











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
Coronary artery vasospasm is a cause of chest pain described more than 50 years ago by Prinzmetal et al., named as variant angina1. Now, it is commonly known as Prinzmetal angina or vasospastic angina (VA). Patients with VA have episodes of oppressive chest pain, characterized by diurnal variation and not with exercise (even at rest), that have good response to short acting oral nitrates and oral calcium channel blockers (CCB)1. Some patients with VA develop malignant ventricular arrythmias during ischemic episodes that lead to sudden death2.
Although VA usually has a good response to oral nitrates and oral CCB, treatment of patients that cannot tolerate oral drugs (on the acute phase of sudden death, hemodynamically unstable or patients on mechanical ventilation) options are very reduced. In this case report, we present a patient with an outpatient aborted sudden death due to VA with frequent episodes of coronary arteries vasospasms with malignant ventricular arrythmias refractory to intravenous nitrates that responded to clevidipine, an intravenous CCB.
A 65-years-old male patient was brought to the emergency room due to out-of-hospital cardiac arrest. Past medical history of hypertriglyceridemia and was an active smoker. Chronic medication included atorvastatin 20 mg once daily (OD) and acetylsalicylic acid 100 mg (OD).
The patient suffered cardiac arrest while traveling on public bus and basic life support maneuvers were started until medical assistance arrived. The automated external defibrillator showed a ventricular fibrillation (VF) and after 2 shocks of 200 Joules (J) and 15 min of cardiopulmonary resuscitation maneuvers the patient recovered pulse. The 12-lead electrocardiogram (ECG) showed sinus tachycardia without signs of myocardial ischemia. The patient was transferred to the hospital with mechanical ventilation support.
Once on the emergency room, the patient was hemodynamically stable without vasoactive drugs. No remarkable findings on physical examination. The ECG showed a sinus tachycardia without alterations suggestive of myocardial ischemia (Fig. 1A). An emergency echocardiogram was performed and normal size non-hypertrophic left ventricle with mild global hypokinesia (no regional alterations in contraction suggestive of coronary artery disease) was found. Anyways, hemodynamics laboratory was contacted for an urgent coronarography to exclude myocardial ischemia as the cause of VF.
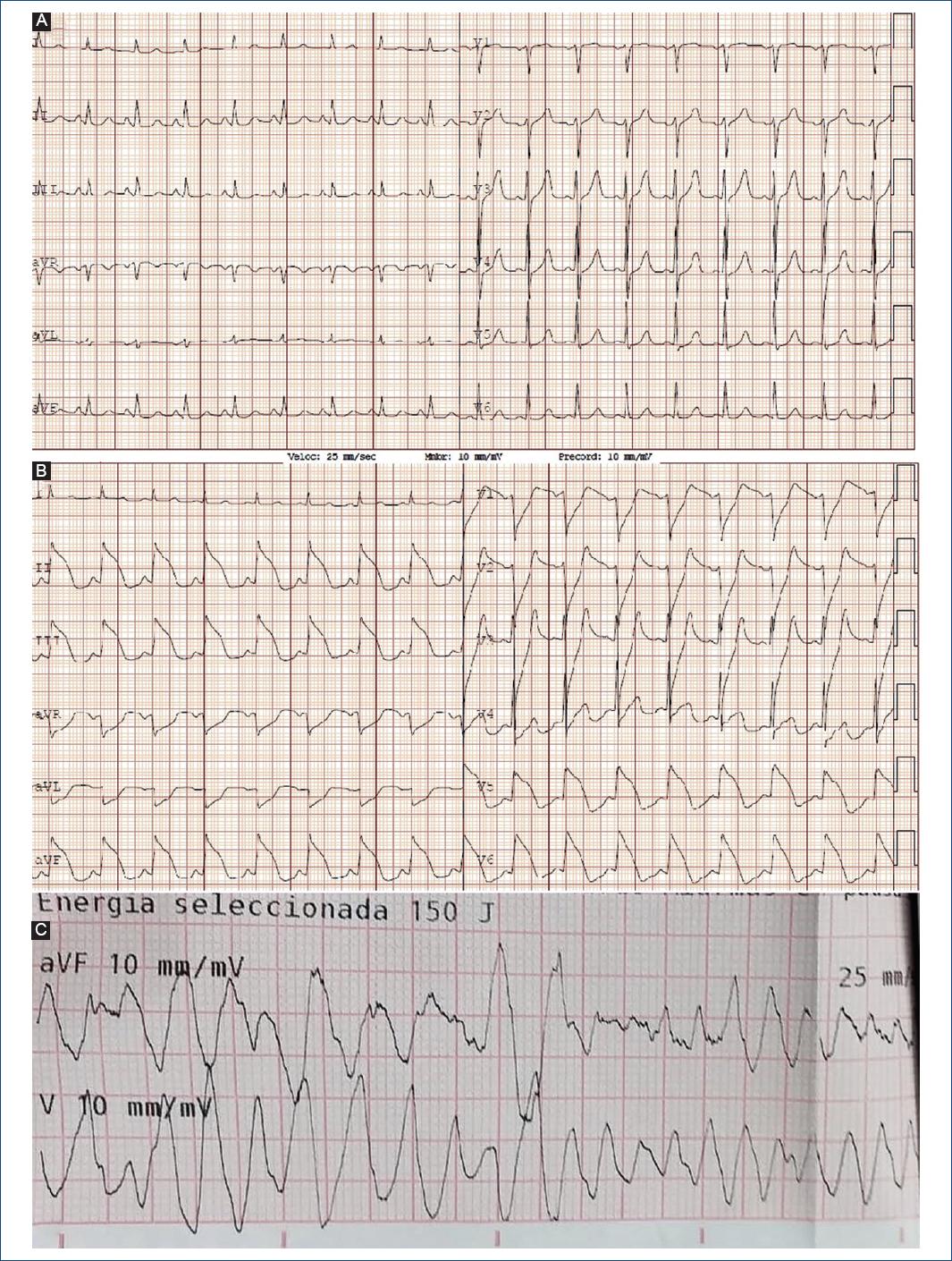
Figure 1 Twelve leads ECG at emergency room admission with no signs of myocardial ischemia A: ECG during catheter laboratory transfer preparation that shows a sinus rhythm to 98 bpm with a ST segment elevation on "Shark Fin” pattern on inferior and low lateral leads, with a specular ST segment depression on anterior and DI-aVL leads, these findings were consistent with a inferior, posterior and lateral STEMI B: episode of polymorphic ventricular tachycardia and ventricular fibrillation C: that was successfully defibrillated to sinus rhythm with 150 J direct current defibrillation.
While preparing to be transferred to the catheterization laboratory, the patient developed ECG alterations. A 12-lead ECG showed a inferior, posterior and lateral ST segment elevation myocardial infarction, Fig. 1B. During transfer the patient had four episodes of polymorphic ventricular tachycardia and one episode of VF (Fig. 1C) that was successfully defibrillated with one 150 J shock.
Emergent coronary angiography showed a diffuse vasospasm with a complete occlusion of the circumflex artery (Fig. 2A, bottom) with intraprocedural ST segment elevation (Fig. 2A, upper). An intracoronary bolus of 0.2 mg of nitroglycerin was administered. Control angiography showed improvement on coronary arteries caliber without significant atherosclerotic disease (Fig. 2B, bottom) with ST segment normalization (Fig. 2B, upper).
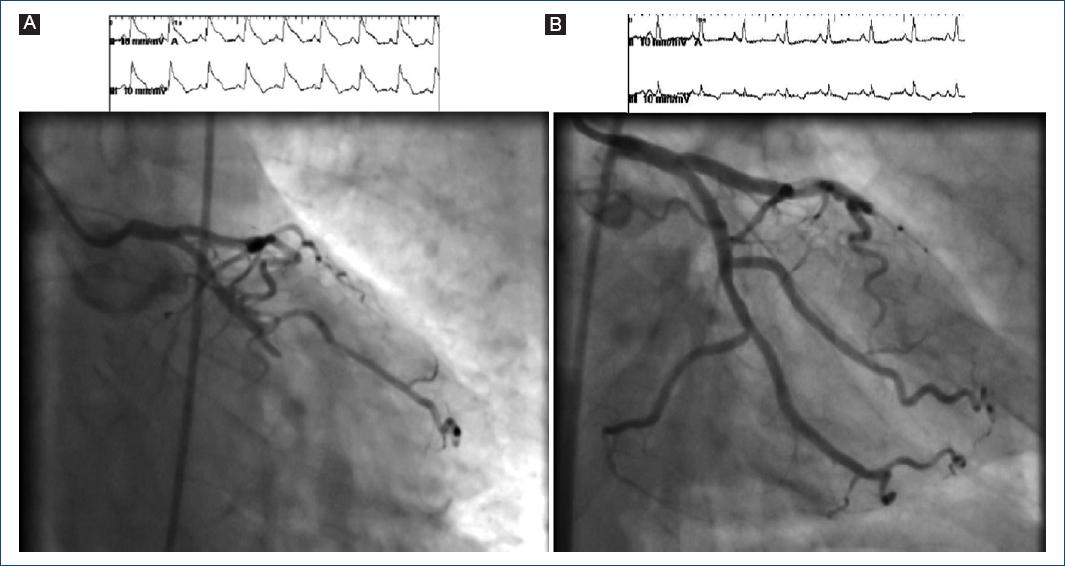
Figure 2 A: coronarography and continuous ECG during procedure. A diffuse vasospasm on the left coronary system with complete occlusion of circumflex artery distal to first marginal branch and concurrent ST segment elevation on continuous ECG B: after administration of 0.2 mg of intracoronary nitroglycerin, the vasospasm was reverted showing improvement on coronary arteries caliber, without significant atherosclerotic disease and normalization of ST segment changes on ECG.
Blood test showed elevated ultrasensitive T troponin at admission, with a peak at 3 h 181 ng/L (normal value < 14 ng/L). The chest X-ray was normal. The patient was admitted in the intensive care unit under mechanical ventilation and nitroglycerine infusion at 20 micrograms/min. Hours later, and despite intravenous nitrates, he presented various episodes of coronary vasospasm with ST segment elevation, NSVT, and VF, that were successfully defibrillated. An infusion of clevidipine (fast acting intravenous CCB) at 4 mg/h was initiated, stopping nitroglycerine infusion to avoid hypotension, since the patient had an invasive systemic blood pressure of 130/76 mmHg. The patient maintained an invasive blood pressure over 90/50 mmHg and no dose reduction was needed due to blood pressure concern, since peripheral perfusion and urine output were favorable. After 24 h of clevidipine infusion, the patient didn’t have more coronary vasospasm episodes.
Two days later the patient was extubated with good neurological condition. Clevidipine was changed by oral diltiazem 30 mg every 8 h. Two ways later was up titrated to 60 mg every 8 h (maintained at discharge and associated to a statin, acetyl salicylic acid 100 mg and clopidogrel 75 mg o.d., as part of acute coronary syndrome treatment) without new events. The patient was discharged without an implantable cardioverter defibrillation (ICD) since he had a good response to oral CCB without new ischemic or arrhythmic events during in hospital continuous ECG telemetry. Eighteen months later the patient was stable without episodes of chest pain or syncope. Even though on this patient ambulatory Holter was not performed, it could be and option for screening for ST segment changes or ventricular arrhythmias.
Discussion
In this report, we present the case of a 65-years-old man that presented a cardiac arrest due to a coronary vasospasm. Despite he had good initial response to intravenous nitrates infusion, later he had recurrent episodes. This nitrate was changed by a clevidipine infusion, which controlled coronary spasms.
Clevidipine is an intravenous CCB of the dihydropyridine family, fast acting (blood esterase metabolism), and very short half-life (approximately 1 min) that is approved for treatment of hypertension3. Clevidipine has no direct effect on myocardial inotropism3,4 and unlike nitroglycerine it does not affect preload, while it may cause mild reflex tachycardia due to decrease vascular systemic resistance4. This drug has been successfully used during cardiac surgery to avoid vasospasm of internal mammary artery and radial artery4 and for treatment of acute hypertension5. Clevidipine was elected over verapamil (and other non-dihydropyridine CCB) since it has no negative inotropism, it’s very fast onset of action and very short effect, what makes it idoneal for acute spastic episodes in patients that could develop significant arterial hypotension.
One previously reported case also used clevidipine for treatment of VA with good result (off-label use)6, but it was used in combination to nitroglycerine. Clevidipine is not approved for treatment of VA, but it is believed that the CCB have a family-related effect on the vascular physiology3 and its very fast onset of action could make it pharmacologically ideal for treating acute vasospastic episodes in patients with inadequate response (or even refractory) to nitrates. The patient on this case had an impressive response to clevidipine, even when vasospastic episodes could not be mitigated with intravenous nitrates. The role that this drug could play on patients with acute treatment-refractory vasospastic episodes should be further studied.
The principal risks factors for developing SCA in patients with VA are hypertension, hyperlipidemia, multivessel spasm, and spasm involving left anterior descending artery7. The 2017 AHA/ACC/HRS guidelines for management of patient with ventricular arrhythmias have introduced a specific recommendation for ICD implantation in these situations with level of recommendation class IIb8. Results of a study suggest that outcome of patients with VA that had an aborted SCA have a worst prognosis than other patients with VA but without sudden death2. The final decision for ICD implantation should be individualized.

