











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkCriss cross is a complex and extremely rare congenital heart disease, defined as a disorder of the rotation of the cardiac loop1.
A 35-year-old female was referred to our hospital with history of 2 years of slowly progressive dyspnea, without other symptoms, she had an antecedent of acute stroke at the age of 15 without neurological sequelae. Diagnosis of congenital heart disease without morphological diagnosis was made pre-gestational and was indicated definitive contraception; however, she decided to get pregnant Consulted to our clinic with a 12-week pregnancy.
Echocardiography was performed showing dextroposition, visceral situs inversus, wide ostium primum atrial septal defect, ventricular septal defect, left ventricular hypoplasia, right ventricular hypertrophy and dilatation, and pulmonary hypoplasia/atresia (Figs. 1 and 2). Diagnosis of Criss cross was not made by this method. Cardiac resonance confirmed the findings described: Cyanotic congenital heart disease: Atrioventricular concordance in Criss cross perforated mode, the ventriculoarterial connections with double outlet of the right ventricle with vessels side by side, aorta in anterior position and the pulmonary artery is posterior (Figs. 3 and 4).

Figure 1 Cardiac magnetic resonance, axial four chambers view. Dextrocardia and crossed connections, atrioventricular concordance preserved. LV: left ventricle; RV: right ventricle; VSD: ventricular septum defect; RA: right atrium; LA: left atrium; ASD: auricular septum defect.

Figure 2 Transthoracic echocardiogram, long paraesternal axis view. Large ventricular septum defect, 37 mm.

Figure 3 Cardiac magnetic resonance, coronal axis view. Dextrocardia, crossed connections, RV above LV.
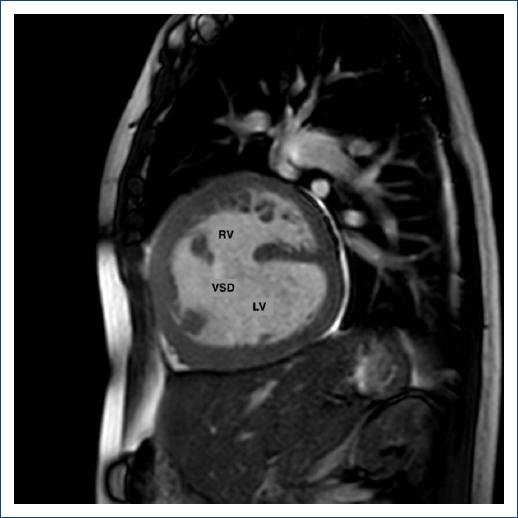
Figure 4 Cardiac magnetic resonance, short axis, sagittal view. The ventricles are related top to bottom.
The patient was managed with closely monitoring, diuretic treatment for heart failure, pulmonary vasodilator, and anticoagulation due to diagnosis of atrial tachycardia, also we performed continuous monitoring with BNP. At week 29, she presented clinical deterioration and a rise in BNP, for that reason, we decided termination of pregnancy, with subsequent decrease in BNP levels (< 100 pg./mL). The mother and newborn had favorably outcomes in postpartum period.
Only 100 cases have been reported in the literature to date. All of them had been described in association with other malformations, and about two-thirds of patients did not survive early childhood. Morbidity and mortality are mainly conditioned by the presence and magnitude of pulmonary stenosis. To the best of our knowledge, only two cases have been reported in pregnancy2. It is important to stratify maternal-fetal risk with scales such as WHOm, CARPREG or ZAHARA3, which should be re-evaluated during pregnancy, to define follow-up and management, as well as natriuretic peptide levels, since they are associated with the occurrence of cardiac events.

