










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkArchivos de cardiología de México
On-line version ISSN 1665-1731Print version ISSN 1405-9940
Arch. Cardiol. Méx. vol.83 n.4 Ciudad de México Oct./Dec. 2013
https://doi.org/10.1016/j.acmx.2013.03.002
Artículo de revisión
About the specialized myocardial conducting tissue
Acerca del tejido miocárdico especializado de excitoconducción
Alfredo de Micheli Serraa,*, Pedro Iturralde Torresb, Alberto Aranda Fraustroc
a Research Fallow, Instituto Nacional de Cardiología Ignacio Chávez, Tlalpan, DF, Mexico.
b Department of Electrocardiology, Instituto Nacional de Cardiología Ignacio Chávez, Tlalpan, DF, Mexico.
c Department of Patology, Instituto Nacional de Cardiología Ignacio Chávez, Tlalpan, DF, Mexico.
* Corresponding author:
Juan Badiano, No. 1, Col. Sección XVI,
Tlalpan, México DF, C.P. 14080, Mexico.
E-mail address: alessandro.micheli@cardiologia.org.mx (A. de Micheli Serra).
Received 5 November 2012.
Accepted 21 March 2013.
Abstract
The chronological succession of discoveries on the location and structure of the atrio-ventricular conducting system are described. The starting point of this system is located in the sinus atrial node, identified by the English scientists A. Keith and M. W. Flack in 1907. The atrioventricular conducting system was pointed out by the Swiss physician Wilhelm His Jr. in 1893. The atrioventricular node (AV) was first identified by the Japanese pathologist Sumao Tawara and his German professor Ludwig Aschoff in 1906.
Likewise the structure and routes of the three internodal bundles are described. These bundles include: Bachmann's bundle (1916) connecting the right with the left atrium and the AV node; the middle Wenckebach's bundle (1910) and the posterior or Thorel's bundle (1910), extending from the region of the sinus atrial node towards the posterior margin of the AV node.
Lastly, the ventricular left and right conduction systems are detailed. These include the main trunk and their peripheral subdivisions with respective networks. Regarding the controversial existence of the left middle subdivision, it can exist in animal and human hearts. Nevertheless, an intermediate left septal network of specialized fibers seems to act as a functional equivalent of this subdivision.
Keywords: Myocardial specialized conducting system; Left ventricular conducting system; Right ventricular conducting system; Mexico.
Resumen
Se describe, en orden cronológico, la sucesión del descubrimiento de la localización y la estructura de los componentes del sistema de conducción auriculoventricular. El haz de conducción AV fue descrito por el médico suizo Wilhelm His Jr. en 1893. El punto de origen de dicho sistema se halla en el nodo sinoauricular, identificado por los ingleses A. Keith y M.W. Flack en 1907. El nodo auriculoventricular (AV) fue identificado por el patólogo japonés Sunao Tawara y su maestro, el alemán Ludwig Aschoff, en 1906.
Asimismo se relatan la estructura y los recorridos de los 3 haces internodales: el anterior o de Bachmann (1916), que conecta la aurícula derecha con la izquierda y el nodo AV; el medio o haz de Wenckebach (1910) y el posterior o haz de Thórel (1910), que se dirige desde la región del nodo sinoauricular hacia la aurícula izquierda y el margen de atrás del nodo AV.
Se presentan asimismo, de forma esquemática, los sistemas de conducción ventricular izquierdo y derecho, que comprenden el tronco principal y las subdivisiones periféricas con sus respectivas redes de Purkinje. Respecto a la controvertida existencia de un fascículo izquierdo medio, éste sí puede existir en corazones humanos y de animales. Pero la red septal intermedia de fibras especializadas parece ser un equivalente funcional de dicho fascículo.
Palabras clave: Sistema cardiaco de excitoconducción; Sistema de conducción ventricular izquierdo; Sistema de conducción ventricular derecho; México.
The specialized myocardial excitoconducting tissue includes several sections. The first component is the sinoatrial (SA) node, the primum movens (first mover) of normal cardiac activity, described by the English A. Keith and M.W. Flack in 1907.1 It is located in the sulcus terminalis and extends from the recess of the right atrial appendage to the intercaval band.2 The atrioventricular conduction system originates in the homonymous node (atrioventricular node) identified by Tawara and Aschoff.3 The anatomy of the aforementioned node has been carefully studied by James.4,5
The AV node is found in the inferior portion of the inter-atrial septum or, to put it more accurately, the AV node lies in what can be defined as the fibromuscular atrioventricular septum. It is located between the orifice of the coronary sinus in the right atrium and the septal leaflet of the tricuspid valve, to the right of the central fibrous body (trigonum fibrosum) where it joins the mitral annulus.5
In the human heart, there are three connections between the SA and the AV nodes, containing Purkinje fibers as well as non-specialized myocardial fibers.6,7 The anterior bundle,8 otherwise known as Bachmann's bundle, connects the SA node with the left atrium where it turns backwards and descends to the interatrial septum towards the AV node. The middle internodal or Wenckebach's bundle9 extends from the dorsal and posterior margins of the SA node and runs behind the superior vena cava through the intercaval sul-cus towards the crest of the interatrial septum. From there, it extends towards the AV node, intersecting with fibers proceeding from the anterior bundle as it approaches the node in the inferior portion of the interatrial septum or, what might be better called, the fibromuscular atrioventricular septum. This means, it lies between the entry of the coronary sinus in the right atrium and the septal leaflet of the tricuspid valve. It lies, thus, to the right of the central fibrous body. The posterior internodal bundle described by Thorel10 follows the crista terninalis from the AV node to the Eustachian ridge and, from there, runs along the same ridge to the posterior margin of the AV node.
Atrioventricular conduction system
The atrioventricular conduction system originates in the AV node with the bundle of His. The bundle of His was described by the Swiss doctor, Wilhelm His Jr. (1863-1934) and comprises the common trunk and the left and right ventricular systems.11 The first, evidenced by Sunao Tawara, using his-tological staining with Chinese ink in the human heart and several animal species, has been localized in recent times by different staining methods. In the canine heart, the bundle is evidenced using iodine-potassium iodide solution (Lugol's solution), because the specialized tissue it contains is very rich in glycogen that has high affinity for iodine. This system can also be stained by Lugol's solution in the human heart.
Left ventricular conduction system
This system is composed by the main trunk of the left branch, which is short (2 or 3 mm) and soon gives rise to two subdivisions: the anterior subdivision located in the left superior septal mass, and the posterior subdivision with branches that run to the posterior wall of the left ventricle.12
In the canine heart, an entanglement of fibres (intermediary network), branches off from this main trunk and the two subdivisions. This network appears to be the functional equivalent of a middle bundle, distributed in the left septal mass of the medial-third of the interventricular septum12 (Fig. 1). Each of the left subdivisions end in the network of endocardial and subendocardial specialized fibers observed by J.E. Purkinje in 1839 and identified histologically by himself a few years later.13

Through the fibers that form the intermediate network, activation impulses may reach the left septal mass and its endocardial surface where the process of ventricular activation starts.14 This process manifests as the first septal vector, i.e., the first vector resulting from ventricular activation.14
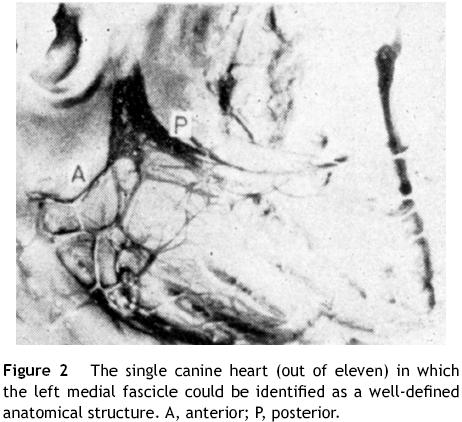
Regarding the ''left middle subdivision'', which is the object of current controversies, it is worth pointing out that we have been able to identify it as a well-defined anatomical structure in only one of eleven canine hearts (Fig. 2).
In all of these cases, we stained the left ventricular conduction systems with concentrated Lugol's solution.12 We have not intentionally searched for it in the human heart. However, it should be recalled that Tawara himself had identified this fascicle in human heart using Chinese ink,15 and the Belgian cardiologists Demoulin and Kulbertus16 have found it through appropriate septal dissections in eleven of twenty human hearts. These authors reported that using the same procedure they were able to identify the middle subdivision in another series of 49 cases in 33 (67%) human hearts.17 In 17 cases, the fascicle branched off the main trunk of the left ventricular system, in 7 cases it arose from the anterior subdivision, and in 9 cases it branched off the posterior subdivision (Fig. 3). Thus, the middle fascicle does exist in human and animal hearts, but activation impulses may also be transmitted through the intermediate network of specialized fibers to activate the medial left septal mass where the first vector resulting from ventricular myocardial depolarization originates. This event would explain the persistent beginning of a normal activation process in hearts, devoid of this fascicle and even in the presence of so-called trifascicular blocks.18,19

Right ventricular conduction system
The main trunk of the right branch of the bundle of His follows a longer horseshoe shaped trajectory with its initial portions running quite superficially. Its medial portions turn deep into the thickness of the homolateral septal mass: pars mimetica. The distal portions become superficial again at the limit of the medial and inferior third5 of the right septal surface, near the base of the anterior papillary muscle, where it divides into three branches. These subdivisions have been found in the canine heart20,21 and in human hearts.22,23 The anterior subdivision21 spreads in the region of the pulmonary artery cone and lies in the dihedral angle formed by the right anterosuperior septal mass and the anterior wall of the right ventricle. The middle subdivision, which branches off the main trunk of the branch at a right angle, divides into several branches in the right anteroinferior septal mass. The posterior subdivision lies in the right posterior septal mass with numerous fillets that are distributed in the posterior, and medial and inferior lateral regions of the homolateral free ventricular wall. Each subdivision ends in the corresponding Purkinje network. Fig. 4 illustrates the right ventricular conduction system in a canine heart. In 1913 the existence of the Kent bundle24 was identified.

Conclusions
Peripheral on distal left blocks that may hide the coexistence of a non-activable myocardium25 can be easily recognized by the diagnostic approach proposed, in due time, by the Mexican School of electrovectorcardiography. The correct diagnosis of a peripheral left ventricular conduction disorder together with pertinent clinical data should suggest the probable association of a non-activable myocardium.25
On the other hand, right distal peripheral blocks generally do not hide the electrical signs of a non-activable myocardium.26 These blocks enhance the manifestations of later occurring electromotive forces resulting from right ventricular activation. Therefore, they do not interfere with the development of ventricular electromotive forces in the zones affected by myocardial injury. This happens both in the presence of a right anterior subdivision block, which increases by at least 10 ms the duration of basal electromotive forces that normally develop in 64 -72 ms27 and in the presence of a right posterior subdivision block. This latter block prolongs by an average of 12 ms the electromotive forces originating in the posterior and medial and inferior posterolateral septal regions of the right ventricular free wall, which become activated in 30 -45ms.28
The middle left fascicle may in fact exist in human and animal hearts, but its presence does not appear to be indispensable for transmission of activation impulses to the medial left septal mass.
Acknowledgment
The authors greatly appreciate the careful collaboration secretarial of Mrs. Blanca Lilia Ochoa.
References
1. Keith A, Flack MW. The form and nature of the muscular connections between primary divisions of the vertebrate hearts. Anat Physiol. 1907;41:172-89. [ Links ]
2. Lev M. The normal anatomy of the conductive system in man and its pathology in atrioventricular block. Ann N Y Acad Sci. 1964;111:817-29. [ Links ]
3. Tawara S. Das Reizleitungssystem des Saugetierherzens. Jena: Gustav Fisher ed.; 1906. [ Links ]
4. James TN. Anatomy of the human sinus node. Anat Rec. 1961;141:109-39. [ Links ]
5. James TN. Morphology of the human atrio-ventricular node, with remarks pertinent to its electrophysiology. Am Heart J. 1961;62:756-71. [ Links ]
6. James TN. The connecting pathways between the sinus node and the A -V node and the A-V node and the right and left atrium in the human heart. Am Heart J. 1963;66: 498 -508. [ Links ]
7. James TN, Sherf L. Specialized tissues and preferential conduction in the atria of the heart. Am J Cardiol. 1971;23:371-427. [ Links ]
8. Bachmann G. The interauricular time interval. Am J Physiol. 1916;41:309-20. [ Links ]
9. Wenckebach KF. Beiträge zur Kenntnis der menschliken Herztätigkeit. Arch Anat Physiol. 1907;1-2:1-24. [ Links ]
10. Thörel C. Über den Aufbau des Sinusknotens und seine Verbindung mit der cava superior und den Wenckebachschen Bundein. Munchen Med Wschr. 1910;57:183-6. [ Links ]
11. His Jr W. Die Thätigkeit des embryonen Herzens und deren Bedeutung für die Lehre von der Herzbewegung beim Erwachsenen. Arbeiten aus med Klin zu Leipzig. 1893:14-50. [ Links ]
12. Medrano GA, Brenes C, de Micheli A, Sodi Pallares D. El bloqueo simultáneo de las subdivisiones anterior y posterior de la rama izquierda del haz de His (bloqueo bifascicular), y su asociación con bloqueo de la rama derecha (bloqueo trifascicular). Arch Inst Cardiol Mex. 1970;40:752-70. [ Links ]
13. Purkinje JE. Mikrosckopisch neurologische Beobachtungen. Arch Anatom Physiol Wissenchaliche Med. 1845;12:281. [ Links ]
14. Sodi Pallares D, Bisteni A, Medrano GA. Electrocardiografía y Vectocardiografía deductivas. México. La Prensa Méd Mexicana. 1964:103. [ Links ]
15. Akiyamuri T. Sunao Tawara: discoverer of the atrioventricular conduction system of the heart. Cardiol J. 2010;17:428-33. [ Links ]
16. Demoulin JC, Kulbertus HE. Histopathological examination of concept of left hemiblock. Br Heart J. 1972;34:307-14. [ Links ]
17. Demoulin JC, Kulbertus HE. Pathological correlates of intra-ventricular conduction. In: Masoni A, Alboni P, editors. Cardiac electrophysiology today. Londres, UK: Academic Press Inc; 1982. p. 427-35. [ Links ]
18. Medrano GA, de Micheli A, Brenes C, Sodi Pallares D. Experimental bases for diagnosis of left bifascicular and trifascicular blocks. G Ital Cardiol. 1975;5:8-18. [ Links ]
19. De Micheli A. Los bloqueos parciales de la rama izquierda del haz de His. Arch Inst Cardiol Mex. 1971;41:625-8. [ Links ]
20. Uhley HN, Rivkin LM. Peripheral distribution of the canine A-V conduction system. Observations on gross morphology. Am J Cardiol. 1960;5:688-91. [ Links ]
21. Medrano GA, de Micheli A. Contribución experimental al diagnóstico de los bloqueos fasciculares derechos. Arch Inst Cardiol Mex. 1975;45:704-15. [ Links ]
22. Lev M. The conduction system. In: Gould S, editor. Pathology of the heart and blood vessels. Springfield, IL: Charles C. Thomas; 1968. p. 185. [ Links ]
23. Mahaim J. Les maladies organiques du faisceau de His-Tawara. Paris: Ed. Masson & Cie; 1931. [ Links ]
24. Kent AFS. A neuromuscular mechanism in the heart. Trans Intern CongrMed Londres. 1913;Section III:102-8. [ Links ]
25. De Micheli A, Medrano GA. Bloqueos periféricos. In: de Micheli A, Medrano GA, Iturralde P, editors. Diagnóstico electrovecto-cadiográfico en clínica. México: Méndez Editores. S.A.; 1992. p. 44 -52. [ Links ]
26. Medrano GA, de Micheli A, Iturralde P. Peripheral heart blocks associated with myocardial infarcts. Clinical diagnosis based on experimental findings. Curr Cadiol Rev. 2008;4:140-7. [ Links ]
27. De Micheli A, Medrano GA. Electrocardiograma y vectocadio-grama en el infarto del miocardio. México: La Prensa Médica Mexicana; 1971. p. 34. [ Links ]
28. Gallagher JJ, Sealy WL, Richet LE, LanW, Wallace AG. Epicardial mapping in the WPW syndrome. In: Welsen AA, editor. Review of contemporary laboratory methods. Am Heart Ass. Inc; 1980. [ Links ]

