










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkArchivos de cardiología de México
On-line version ISSN 1665-1731Print version ISSN 1405-9940
Arch. Cardiol. Méx. vol.79 n.2 Ciudad de México Apr./Jun. 2009
Comunicaciones breves
Clinical evidence of the antiarrhythmic effect of a magistral suspension of propafenone: A case report
Evidencia clínica del efecto antiarrítmico de una suspensión extemporánea de propafenona. Reporte de un caso
Lina Barranco–Garduño,1,2 Janett Flores–Pérez,1,2 Hugo Juárez–Olguín,1,2 Jesús Bobadilla–Chávez,3 Héctor Osnaya,3 y Carmen Flores–Pérez1*
1 Laboratorio de Farmacología, Instituto Nacional de Pediatría (INP). México, D.F. México.
2 Departamento de Farmacología, Facultad de Medicina, Universidad Nacional Autónoma de México. México, D.F.
3 Servicio de Cardiología, INP.
* Corresponding author:
Carmen Flores Pérez.
Avenida Imán No.1 3er piso, Colonia Cuicuilco,
04530 México, D.F. México.
Telephone Et Fax: (55) 5255–1084–3883.
Correo electrónico: cfp3575@yahool.com.mx
Received: July 4, 2007.
Accepted: December 15, 2008.
Abstract
Propafenone is an antiarrhythmic that has been used for the treatment of tachiarrytmias in both adults and children. The aim of this study was to analyze the pharmacologic effect of a magistral suspension of propafenone, due to lack of an adequate commercial formulation for use in children. In this study we present, a case of a 2–year–old boy that was diagnosed with Wolff–Parkinson White syndrome and treated with a magistral suspension of propafenone. He has now been one year with no symptoms, no tachycardia and no cyanosis. The clinical status of the patient under treatment with propafenone was improved through constant medical care in the Cardiological Health Care Unit. The use of a magistral formulation of propafenone developed in our laboratory offers a temporal solution due to lack of medicines for children.
Key words: Antiarrhythmic agent; Children; Pharmacology; Propafenone; Supra ventricular tachycardia; Mexico.
Resumen
La propafenona es un antiarrítmico utilizado para el tratamiento de taquiarritmias tanto en niños como en adultos. El objetivo de este estudio fue analizar el efecto farmacológico de una suspensión extemporánea de propafenona, debido a la falta de una presentación comercial adecuada para uso en niños. Se trata de un niño de 2 años de edad diagnosticado con síndrome Wolff–Parkinson White, quien fue tratado con la preparación extemporánea de propafenona. Antes del tratamiento el paciente presentó taquicardia supraventricula; durante el seguimiento y bajo el tratamiento mencionado el paciente no mostró datos de taquicardia, ni cianosis, ni efectos adversos. El estado clínico del paciente bajo tratamiento con propafenona mejoró a través del constante cuidado médico por parte de la Unidad de Cuidados Intensivos del Servicio de Cardiología. El uso de una formulación extemporánea de propafenona desarrollada en nuestro laboratorio ofrece una solución temporal ante la falta de medicamentos para niños.
Palabras clave: Antiarrítmicos; Farmacología; Niños; Propafenona; Taquicardia supraventricular; México.
Introduction
Supraventricular tachycardia (SVT) is frequently manifested in emergency pediatric care units and is difficult to solve because the hemodynamic state of the patient may be involved.
The frequency of this disorder ranges from 1 in 250 to 1000 children.1 Forty percent of children who has SVT suffer from factors that predispose them to this condition, such as congenital heart disease, Wolff–Parkinson–White (WPW) syndrome, infections, fever or adverse reactions due to exposure to various different drugs. SVT is characterized by episodes of rapid cardiac rhythm caused by abnormal electrical circuits in the heart. The electrocardiogram (EKG) shows short PR interval, delta wave and complex prolongation of QRS. Propafenone is beta–blocking drug recommended for the treatment of SVT. It acts as a potent sodium channel blocker and is a weak b–adrenergic and calcium antagonist. Its main electrophysiological effect is to slow down conduction in tissues of quick response. Due its main electrophysiological effects, propafenone has a wide spectrum of activity and efficacy for the treatment against SVT including those of the WPW syndrome and recurrent atrial fibrillation. It has also been used safely in the treatment o various tachyarrhythmias among children.2 The efficacy and safety of propafenone for the treatment of infantile arrhythmia has been reported, with an average dose of 300mg/m2/day (ranging from 250–400 ng/mL) every 8h.3 Children with SVT were successfully treated with this drug without adverse or proarrhythmic effects. Due to its pharmacokinetic characteristics, propafenone has variable bioavailability when taken orally.4 The therapeutic plasmatic concentrations are between 0.2 and 1.5μg/ mL, following a dose of 150–200 mg/m2/day, with a dose increase of up to 600 mg/m2/day.5 Its elimination is of 11 mL/min/kg. Though uncommon, especially in cases of very high doses, adverse effects include lack of appetite, bloating sensation, feeling of nausea, bitter taste, and in some cases blurred vision and dizziness.6
Clinical case
The case of a 2–year–old boy, born and resident in Xochimilco, Mexico City, who had been given cardiological health care at the National Pediatric Institute from May 2005 (since the age of four months) is described. The boy was diagnosed with secondary SVT of the WPW syndrome, and treated with a magistral suspension of propafenone, starting May 2005. The drug was prepared according to an approved formula tested previously in laboratory studies.7 The mother is an apparently healthy 29–year–old housewife; the father, aged 31 years, has a degree in hotel administration, is apparently healthy and smokes 3/24, whilst denying alcoholism or drug addiction. The parents mentioned genetic inheritance of arterial hypertension on the paternal side and the patient has an apparently healthy 4– year–old brother.
This child is the outcome of a second pregnancy, which evolved normally with prenatal control from the first term of gestation, and the mother reported consuming iron and folic acid. It is reported that during the 37th week of gestation, an abdominal ultrasound was carried out which indicated extreme fetal suffering, due to nuchal cord, which required an urgent cesarean section to be carried out on February 16, 2005, producing a single outcome, with an Apgar score of 7/9, at 37 weeks of gestation, weight of 2.500 kg, size 49 cm, without any complications at birth, the child and mother left the hospital 72 hours later. He was breast fed until the end of the first year, taking solids at 6 months, and is currently incorporated into the family diet, which includes; vegetable consumption 3–4/7, fruit 7/7, red meat 4/7 and green vegetables 3/7, egg 1/7, milk and derivatives 3/7, pulses 1/7. He does not eat lentils or beans, only in soup. Psychomotor development was as follows: social smile at four months, sitting up at 6/2, crawling 8/2, with walking now in process. His vaccines are complete.
His current illness began on May 11, 2005, suffering from tachycardia, sweating and indications of poor perfusion, suffering from sweating with a cardiac frequency of 310 per minute and general signs of poor perfusion; together resulting in a diagnosis of SVT.
After non effective vagal stimulation maneuvers, propafenone was administered intravenously, however, due to unsuccessful therapeutic actions, patient underwent one attempt of transthoracic electrical cardioversion to restore normal sinus rhythm (Figure 1).
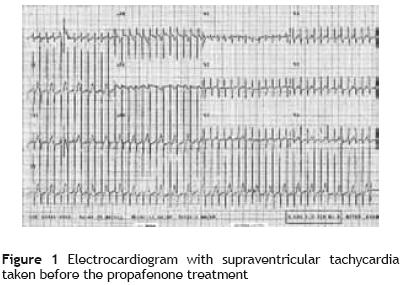
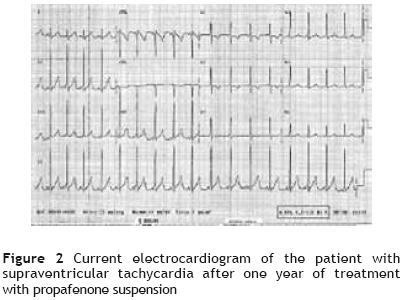
The child was placed in the Intensive Therapy Unit to monitor and stabilize hemodynamic activity and was discharged on May 15, 2005. From the time he was placed in hospital, he received treatment with a magistral suspension of propafenone as previously was mentioned, he received at the beginning 3 mg/8h for 4 months, followed by 6 mg/8h, and finally 11 mg/8h. He has been without symptoms for the last year. Figure 1 shows an EKG with SVT that was taken before propafenone treatment. Figure 2 shows the current EKG with SVT of the patient after one year of treatment with propafenone suspension.
Discussion
Research undertaken in the pharmacological laboratory of the National Pediatric Institute includes the development and evaluation of drugs at adequate doses for pediatric use, which are currently not available in our country. On this occasion, a magistral suspension was prepared using commercial tablets. The suspension was prepared by grinding 1 tablet of 150 mg of hydrochloride propafenone (Norfenon, Abbott Lab, Mexico) in a mortar. The finely ground tablets were then powdered and forced to pass through a mesh (size 100) in order to homogenize the particle size. Pomegranate syrup (La Madrileña, Mexico), which was used as diluent, was added to obtain a final concentration of 1.5 mg/mL of propafenone.
The obtained suspension was subjected to stability tests over a 90 day period, stored at room temperature (15 ± 5 °C) and refrigeration (3–5 °C), and turned out to be stable; neither physicochemical changes nor microbiological growth were observed. High performance liquid chromatography was used to validate dosage and to determinate the plasmatic levels of the drug.8
Previous to this study we carried out an analysis of the bioavailability of the suspension utilized for the present study compared with commercial tablets.7 The results of that study showed acceptable value of bioavailability as previously reported.9 Results demonstrate the reliability to administrate the drug. Plasma levels observed in children with SVT reached concentrations after they took the suspension. There are not reports in children that mention therapeutics range of propafenone, in this study we found that plasma concentration of drug was correlated with the clinical improvement of patients. The EKG done simultaneously during monitoring of propafenone showed an improvement respect initial exam reported during the diagnostic process.
To monitor propafenone levels in the patient, concentration of drug was measured at 3.5 h post administration, obtaining 11.7 ng/mL (0.0117 μg/mL) of propafenone in plasma. This result coincided with the dose administered; however, it differed from results reported in the literature, even though the clinical response of the patient was favorable with a dose of 2.5 mg/kg/day.
The patient s health improved under the constant medical care by the personnel of the Cardiological Health Care Unit, and monitoring through EKG, reveling a favorable evolution of the patient.
Limitations of case
During clinical surveillance, the patient was maintained in control of the disease that was enough for physician to decide not to ask for therapeutic monitoring of propafenone levels, but if this would be indicated, a strong relationship between levels and therapeutic response.
We concluded that chronic use of propafenone is indicated for patients with SVT secondary to WPW syndrome.
As a temporal solution the use of magistral formulations in pediatric population has to be evaluated in terms of safety and efficacy but in terms of relationship between risk–benefit during prolonged use of propafenone, overall when such relationship will be compared with a spontaneous favorable evolution in the group of patients younger than one year of age diagnosed of WPW syndrome.
This study was supported partially by Abbott Laboratories, specifically for its presentation in the 35th Annual Meeting of American College of Clinical Pharmacology, held in Cambridge (MA), 2006 September 16–19. There is not conflict of interest.
Bibliography
1. Luedtke SA, Kuhn RJ, McCaffrey. Pharmacologic management of supraventricular tachycardias in children. Ann Pharmacother 1997;31:1227–43. [ Links ]
2. Capucci A, Villani GQ, Aschieri D, Piepoli M. Safety of oral propafenone in the conversion of recent onset atrial fibrillation to sinus rhythm: A prospective parallel placebo–controlled multicentre study. Int J Cardiol 1999;68:187–96. [ Links ]
3. Celiker A, Ozer S, Ozme S, Ozkutlu S, et al. Experience with propafenone for the treatment of cardiac arrhythmias in children. Turk J Pediatr 1990;32:85–92. [ Links ]
4. Connolly S, Cynthia L, Winkle A, Harrison D, et al. Propafenone disposition kinetics in cardiac arrhythmia. Clin Pharmacol Ther 1984;36:163–8. [ Links ]
5. Batra AS, Luna CF, Silka MJ. Pharmacologic management of arrhythmias in patients with congenital heart disease. Am J Cardiovasc Drugs 2001 ;1:91 –103. [ Links ]
6. Bink–Boelkens MT. Pharmacologic management of arrhythmias. Pediatr Cardiol 2000;21:508–15. [ Links ]
7. Olguín–uárez H, Flores–Pérez C, Flores–Pérez J, Ramírez–Mendiola B, et al. Bioavailability of an extemporaneous suspension of propafenone made from tablets. Biopharm Drug Dispos 2006;27:241–5. [ Links ]
8. Flores–Pérez C, Juárez–Olguín H, Flores–Pérez J, Ramírez–Mendiola B., et al. A simple method to measure plasma levels of propafenone with fluorescence detection. Chromatographia 2005;62:373–7. [ Links ]
9. Mehvar R, Brocks DR, Vakily M. Impact of stereoselectivity on the pharmacokinetics and pharmacodynamics of antiarrhythmic drugs. Clin Pharmacokin 2002;41:533–58. [ Links ]

