











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkThe high-grade undifferentiated pleomorphic cardiac sarcoma (UPS) is the second most common primary malignancy in the heart; usually remains asymptomatic, until they produce a mass effect or embolization. A 47-year-old female previously healthy was admitted for a 7-day history of progressive dyspnea. At physical examination, there was mitral regurgitant murmur Grade III and bilateral crepitation rales; the electrocardiogram detected sinus tachycardia (Fig. 1A) and X-ray showed Grade II venocapillary hypertension and pleural effusion (Fig. 1B). The echocardiogram revealed an intracardiac mass in the left atrium of 36 mm × 48 mm, protruding through the mitral valve, conditioning moderate stenosis and severe insufficiency (Fig. 1C-E). Surgical treatment was realized with resection of the tumor, partial resection of the posterior wall of both atrial and interatrial septum, and mitral commissuroplasty. The histological sections showed a solid-appearing neoplastic proliferative lesion with lax isolated areas of myxoid appearance, short cellular bundles, and branched vessels with extensive myocardial infiltration and infiltration of the valvular tissue (Fig. 2A-C). Thoracoabdominopelvic tomography showed no evidence of metastatic disease. Treatment was started with chemotherapy, but she had progressive deterioration and died 3 months later. Cardiac sarcoma has an incidence of ~ 1.7% of cases; survival at 10 years is 90% in low-grade sarcomas, 60% with intermediate grade, and 20% with high degree1. The treatment is surgical resection followed by chemotherapy2, however, the invasive nature of UPS makes it difficult to obtain surgical margins without tumor activity, associated with relapse and poor short-term prognosis3.
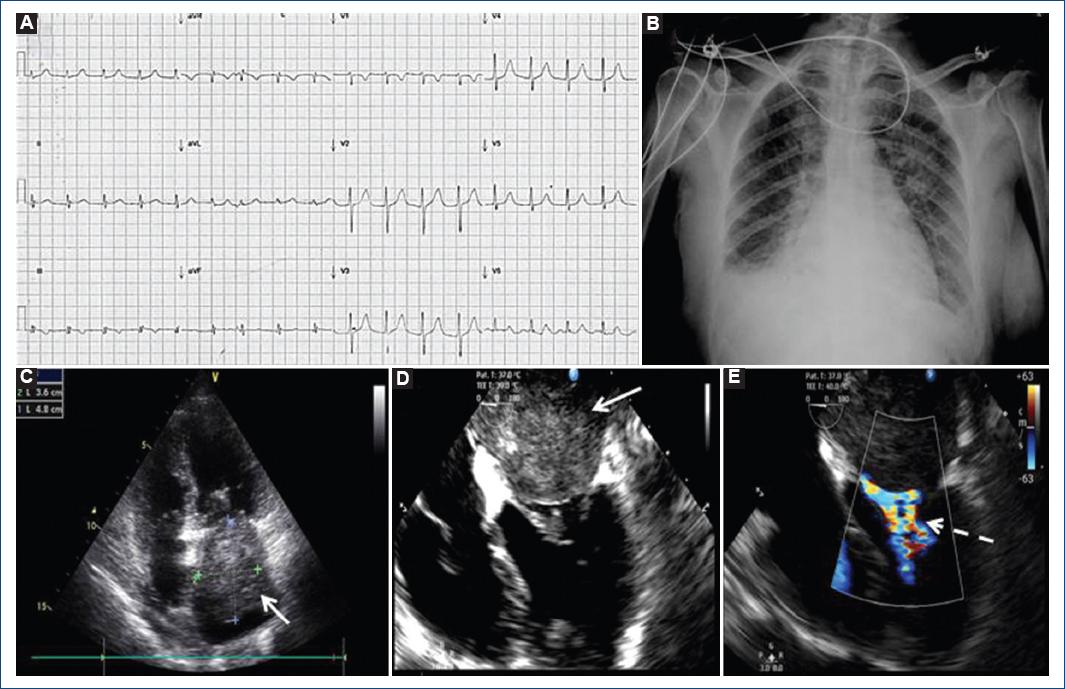
Figure 1 Electrocardiogram and multimodality imaging approach of undifferentiated pleomorphic cardiac sarcoma. A: 12-lead electrocardiogram shows sinus tachycardia; B: chest X-ray with Grade II venocapillary hypertension and pleural effusion; C: four chambers image by transthoracic echocardiogram, showing intracardiac mass (arrow) located in the left atrium; D: transesophageal echocardiogram confirms mass in the left atrium (solid arrow) adhered to the posterior wall of 48 mm × 34 mm and E: Doppler color showed obstruction of the left ventricle inflow tract (dashed arrow).
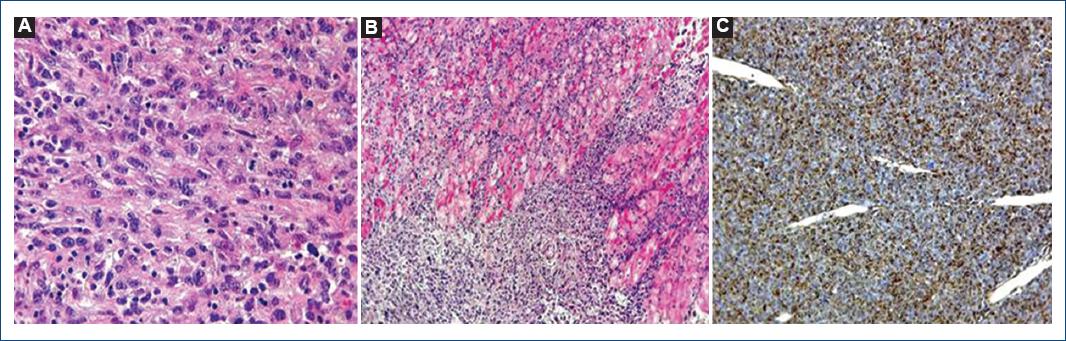
Figure 2 Histological sections of undifferentiated pleomorphic cardiac sarcoma. A: the neoplastic cells have an epithelioid or spindle cell appearance with pleomorphic nuclei, atypical mitosis, and scarce lymphocytic infiltrate (HE, 400 ×); B: extensive myocardial infiltration is shown by pleomorphic neoplasm with a solid pattern (HE, 100 ×); C: immunohistochemical staining with positive cytoplasmic anti-vimentin antibody (ocher color) in most of the neoplastic cells (100 ×). HE: Hematoxylin-eosin.

