











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
Asthma is a common cause of admission to the pediatric intensive care unit (PICU). In addition to pharmacological therapies, respiratory support by non-invasive mechanical ventilation (NIMV) has been the classical approach to help these patients. In recent years, this approach has been complemented and replaced by a high-flow nasal cannula (HFNC)1. Both respiratory supports are used to avoid mechanical ventilation (MV), which is helpful but associated with complications2.
The use of HFNC in children has increased. Certainly, its simplicity and comfort have influenced its implementation3,4. Thus, its use has been described in neonatal units5,6, emergency rooms7-9, hospital wards5,10,11, transport12, or intensive care units13-15. Additionally, HFNC has been defined as safe for managing bronchiolitis16,17 or asthma1,14,15,18.
However, using HFNC in these different clinical settings is not always supported by consistent clinical evidence8,19. In addition, there is concern that HFNC may delay the initiation of other ventilatory strategies with proven efficacy7. In asthma, for example, there are doubts about how HFNC might delay NIMV10,13. This potential risk should be addressed in children with severe asthma20.
Therefore, in this short prospective observational monocentric study, we described and analyzed the therapies applied to children admitted to a tertiary PICU due to asthma. Later, we evaluated the use of HFNC in these patients and compared their evolution and complications with those who received non-invasive ventilation.
Methods
Design
We conducted an observational, prospective, longitudinal study in a tertiary PICU (from October 2017 to October 2019). The study was approved by the hospital ethics committee. Data were collected from clinical records following the principles of the Declaration of Helsinki. The parents or caregivers of each patient were informed about the study and were included after obtaining their consent. In addition, patient data were anonymized after discharge.
Inclusion criteria
Patients who met the following criteria were included in the study:
− < 18 years of age.
− Patients with asthma, defined as an acute episode of increased work of breathing with wheezing and prolonged expiratory phase in a previously healthy child or with similar previous episodes.
− Patients admitted to the PICU due to failure to respond to optimized asthma therapies in the Pediatric Emergency Department/Pediatric Unit.
− No major comorbidities or pre-existing conditions other than asthma.
− No criteria for acute bronchiolitis. On physical examination, acute bronchiolitis was defined as the onset of wheezing before 24 months in patients with a viral lower respiratory tract infection and no other explanation for the wheezing.
Respiratory support
The respiratory support used was not standardized or randomized. Physicians decided which therapy to use based on their clinical judgment.
− NIMV: bi-level positive airway pressure (BiPAP) Vision V60® (Respironics Philips) with a full-face or oronasal mask. Modalities: continuous positive airway pressure (CPAP) and BiPAP. CPAP was initially set at 5-6 cm H2O. For BiPAP, inspiratory positive airway pressure was initially set at 8-10 cm H2O, and end-positive airway pressure was set at 5-6 cm H2O. Inspiratory and expiratory pressures were titrated in 2 cm H2O increments based on tidal volume, continuous pulse oximetry, work of breathing, respiratory rate, and subject-ventilator synchrony. The fraction of inspired oxygen (FiO2) was titrated to maintain SpO2 > 92%.
− High flow nasal cannula (HFNC): Fisher-Paykel High Flow Nasal Cannula® and Vapotherm® were used. A cannula of a suitable size, an appropriate circuit, a humidifier, and air or oxygen were used. Cannula size was selected based on the subjects weight, and flow rates were initiated at 0.5-1 L/kg/min. The FiO2 was titrated to maintain a SpO2 > 92%.
Data
− Demographic characteristics (age in months and sex).
− Clinical data: respiratory rate on admission, presence and characteristics of wheezing, pulmonary score, oxygen saturation (SatO2)/FiO2 ratio, venous blood gas values on admission (pH, partial pressure of carbon dioxide, HCO3), pharmacological treatment received (bronchodilators, corticosteroids, antibiotic therapy, magnesium sulfate), type and days of ventilatory support, length of stay in the PICU, and total hospital stay. The attending physician selected pharmacologic treatment based on his or her expertise and the clinical protocols of the PICU.
Statistical analysis
Data analysis was performed with the SPSS® statistical package (version 21.0; IBM Company®, New York, United States). The homogeneity of the demographic variables and other clinical parameters were analyzed at the beginning of the study (having a non-normal distribution) and compared between groups. Descriptions were made using the median and interquartile range, and for the qualitative variables, absolute frequency and relative frequency. The KruskalWallis test for quantitative variables and Fisher´s exact test for dichotomous variables were used to analyze the characteristics of the three treatment groups.
Results
Eighty-six children were initially recruited (Fig. 1). Finally, 76 patients were included in the study, of whom 39 were female; the median age of the study population was 25 months (4-160). The median length of hospital stay was 6 days (1-23). On admission to the PICU, the SaO2/FiO2 ratio was 195 (90-384), the pulmonary score was 5 (1-8), and the respiratory rate was 40 (20-68). Regarding the gasometer variables, we observed that children had a PCO2 of 36.15 (15.2-86), a HCO3- of 21.7 (13.5-40) with a pH of 7.37 (7.13-7.49) on admission to the PICU. Sixty-nine children received intravenous steroids prior to PICU admission. These data are described globally and based on each respiratory support received in table 1. There were no children in the MV group. None of the patients who received HFNC as initial therapy required NIMV. There were no deaths.
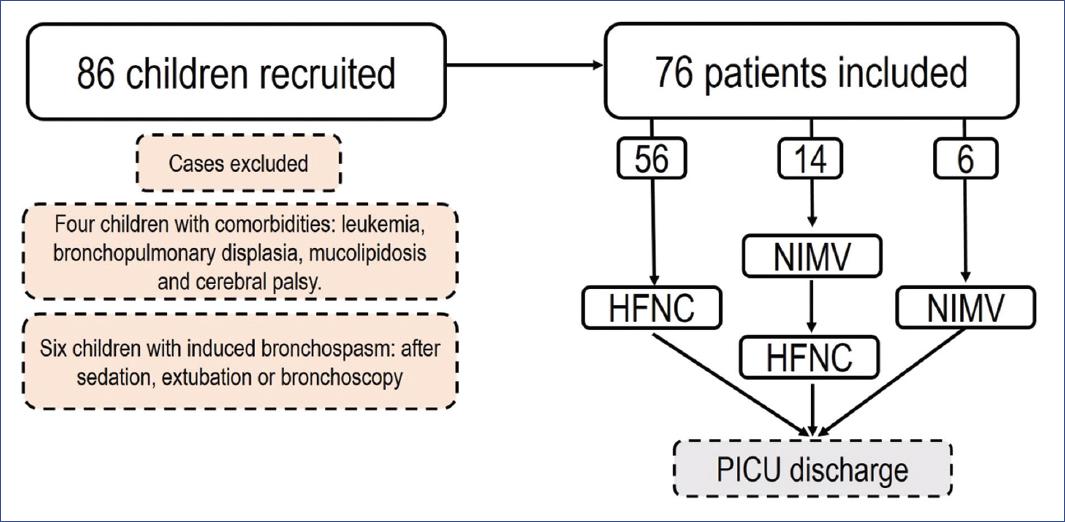
Figure 1 Flowchart of patient inclusion and exclusion. HFNC: high flow nasal cannula; NIMV: non-invasive mechanical ventilation; PICU: pediatric intensive care unit.
Table 1 Treatments of children admitted to a tertiary PICU due to asthma
| Variables analyzed | Total | Only HFNC (n = 56) | HFNC + NIMV (n = 14) | Only NIMV (n = 6) | p-value |
|---|---|---|---|---|---|
| Female | 39/76 (51%) | 26/56 (46%) | 9/14 (64%) | 4/6 (66%) | 0.6 |
| Age (months) | 25 (4-160) | 29 (4-143) | 12.5 (4-164) | 14 (5-26) | 0.1 |
| Hospital stay (days) | 6 (1-24) | 5 (2-24) | 11 (1-12) | 14 (3-22) | 0.09 |
| SatO2/FiO2 ratio | 195 (90-384) | 204 (97-384) | 185 (92-333) | 101 (90-271) | 0.02 |
| PCO2 | 36.15 (15.2-86) | 35 (15.7-67) | 43.5 (32.8-86) | 45.6 (28.1-51) | 0.032 |
| Pulmonary score | 5 (1-8) | 5 (1-7) | 5 (3-8) | 5 (2-7) | 0.53 |
| pH | 7.37 (7.13-7.49) | 7.37 (7.13-7.49) | 7.38 (7.15-7.47) | 7.41 (7.29-7.49) | 0.6 |
| HCO3 | 21.7 (13.5-40) | 20.7 (13.5-40) | 21.7 (17.9-32.4) | 24.6 (21.7-28.9) | 0.11 |
| Respiratory rate | 40 (20-68) | 39 (20-68) | 43 (24-68) | 52 (29-62) | 0.06 |
| Intravenous steroids | 69/76 (90%) | 50/56 (89%) | 14/14 (100%) | 5/6 (83%) | 0.38 |
HFNC: high flow nasal cannula; NIMV: non-invasive mechanical ventilation; SatO2/FiO2: oxygen saturation/fraction of inspired oxygen ratio; PCO2: partial pressure of carbon dioxide.
Comparisons based on respiratory support
In our series, 52/76 children underwent a chest X-ray. In addition, 33/76 received antibiotics, 13/76 received magnesium sulfate, and 19/76 received a continuous dose of albuterol. Table 2 shows the comparison between the respiratory groups. Children requiring only HFNC required less routine chest radiography, antibiotic therapy, continuous albuterol, and magnesium sulfate.
Table 2 Complementary tests according to each type of respiratory support
| Respiratory support | Chest X-ray | Empiric antibiotics | Magnesium sulphate | Continuous albuterol | ||||
|---|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | Yes | No | Yes | No | |
| Only HFNC | 34/56 (60%) | 21/56 (40%) | 21/56 (37%) | 35/56 (63%) | 7/56 (12%) | 49/56 (88%) | 10/56 (18%) | 46/56 (82%) |
| HFNC + NIMV | 14 (100%) | 0 | 9/14 (64%) | 5/14 (35%) | 6/14 (43%) | 8/14 (57%) | 9/14 (64%) | 5/14 (35%) |
| NIMV | 4/6 (66%) | 2/6 (33%) | 3/6 (50%) | 3/6 (50%) | 0 | 6 (100%) | 0 | 6 (100%) |
| Total | 52/76 (68%) | 24/76 (30%) | 33/76 (44%) | 43/76 (56%) | 13/76 (17%) | 63/76 (83%) | 19/76 (25%) | 57/76 (75%) |
| p-value | 0.007 | 0.001 | 0.02 | 0.001 | ||||
HFNC: high-flow nasal cannula; NIMV: non-invasive mechanical ventilation.
The median number of PICU days was lower in the only-HFNC group compared to other types of ventilatory support (Table 3, p = 0.025). Furthermore, SatO2/FiO2 was lower in the only-NIMV group and higher in the only-HFNC group (Table 3, p = 0.026). PCO2 was higher in the only-NIMV group (Table 3, p = 0.032).
Table 3 Progression and severity variables (median and range)
| Respiratory support | PICU days | SaO2/FiO2 ratio | pCO2 |
|---|---|---|---|
| HFNC | 3 (1-8) | 204 (97-384) | 35 (15.7-67) |
| HFNC + NIMV | 5 (1-9) | 185 (92-333) | 43.5 (32.8-86) |
| NIMV | 3.5 (1-10) | 101 (90-271) | 45.6 (28.1-51) |
| p-value | 0.025 | 0.026 | 0.032 |
HFNC: high flow nasal cannula; NIMV: non-invasive mechanical ventilation; SatO2/FiO2: oxygen saturation/fraction of inspired oxygen ratio; PICU: pediatric intensive care unit.
Discussion
In this study, we observed that HFNC was the most frequently used respiratory support in children admitted to the PICU for asthma. Furthermore, children requiring only HFNC had less pharmacological therapy and shorter PICU and hospital stays. The presence of low SatO2/FiO2 and elevated PCO2 on admission was associated with using NIMV.
HFNC delivers a warm and humidified airflow with a variable oxygen fraction (between 0.21 and 1) and a flow between 2 L and 60 L21. Theoretically, HFNC reduces oropharyngeal dead space, decreases CO2 rebreathing, improves mucociliary clearance22, and generates an airway positive pressure of up to 6 cm H2O. The interest in using HFNC as respiratory support stems from these properties and increased patient comfort17,23. In addition, it does not require breathing synchronization and requires less nursing care (compared to a NIMV device). This constant flow may also facilitate nasopharyngeal air renewal, which would improve CO2 washout and oxygenation11.
As mentioned above, asthma is one of the leading causes of PICU admission. In our series, we included a similar number of males and females, with a median age of almost 2 years. This age is younger than that described in other studies and may limit the external validity of our work14,15. Although we applied strict exclusion criteria, preschool children inclusion may have introduced a bias. We probably also included cases of bronchospasm, more representative of infectious bronchial hyperreactivity than asthma.
As it is known, the evidence on the utility of HFNC as an optimal respiratory support in severe asthma is scarce1,13,20. Ramnarayan et al. conducted a pilot study to evaluate it through a multicenter and randomized clinical trial. They found that switching from HFNC to NIMV was frequent15. Similarly, an observational study of 42 asthmatic children by Pilar et al. concluded that initial support with HFNC was not optimal and that NIMV support was delayed. As mentioned above, HFNC was the most frequently used respiratory support14. In addition, we did not observe any treatment failures or increased PICU or hospital admission days in those who received HFNC as first respiratory support. These findings are in contrast to what has been published previously and should be considered with caution15.
Given the design of our study, it is difficult to define objective data to understand and explain why the transition from HFNC to NIMV was unnecessary. We observed that patients receiving HFNC showed higher SatO2/FiO2 values and lower CO2 levels, probably indicating a better situation on admission to the PICU for these children20. Furthermore, the decision to initiate one type of ventilatory support over another was not randomized but left to the clinicians judgment. It appears that SatO2/FiO2 and CO2 levels significantly influenced the choice of NIMV as treatment. In addition, children receiving NIMV required more chest X-rays, empirical antibiotic therapy, magnesium sulfate, and continuous nebulized albuterol. Overall, these aspects would provide insight into the higher clinical severity in the NIMV group1.
Finally, as noted above, the use of HFNC remains controversial because it is still being determined whether it can prolong hospital stays and delay other types of assistance while being cost-effective for the healthcare system. In our series, there was no delay in other types of care. In addition, we observed that patients who received HFNC had a shorter PICU stay and a significantly shorter hospital stay. Although these observations cannot be considered a direct effect of HFNC use, they are of interest because they objectively demonstrate that, at least in our center, patients requiring HFNC for severe asthma are discharged promptly without excessive impact on resource utilization.
This study has several limitations. As mentioned above, physician expertise led to selecting children who could be treated with HFNC with a low risk of treatment failure. Therefore, our results may be difficult to generalize. In addition, we included children < 2 years of age. We tried to exclude cases of acute bronchiolitis, but we assume this cohort may not represent critical asthma patients. Finally, the different pharmacological treatments used were not evaluated; their indications and impact on clinical evolution and respiratory support effectiveness should be evaluated in future studies.
In conclusion, HFNC was a safe approach for children admitted to the PICU for asthma. Those patients who received HFNC as primary respiratory support did not require escalation to NIMV. The absence of blood gas changes on admission to the PICU and the absence of high oxygen requirements may help to select good responders to HFNC. However, external validation of our results is complex. Data from other centers are needed to verify our observations.

