











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkProfessor Dr. José Manuel Rivero Carvallo (Fig. 1) was an eminent Mexican cardiologist, born in the state of Puebla on April 1, 1905, and died on February 15, 19931. He dedicated his life to the study of tricuspid valve disease focusing on semiological aspects and giving important contribution to the knowledge of the pathology of tricuspid valve disease and the mechanical aspects of murmurs.
1928. He started studying at the meritorious Autonomous University of Puebla, Mexico, and he got a scholarship to the Sorbonne University in Paris.
1932. He obtained a Doctorate at the Sorbonne University with the thesis entitled “Blood pressure during anesthesia and certain surgeries” (La pression artèrielle au tours de l’anesthèsie et de certaines interventions chirurgicales, Paris, E. Le François, 1932).
1933. Internship at Hôpital de la Pitié under the authority of Louis Henri Vaquez who introduced the use of the electrocardiogram and the recording of the jugular pulse into French medicine. During this period, Rivero Carvalho carried out several works, especially those dedicated to arterial pressure.
1934. He returned to Mexico with a solid education. He revalidated the title obtained in France at the National Autonomous University of Mexico. That year he obtained a position in the General Hospital of Mexico, in the cardiology service, founded by Ignacio Chávez Sánchez (1897-1979) – Chávez was the founder of the first cardiology journal and the first cardiology hospital in Mexico. In this institution, he acquired a great reputation as a semiotician.
1944. The Inter-American Society of Cardiology was constituted and the National Institute of Cardiology was inaugurated on April 18; Chavez was one of its founders. Chavez was one of its founders who occupied a position as head of clinical service as well as a researcher until 1970. He also dedicated himself to teaching as a professor of clinical medicine at the Faculty of Medicine of the UNAM (Universidade Nacional Autônoma do México).
1946. Rivero Carvallo published an article entitled “A sign for the diagnosis of tricuspid insufficiency”2. This article introduced a diagnostic maneuver that was tested in four different groups of patients: those with clinical evidence of tricuspid insufficiency, those with mitral valve disease without tricuspid involvement (or arrhythmias), those with rheumatic tricuspid valve disease with arrhythmias, and, finally, patients with heart failure or arrhythmia without rheumatic disease. In the test, the patient was asked to perform deep inspirations and maintain inspiratory apnea. In patients with tricuspid insufficiency, such a maneuver resulted in an increase in the intensity of the systolic murmur, with maximum intensity in the tricuspid area, radiating to the mesocardium and the liver. In addition to the reinforcement of the murmurs, Rivero Carvallo’s maneuver also changed the tone of the murmurs, turning them rough, like a steam jet3.
1950. Rivero-Carvallo described a maneuver for the diagnosis of tricuspid stenosis (TS). He found that inspiration resulted in an increase in the intensity of the diastolic murmur and the opening click4. The pathophysiologic explanation is that during deep inspiration, the intrathoracic pressure is reduced, increasing the return of blood through the vena cava to the right atrium (RA). This increases the pressure, velocity, and volume of blood flow through the tricuspid valve, intensifying the sounds originating in the diseased valve3 (Fig. 2).

The Rivero Carvallo maneuver
The patient is placed in the supine position and the stethoscope is positioned in the tricuspid area. Then, the patient is asked to take a deep breath. If the murmur does not increase or decrease in intensity, the Rivero Carvallo maneuver is considered negative. In this case, the murmur originates (is radiated) from the mitral valve. On the other hand, if in deep inspiration, the murmur increases in intensity (positive maneuver), it indicates that the murmur originates from the tricuspid valve. Why does this occur? When the patient takes a deep breath, the intrathoracic pressure decreases, which increases venous return to the right side of the heart during systole. When there is a greater volume of blood reaching the right ventricle, and there is valve regurgitation, more blood will be flow from the right ventricle to the RA during systole, thus increasing the intensity of the murmur on auscultation.
When listening to the murmur of tricuspid insufficiency, one can notice a variation of intensity: the holosystolic murmur increases in intensity with inspiration.
Luis Lasso Rodríguez Rivero Carvallo could confirm the origin of the murmur in 10 of 11 autopsies of patients with tricuspid regurgitation. In another work, performed by Dr. B. L. Fushdeler, the maneuver was positive in 75% of 300 cases of tricuspid regurgitation.
Rivero Carvallo described the use of his maneuver for the diagnosis of TS. Also in this valvular disease, deep inspiration with a reduction of intrathoracic pressure and increase of the return of blood to the right side of the heart intensifies the diastolic murmur. In September 1965, together with Ramirez-Jaime, Carvallo observed that with the progression of the disease, the diastolic murmur may disappear due to dilation of the RA associated with the thinning of its walls, which they called atrium papyraceum (“paper-thin atrium”)5.
Rivero Carvallo published several studies covering many aspects of cardiovascular disease, including rheumatic mediastinitis6, descending aortic ectasia7, apical impulse in tricuspid lesions8, atrial dilatation and descending aortic dilatation9, and apical double shock10. Carvallo is considered one of the great masters of Mexican cardiology, and his maneuver is the most used and well-known Mexican eponym.
1951. Rivero Carvallo described “atrium papyraceum” or thinning of the right atrial wall in patients with chronic TS11. He verified that the Rivero Cavallo sign was independent of heart rhythm or frequency, and that it could even be found in patients with atrial fibrillation11.
1959. Rivero-Carvallo and Garza de los Santos described differentiation between mitral and tricuspid mid-diastolic murmurs and sounds. Mid-diastolic murmurs start after the second heart sound (S2) and end before the first heart sound (S1). They are due to turbulent flow across the atrioventricular (mitral and tricuspid) valves during the rapid filling phase in mitral or TS stenosis. TS is best heard over the left sternal border with a rumbling character and a tricuspid opening snap with wide splitting of S1. The murmur may increase in intensity with inspiration (Carvallo’s sign). TS often occurs in association with mitral stenosis (MS). Isolated TS is often associated with carcinoid disease or right atrial myxoma. The murmur of MS murmur has a rumbling character and is best heard with the bell of the stethoscope in the area of the apical pulse with the patient in the lateral decubitus position. It is usually preceded by an opening snap. In general, the shorter the duration from S2 to the opening snap, the more severe the MS. However, this rule can be misleading in situations where the stenosis is so severe that the flow becomes reduced, or during high-output situations such as pregnancy where a less severe stenosis may still produce a strong murmur. In MS, a tapping apical impulse is present8.
1962. Rivero Cavallo describes the sign of a double apex impulse10.
Double systolic impulses are often present in hypertrophic cardiomyopathy and left bundle branch block. An extra impulse in late diastole occurs after atrial contraction; it corresponds to auscultation of the fourth heart sound and is observed in hypertrophied or noncompliant ventricles: systemic hypertension, aortic stenosis, hypertrophic cardiomyopathy, and during myocardial ischemia. An early diastolic impulse can correspond to the third heart sound and is found in normal hearts in young or slim patients or in patients with dilated ventricles in chronic heart failure or volume overload states. In the latter cases, the second impulse corresponds to the exaggerated “a” wave (Fig. 3A) that is normally not palpable and represents left ventricular filling during diastole. However, in states of elevated end-diastolic pressure, the “a” wave will increase and be palpable causing the “second” impulse. These states include left ventricular hypertrophy (aortic stenosis, hypertension, an hypertrophic cardiomyopathy), myocardial disease/cardiomyopathy, and non-compliant heart in myocardial ischemia. Both the observation and palpation of the point of maximal impulse (PMI) of the heart are part of a complete cardiac examination. These findings can yield important information about the heart such as a laterally displaced PMI in an enlarged heart.
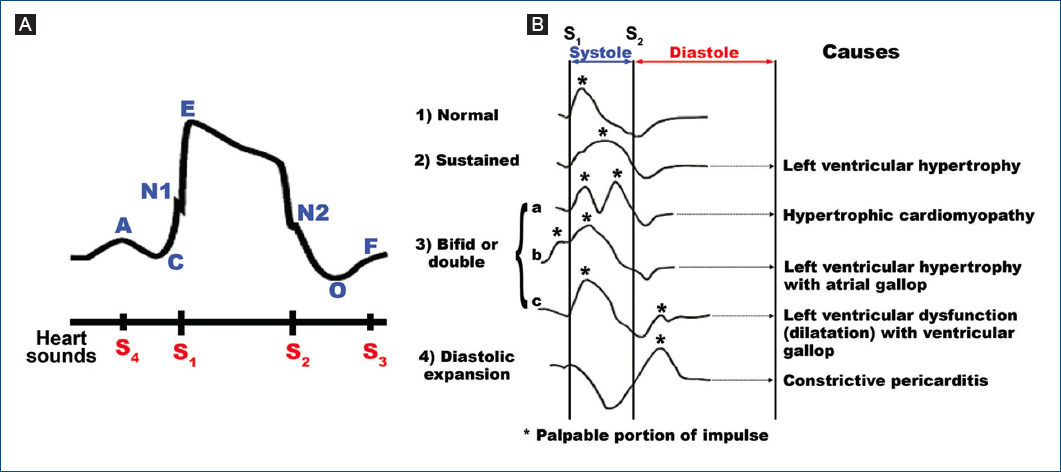
Figure 3 A: apical impulse: its timing and contour (A = left ventricular filling; C = systolic wave; E = systolic peak; O = start of rapid filling (mitral valve open); F = start of slow filling [diastasis]; and N = notch). B: systolic and diastolic contours in normal and some pathological circumstances.
The apex cardiogram
Figure 3A shows the curve created by the PMI measured by apex cardiogram. Although nowadays infrequently used, this device can aid in the diagnosis of ventricular abnormalities. Figure 3B shows a representation of normal contours and an indication of some pathologies.
In the same year, (1962) Rivero Cavallo described the left bronchial compression syndrome caused by the left atrial enlargement and dilatation of the descending aorta9. Aortic root dilatation or ascending aortic aneurysm may lead to symptoms of dyspnea due to aortic regurgitation, and compression of the left atrium (LA) or pulmonary veins may cause dyspnea12. Compression of these structures may impair left ventricular diastolic filling, which can result in shortness of breath. Occasionally, hemodynamic instability may develop as a result of decreased left ventricular filling13. Compression of the LA or pulmonary veins due to type A aortic dissection, descending aortic aneurysm, or pseudoaneurysm has been described. Compression of the LA and pulmonary veins by both ascending and descending aortic aneurysms is a rare condition.
1965. Rivero-Carvallo and Jaime Ramirez did further studies on atrium papyraceum (paper-thin atrium). As previously mentioned, these structural changes of the RA are caused by TS and are characterized by degeneration and thinning of the free wall of the RA and on occasion of the interatrial septum5. They studied 40 patients, 27 of them at autopsy. About 16% of the cases with TS had a paper-thin atrium at autopsy. The previous studies on tricuspid valvular disease had demonstrated that murmurs (diastolic and systolic) and other sounds (first sound and opening snap) originating from the tricuspid valve are louder during the post-inspiratory apnea. Some of the patients, however, had this increase in loudness only following several periods of post-inspiratory apnea. This was called the sign of the repeated maneuver. In other cases, these murmurs and sounds became fainter or even disappeared after inspiration, in spite of the fact that they were clearly heard during normal respiration and were reinforced during the post-inspiratory apnea. This was called the paradoxic sign. Patients with murmurs that increased only after several periods of post-inspiratory apnea (repeated maneuver) were classified as having Grade 1 paper-thin RA. Those with murmurs that became fainter or disappeared in the post-inspiratory apnea (paradoxic sign) were classified as having Grade 2 paper-thin RA. This classification corresponds to the extent of degeneration of the RA wall. In general, the clinical signs, the hemodynamic findings, and the extent of the structural changes found at autopsy were in agreement with this classification. The investigators provided an interpretation of the clinical findings, based on hemodynamic interpretation. The diagnosis was made on the basis of clinical data and on the changes of the tricuspid murmurs produced by single or repeated inspiration5. The Rivero Carvallo maneuver is mainly used to differentiate murmurs of tricuspid regurgitation from murmurs of mitral valve regurgitation.
1993. Rivero Carvallo died on February 15, 1993, at 88 years old.

