of controversy. Even though common objectives of orthodontic treatment include tooth alignment and stability, periodontal health, facial and dental esthetics, as well as functional occlusion, the inter-relation among these factors and condylar position has not yet been fully understood.1
A stable, replicable mandibular position, to be used as reference, is the base from which a successful orthodontic diagnosis can be established. This position is known as Centric Relation (CR). Due to the fact that it is the only replicable maxillarymandibular relationship, it has acquired acceptance as a referential position.2
DEFINITION OF CENTRIC RELATION, CENTRIC OCCLUSION AND MAXIMUM INTERCUSPATION
Dental sciences have not been able to reach an agreement with respect to the definition of centric relation. In 2004, Christensen3 mentioned that himself, as well as most dental professionals, «accept the concept of centric relation as the most comfortable posterior position of the mandible when it is bilaterally and gently manipulated in upward and forward movements towards a retrusive position». Nevertheless, for already 20 years, centric relation has been recognized as a condylar retrusive and posterior position.4
According to the glossary of prosthodontic terms centric relation (CR) is defined as «a maxillary-mandibular relationship where condyles are articulated to the thinnest and most avascular portions of their respective articular disks, with the assemblage at is most anterior and superior position against the walls of the articular eminence. This position is independent from dental contact. It is clinically established when the mandible is directed in a upper and forward direction through the transversal horizontal axis. This position is independent from what is clinically understood as dental contact, when the mandible is directed in upper and anterior direction through the transversal horizontal axis.»
Maximum intercuspation (MIC) is defined as «the complete intercuspation of the teeth independently from condylar position». Whereas centric occlusion (CO) is defined as «the occlusion of teeth when the mandible is placed in centric relation». This might or might not coincide with maximum intercuspation.5
HISTORY OF CENTRIC RELATION RECORDINGS
Phillip Ptaff6 was the first to describe his technique for bite recording, he called it «taking bite». From the end of the 19th century onwards this was the most commonly used method, nevertheless, several clinical operators have developed other techniques to record centric relation. In 1955 Shanahart7 described a technique he called «swallowing or free closure». This technique was based upon the fact that swallowing saliva was the determining factor to obtain vertical dimension and centric relation. Other researchers used the technique described by McCollum,8 called «chin point guidance». When this technique is followed, the mandible is retruded so as to emphasize the importance of the axial axis in centric relation recordings. Dawson9 recommended the «bilateral manipulation» technique. This technique stressed the importance of guiding the lower jaw in an upper direction, placing the operator's fingers into the goniac angles while thumbs applied pressure to the chin in order to facilitate condylar positioning in centric relation. Another technique, known as «Myo-monitor technique» is based upon muscular contractions stimulated to record centric relation.10
Lucia11 in 1964, suggested the use of an anterior jig, which was designed to minimally separate upper and lower teeth and thus break the proprioceptive pattern resulting from dental contact, thereby allowing the muscles to seat the condyle. Lundeen12 and Wood13 informed that a strong muscular contraction performed by a patient with a rigid anterior stop settles the condyle into a more superior position when compared to other techniques. With this same purpose in mind, Williamson14 supported the use of gauged sheets, that is to say, to settle the condyle in an anterior and superior position by the action of the upper bundle of the external pterygoid muscle and the temporal muscle without any influence of dental contact.15 Roth implemented a technique called power centric; in this technique two segments of Delar® (Delar Co, Lake Oswego) blue wax were used to record the bite. This technique allowed the patient's muscles to seat the condyles without influence of dental contact. The first graphic record was based upon mandibuar movement studies conducted by Balkwill in 1866.16 Arch intersection produced by left and right condyles forms an apex known as gothic arch tracing.17
The first «trace vertex» was reported by Hesse in 1897, this technique was established and made popular by Gysi around 191018 Gysi used an extraoral type of tracer. The plate where the tracing was to be undertaken was coated with wax and secured to the mandibular arch. This device included a rod or marker which was mounted on the maxillary arch. When an accurate recording was taken, the patient kept the plates centered on the apex of the tracing, these plates were upheld by a niche and were thus recorded and fixed. In 1927, Hanau19 established the fact that Gysi tracings were an effective method to perform recordings. On the other hand, Trench20 established that Gysi tracings should be the sole method to perform centric relation recordings, and that all other methods were «deceit and games». Gysi concluded that his tracing technique allowed for only a five degree error, whereas bite recordings made with wax exhibited error of up to 25 degrees.21
IMPORTANCE OF CENTRIC RELATION RECORDING AND CONDYLAR POSITION INDICATOR
At the beginning of the 70's, Roth, supporting the gnathological approach of occlusion and condylar position, encouraged orthodontists to perform mountings on articulated models when establishing their diagnoses. Roth considered that mounting models in centric relation would be extremely helpful to the orthodontist to identify the presence of dual bite as well minutiae of occlusal and condylar disharmonies.15,22
Criteria must be established for the adequate operation of the occlusion. Required occlusal scheme to meet these criteria must be carefully defined. An aspect that must be constantly present in our minds is the fact that we cannot simply believe all we see in the mouth. What we see within the mouth is the neuromuscular adaptation to closure as well as movements for existent occlusal disposition. Patients will bite where teeth are comfortable. Patients will move the mandible so as to avoid harmful tooth contact, averting possible collisions. Muscles will contract to evade self-inflicted damage to articulations, teeth and supporting structures. All these neuromuscular responses to the patient's existing occlusion limit our capacity to observe what we need to see in order to establish a functional occlusion.
Therefore, we need the help of instruments to remove all neuromuscular mechanisms of the patient and to see how would the patient open and move if there were no dental interference with the movement pattern allowed by his TMJ. We must also be able to study the tridimensional effect of mandibular and closing movement, as well as how the occlusion relates to movements dictated by the joint and closure patterns, if we wish to know how and why we will alter the position of the teeth.23
In order to record CR and border movements, articulators have been designed with the aim of replicating anatomical positions of the maxilla and mandible in order to achieve extra-oral analysis. The Condylar Position Indicator (CPI) and the Condylar axial position indicator (API) of the Panadent Company, were designed to record condylar movements. CPI or API assess, through occlusion, positional changes of the condyle: this is achieved with models mounted on the articulator in CR. These models are later transferred to CPI or API and when relating them to the maximum intercuspation record (MIC) transversal, vertical and anterior-posterior measurements can be achieved. Thus, through CPI, anterior-posterior distractions of the condyle from CR to MIC can be identified.24
In orthodontics, occlusion aspects addressed to diagnosis and treatment are of the utmost importance. Derakhshan and Sadowsky25 published the clinical case of a 41 year old female patient. In this case initial diagnosis was a slight class II division 1 malocclusion. This patient, after several months of treatment, exhibited an increase of horizontal overbite, anterior open bite, increase of the height of the lower third and muscle hypertonia, associated to a change in mandibular position generated by neuromuscular de-programming fostered by tooth movement. In this case, treatment plan had to be re-devised and the patient finally underwent surgery so as to achieve functional objectives. Authors regretted not having conducted an articular mounting before the treatment, since this would have helped them to unmask the real skeletal problem of that patient.
CONDYLAR POSITION IN PATIENTS WITH CLASS II BONE RELATIONSHIP
Ricketts26 showed that before orthodontic treatment, condyles which were in class II division 1 malocclusion were in a relatively forward position in the fossa, since in these patients, this was a way to try to maintain an appropriate airway. With treatment, condyles were moved backwards, to their normal position. With the help of laminographies, the following was found: both condyles as well as the mandibular closure pattern showed significantly greater distal movement from rest position to centric occlusion in cases of class II division 1 when compared to class II division 2 cases.27
The aim of the present study was to assess two techniques for mandibular centric relation recordings in bone class II patients, as well as determining the most efficient method to undertake model mounting based upon measurements obtained of CR and MIC discrepancies, and the experience achieved with manipulation of recording materials.
MATERIALS AND METHODS
The present study was assessed and approved by the Department of Teaching and Academic Development of the «Dr. Federico Gomez» Children's Hospital, Mexico. Informed consent was obtained according to requirements stated by this hospital. All the following were included: healthy patients (1), adolescents referred by the orthodontic outpatient service (2), patients exhibiting bone class II according to ANB angle (point A-nasion-point B) (3), patients without fixed appliances (4). The following were excluded: patients with facial and/or skeletal asymmetries (a), patients in early mixed dentition stages (b), patients with anterior maxillary compression greater than 5 mm (c), patients with sequels of cleft lip and palate (d), patients with dental agenesis in the posterior or anterior sector which would interfere with the recording (e) and patients with ATM signs and/ or symptoms (f). All patients who discontinued the study were discarded as well as those patients who had been subjected to restorative treatment during the time of record taking.
All procedures were undertaken by a single operator, previously gauged to decrease error degree. During procedure the following items were used: an articulator, facial bow, mounting stem bite tabs®, mounting table and condylar axial position indicator (API) (Panadent® system).
Three sets of alginate impressions were taken of each patient. They were immediately disinfected with sodium Hypochlorite and then rinsed. They were carefully cast with type IV plaster (Silky Rock, WhipMix Corp). Surplus and bubbles present in the models were removed in order to eliminate interferences.
UPPER MODEL MOUNTING
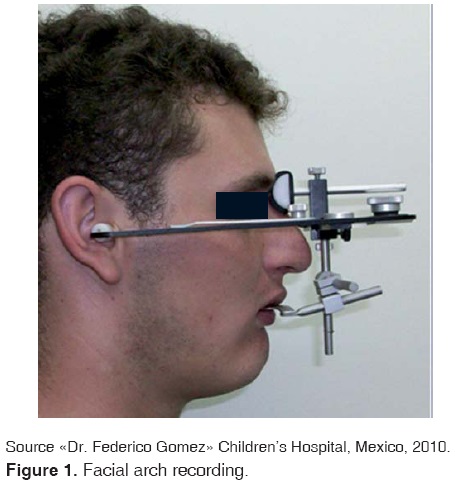
A split cast technique was used for the upper model by placing a plaster-plaster separator between surfaces at the moment they were joined. This was performed with the aim of rectifying the proper mounting of the lower model with the power centric technique. In order to successfully mount the upper model, information obtained in the facial arch recording of each patient was transferred to the articulator (Figure 1).
RECORDING AT MIC
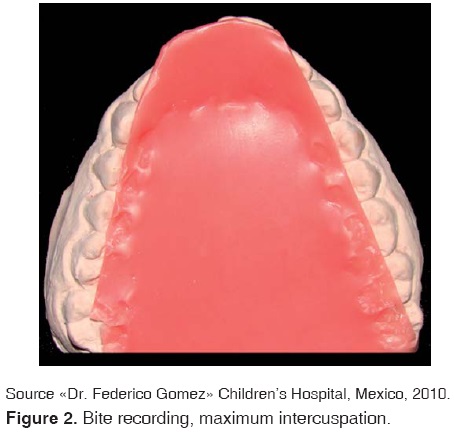
Maximum intercuspation recording was performed with extra-hard Moyco® pink wax. A wax sheet was heated to 53o so as to be able to bend it and thus obtain a sheet with two wax thicknesses. After this, it was pre-adjusted in the models in order to obtain a recording of greater precision and comfort for the patient. Wax was once again heated and was carefully inserted in the patient's mouth; the patient was requested to occlude with force into his habitual closing position, until feeling that antagonist occlusal aspects were in contact. Posterior and lateral excess material was trimmed before wax hardening. The wax sheet was once again placed into the mouth and care was taken to ascertain that closure was the same, either with wax, or without it (Figure 2). Once the recording of maximum intercuspation for record taking of both techniques was obtained, a roll of cotton was placed between patient's incisors for five minutes before initiating the procedure.
Recording at CR; centric power technique
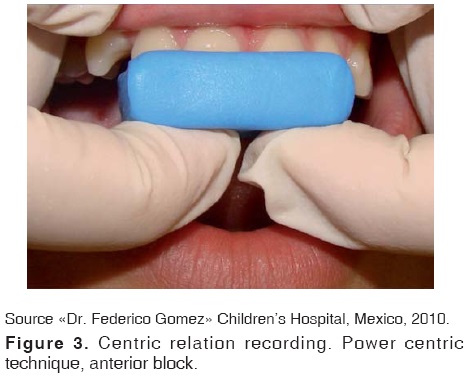
In order to record bite patterns, two segments of blue Delar® wax were used for each patient. The anterior block was built with a three-sheet thickness; this block spanned from the distal aspect of the right upper lateral incisor up to the distal aspect of the opposing side. Palatal extension varied according to the patient's overjet. The posterior segment was built with two wax thicknesses; this segment spanned from the right second premolar and first molar to the contra-lateral teeth. Following this, the patient was placed in a recumbent position at 45o with respect to the floor.
Wax was heated at 53 oC and was then taken to the patient's mouth. Once the wax's anterior segment was placed, the operator guided the mandible to centric relation, seating the condyles in an upwards direction and guiding the progonion downwards. Immediately after this, the patient was instructed to close the mandible until posterior teeth reached a 2 mm disocclusion. The anterior block was cooled with compressed air before being removed; once removed, the block was immersed in water and ice in order to avoid deformation (Figure 3).
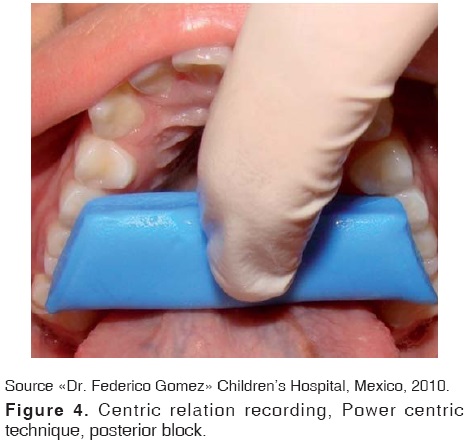
After this, the posterior segment was heated to a 53 oC temperature, to be then placed on the upper teeth. Once the posterior segment was in position, the anterior block was once again placed on the upper arch. The patient was once again guided to mandibular closure until feeling contact of lower incisors within the anterior block. Materials were once more cooled before and after inserting them in the mouth (Figure 4). Once the recording was achieved, wax sections were adjusted with the aim of freeing interferences. The lower model was then mounted using the split-cast method to rectify the procedure.
Recording at CR: gothic arch tracing technique
In order to record centric relation with the gothic arch technique. Dentsply® commercial recording sheets were used. These sheets were individually adapted to each patient; this was achieved with the use of a set of plaster models mounted on a hinged articulator set at maximum intercuspation and with Nictone® clear self-curing acrylic to achieve individualization (Figure 5). Before placing the lower plate into the patient's mouth it was tinted with a black indelible marker, bearing in mind that mandibular movements were traced on this surface.

The patient was placed in a 90o position with respect to the floor, and the upper plate with the marker rod was placed. After this, the lower plate was introduced in the lower arch. The patient was then instructed to occlude until the upper rod would contact the lower plate. The patient was then instructed to perform protrusion and laterality movements for two minutes, without separating the plates. Lacks of contact and interferences were carefully monitored during the record taking, so as to guarantee that contact would only take place between the rod and the lower plate (Figure 6).

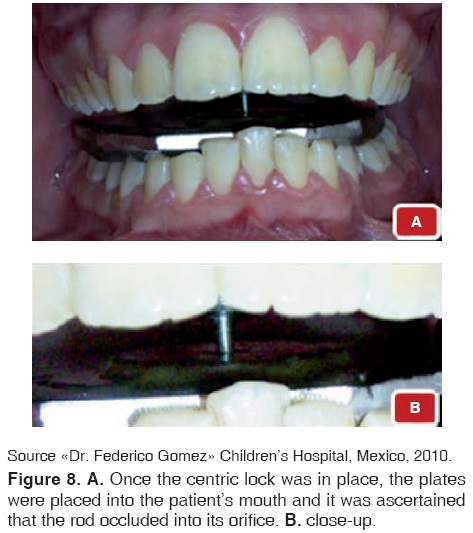
Once the tracing was obtained, the lower plate was removed and the centric lock was placed. This centric lock is an acrylic appliance containing one perforation, which was placed and secured with wax exactly at the vertex of the gothic arch tracing, this is better known as centric relation (Figure 7).

Once the position was verified, the lower plate was once more introduced in the patient's mouth intending that the rod would fall into the centric relation lock orifice (Figure 8). In this position snow-white type plaster was laterally injected; this was performed with the aim of obtaining mounting guides for the lower model. After four minutes, when the plaster had set, plates and gothic arch tracing guides were removed in order to perform adjustments.
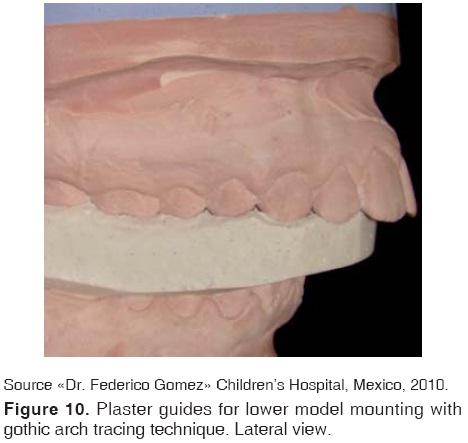
Mounting of the lower model was achieved with the use of plates along with obtained plaster guides. This enabled achievement of greater precision at the moment of conducting the procedure (Figures 9 and 10).
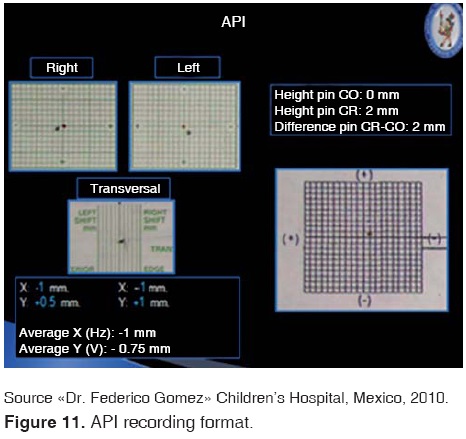
Once the recordings were completed and the mountings were achieved, measurements of detected occlusal findings were undertaken. With the help of a millimeter digital gauge and a condylar axial position indicator (API), condylar level saggital, vertical and transversal distractions could be measured (Figure 11).
Obtained measurements were compared and rectified in order to decrease error possibilities. Afterwards, they were concentrated into the database to be later statistically analyzed.
STATISTICAL ANALYSIS
Comparison of proportions was undertaken with Fisher exact test of qualitative variables, as well as median test for their comparison, p < 00.05 was considered statistical significance.
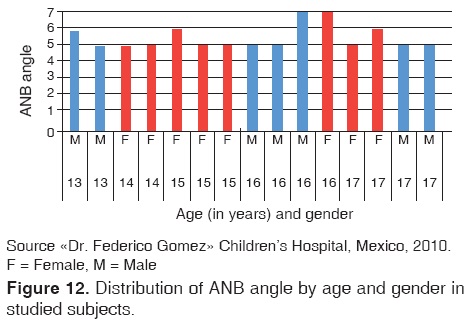
Figure 12 shows distribution according to gender and age of ANB angle (formed by the planes Nasionpoint A and Nasion-point B).
RESULTS
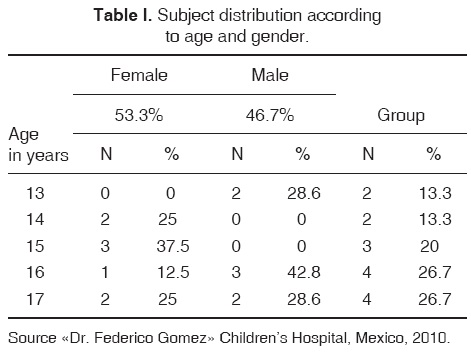
A total of 30 mountings were performed in 15 bone class II patients, eight were female (53.3%) and seven male (46.7%), mean age was 16 ± 1.4 years table I shows distribution according to age and gender.
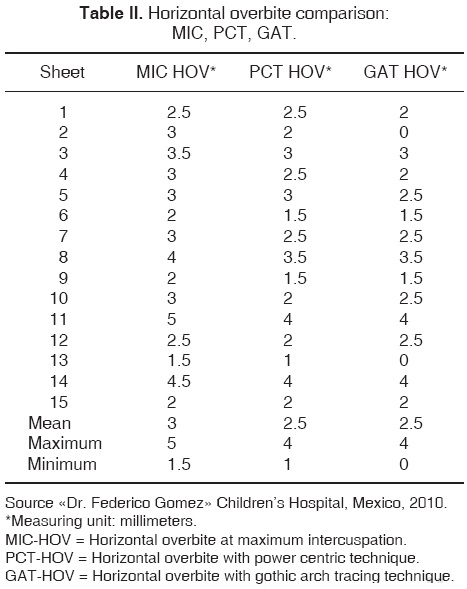
With respect to horizontal overbite at MIC (maximum intercuspation) the following was obtained: mean of 4 mm, maximum 7 mm and minimum 2 mm. With the power centric technique (PCT) a 5 mm mean was achieved, maximum 7.5 and minimum 2.5. With the gothic arch tracing technique (GAT) mean was 5 mm, maximum 9 mm and minimum 2.5 mm, as depicted in table II.
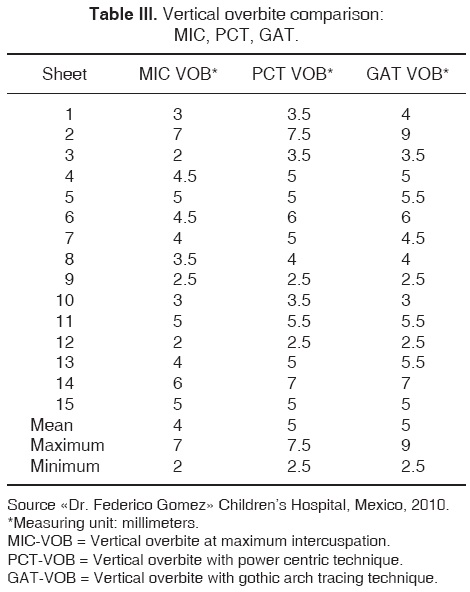
Vertical overbite at maximum intercuspation (MIC) showed a 3 mm mean, maximum 5 mm and minimum 1.5 mm. PCT recorded 2.5 mean maximum 4 mm, minimum 1 mm. GAT achieved 2.5 mm mean, maximum 4 mm and minimum 0 mm as depicted in table III.
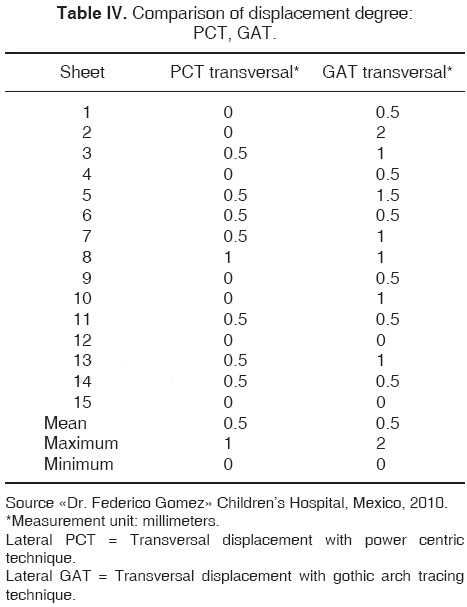
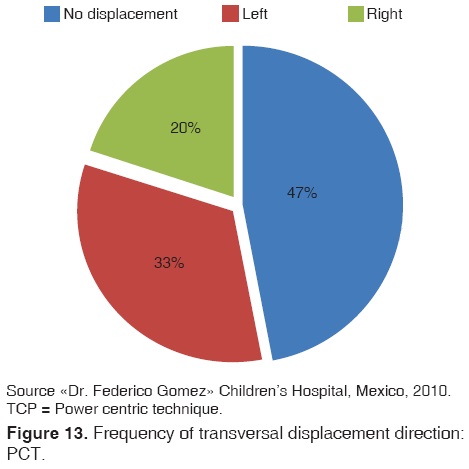
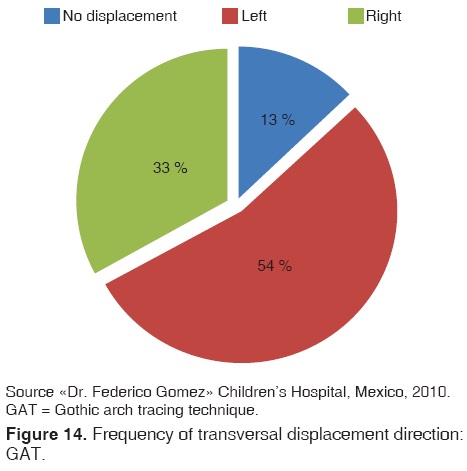
When studying transversal displacement, gothic arch technique showed greater movement, with 0.5 mm mean, 2 mm maximum and 0 mm minimum (Table IV). Figures 13 and 14 show frequency of this displacement.
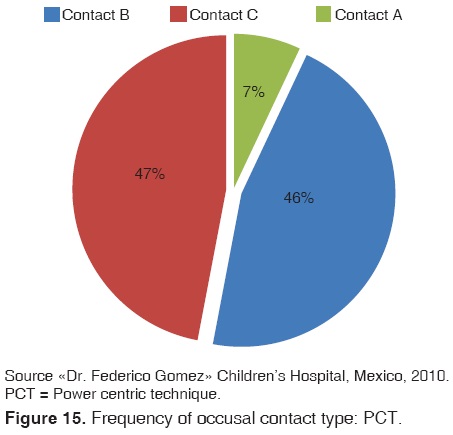
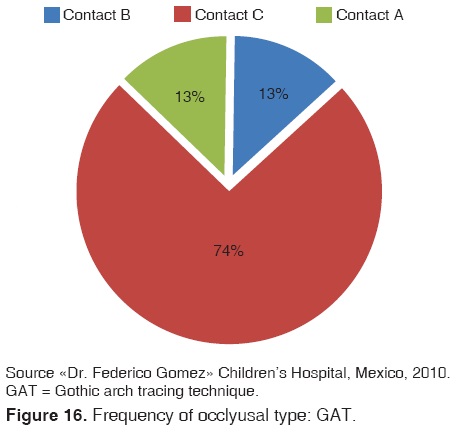
With respect to occlusal contact type frequency, it was observed that PCT and GAT exhibited greater frequency of type B contacts (Figures 15 and 16).
With respect to results obtained with the condylar axial position indicator (API), a condylar distal displacement trend was observed at plane X (horizontal). For PCT mean was -1 mm with -0.5 mm maximum and -2.75 minimum. For GAT, mean was -1.25 mm with -0.5 mm maximum and -3.25 mm minimum. In plane Z (vertical), displacement trend was lower, PCT reported a mean of 1 mm, maximum 2.25 mm and minimum 0f 0.25 mm. GAT showed mean of 1 mm, 2.75 mm maximum and 0.5 mm minimum.
With respect to vertical API, with PCT, a 0.5 mm mean was obtained , with maximum 1 mm, minimum 0 mm, with GAT, 0.5 mm mean was obtained, with 3 mm maximum and 0 mm minimum.
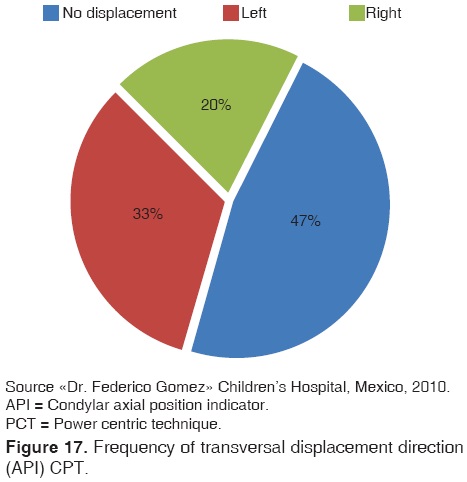
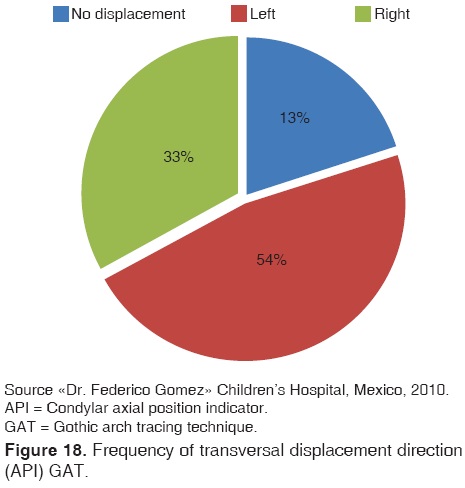
With respect to transversal API, with PCT a 0.5 mm mean was reported with 1.5 mm maximum and 0 mm minimum; with GAT a 1 mm mean was reported with 2.5 mm maximum and 0 mmminimum (Table V). Figures 17 and 18 show frequency of direction of this displacement.
DISCUSSION
The topic of centric relation recordings and true mandibular position is a very controversial subject. Nevertheless, in our search for excellence and distinction as professionals, we must target achieving improved recordings in order to establish a treatment plan which will yield better results. Mastery of a technique suitable to record centric relation depends on many factors: experience of the operator, material quality and manipulation ease, patient's cooperation and neuromuscular circumstances, as well as operator's skill to face situations where recording taking can represent a great challenge.
According to Schmitt,2 when he conducted research on reproducibility of power centric technique, he concluded that it was a highly reproducible method to record CR, nevertheless he mentioned there were slight inconsistencies during his study, which were probably due to an error during bite recording or during instrumentation with the condylar position indicator.
Orthodontists with gnathological orientation believe that the tolerance which must exist between MIC and centric relation must be 1.5 mm in horizontal and vertical planes, and 0.5 mm in transversal plane.24 Utt28 reported 2.0 mm in horizontal and vertical planes and 0.5 mm in transversal plane. Crawford29 suggested a discrepancy of 12 mm in horizontal-vertical planes, and a transversal discrepancy of 0.5 mm. Other professionals who did not share this vision stated there was a 2-4 mm tolerance in the horizontal plane and none or nil relevance in vertical and transversal dimension.30,31
Results obtained in the present study were the following: horizontal overbite mean was 4 mm for MIC, 5 mm for PCT and GAT, therefore, discrepancies between MIC and CR were 1 mm. Vertical overbite acquired a 3 mm mean in MIC, 2.5 mm for PCT and 2.5 for GAT; this represented a 0.5 mm discrepancy between MIC and CR. In transversal direction, mean with respect to condylar distraction degree was 0.5 mm in both techniques.
Klar1 who conducted a study on 200 patients treated with Roth philosophy and straight arch appliances, reported that pre-treatment mean discrepancy between MIC and CR was 0.81 in vertical direction and 0.44 mm in transversal direction. He conducted other tests to examine whether there were other correlations among groups and the amount of condylar distractions such as bone class, facial biotype etc. Nevertheless, he did not find significant differences.
With respect to condylar distraction recorded in API, we found a horizontal direction (x) horizontal discrepancy of -0.25 mm between GAT and PCT, a 0 mm (z), vertical with respect to the articular rod of0mmaswell astransversal of 0 mm. Although differences found between both techniques are not significant they exhibited with GAT recordings greater degrees of distraction.
CONCLUSIONS
Gothic arch tracing technique is a reliable method. This could be due to the fact that materials used to achieve CR mounting were not thermoplastic and did not require patient manipulation performed by the operator to lead the mandible to centric relation. It equally offers a certain degree of dis-occlusion while taking recordings, this helps neuromuscular de-programming and with it, a more reliable and reproducible recording. Although more laboratory time is needed for its construction, less patient time is required in the dental chair.
REFERENCES
1. Klar NA, Kulsbersh R, Freeland T, Kaczynski R. Maximum intercuspation - centric relation disharmony in 200 consecutively finished cases in a gnathologically oriented practice. USA Semin Orthod. 2003; 9: 109-116. [ Links ]
2. Schmitt, Freeland T, Bever K, Pink FE. Reproducibility of the roth power centric in determining centric relation. USA Semin Orthod. 2003; 9: 102-108. [ Links ]
3. Christensen GJ. Is occlusion becoming more confusing? A plea for simplicity. JADA. 2004; 135: 767-770. [ Links ]
4. Rinchuse DJ, Kandasamy S. Centric relation a historical and contemporary orthodontic perspective. JADA. 2006; 137: 494-501. [ Links ]
5. The glossary of prosthodontic terms. J Prosthet Dent. 2005; 94 (1): 10-92. [ Links ]
6. Swenson MG. Complete dentures. Ed. 6. St. Louis, 1970 The C.V. Mosby Co. [ Links ]
7. Shanahan TE. Physiologic jaw relation and occlusion of complete dentures. J Prosthet Dent. 1955; 5: 319-324. [ Links ]
8. McCollum BB. Function--factors that make mouth and teeth a vital organ. Am Dent Assoc. 1927; 14: 1261-1271, CB Mosby, 1989. [ Links ]
9. Dawson PE. Evaluation, diagnosis, and treatment of occlusal problems. St Louis, MO. [ Links ]
10. Granger ER. Centric relation. J Prosthet Dent. 1952; 2: 160-171. [ Links ]
11. Lucia VO. A technique for recording centric relation. J Prosthet Dent. 1964; 14: 492-505. [ Links ]
12. Ludeen HC. Centric relation records: The effect of muscle action. J Prosthet Dent. 1974; 31: 244-253. [ Links ]
13. Wood DP, Floreani KJ, Galil KA, Teteruck WR. The effect of incisal bite force on condylar seating. Angle Orthod. 1994; 64: 321-330. [ Links ]
14. Williamson E. Occlusal concepts in orthodontic diagnosis and treatment. In: Johnson LE (ed). New vistas in orthodontics. Philadelphia, PA, 1985; 192-147. [ Links ]
15. Roth RH. Functional occlusion for the orthodontist, Part I. J Clin Orthod. 1981; 15 (1): 32-51. [ Links ]
16. Balkwill FH. The best form and arrangement of artificial teeth for mastication. Br J Dent Sci. 9:278, 1886. [ Links ]
17. Sears VH. Centric jaw relation. Dent Dig. 1952; 58: 302. [ Links ]
18. Gysi A. The problem of articulation. Dent Cosmos. 1910; 52: 1. [ Links ]
19. Hanau RL. Dental engineering. Vol. I. part II. Buffalo, 1927, Hanau Engineering Co. [ Links ]
20. Tench RW. Interpretation and registration of mandibulomaxillary relations and their reproduction in an instrument. J Am Dent Assoc. 1926; 13: 1675. [ Links ]
21. Gysi A. Practical application of research results in denture construction. J Am Dent Assoc. 1927; 14: 409. [ Links ]
22. Roth RH. Functional occlusion for the orthodontist, Part II. J Clin Orthod. 1981; 15 (2): 100-123. [ Links ]
23. Roth RH. Functional occlusion for the orthodontist, Part III. J Clin Orthod. 1981; 15 (03): 174-198. [ Links ]
24. Lavine D, Kulbersh R, Bonner P, Pink FE. Reproducibility of the condylar position indicator. Semin Orthod. 2003; 9: 96-101. [ Links ]
25. Derakhshan M, Sadowsky C. A relatively minor adult case becomes significantly complex: a lesson in humility. Am J Orthod Dentofacial Orthop. 2001; 119: 546-553. [ Links ]
26. Ricketts RM. A study of change in temporomandibular relations associated with the treatment of Class II malocclusion. Am J Orthod. 1952; 38: 918-933. [ Links ]
27. Bishara SE. Class II malocclusions: diagnostic and clinical considerations with and without treatment. Semin Orthod. 2006; 12:11-24. [ Links ]
28. Utt TW, Meyers CE Jr, Wierzba TF, Hondrum SO. A three-dimensional comparison of condylar position changes between centric relation and centric occlusion using the mandibular position indicator. Am J Orthod Dentofacial Orthop. 1995; 107: 298-308. [ Links ]
29. Crawford SD. Condylar axis position, as determined by the occlusion and measured by the CPI instrument, and signs and symptoms of temporomandibular dysfunction. Angle Orthod. 1999; 69 (2): 103-115. [ Links ]
30. Rinchuse DJ. Counterpoint: a three-dimensional comparison of condylar change between centric relation and centric occlusion using the mandibular position indicator. Am J Orthod Dentofacial Orthop. 1995; 107: 319-328. [ Links ]
31. McNamara JA Jr, Seligman DA, Okeson JP. Occlusion, orthodontic treatment, and temporomandibular disorders: a review. J Orofac Pain. 1995; 9 (1): 73-90. [ Links ]
Note This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam Mailing address:
Mailing address:
Juan Antonio Maldonado Moreno
E-mail: grupoolinka@hotmail.com

