










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkArchivos de cardiología de México
On-line version ISSN 1665-1731Print version ISSN 1405-9940
Arch. Cardiol. Méx. vol.71 n.1 Ciudad de México Jan./Mar. 2001
Revisión de temas cardiológicos
The rational approach to the electrical exploration of the heart
Enfoque racional de la exploración eléctrica del corazón
Alfredo de Micheli, Alberto Aranda, Pedro Iturralde, Gustavo A. Medrano
From the Instituto Nacional de Cardiología "Ignacio Chávez". (INCICH. Juan Badiano No. 1, 14080 México, D.F.)
Aceptado: 18 de septiembre de 2000
Abstract
A rational approach is inevitable in any scientific activity. Such an approach is opposed not only to irrationality, at all inadmissible in scientific thinking, but also to empiric reasoning. Many years ago, Sodi Pallares introduced the rational method in the electrical exploration of the heart based on experimental findings obtained in his laboratory. This method has progressively been accepted and used with good results for diagnoses and has led to logical therapeutic inferences.
To confirm the results from the logical interpretation of electrical tracings, we present some examples of its application in three fields: arrhythmias, myocardial infarction, and left ventricular hypertrophy. In the studied cases -two with tachycardia, one with a posterior infarct, and two with left ventricular hypertrophy- a very satisfactory correlation has been observed between the electrical exploration findings and those obtained through direct examination of the heart.
It is desirable, and even profitable, to analyze in this way the electrical tracings to get as close as possible to reality, rejecting the stereotyped aspects of a simple routine exploration, which often induce errors and lead to some fallacious asseverations.
Key words: Arrhythmias. Myocardial infarction. Left ventricular hypertrophy.
Resumen
Un enfoque racional es ineludible en toda actividad científica. Dicho enfoque se opone no sólo a los irracionales, del todo inadmisibles en el quehacer científico, sino también a los empíricos. Hace años, Sodi Pallares introdujo el método racional en la exploración eléctrica del corazón, con base en hallazgos experimentales obtenidos en su laboratorio. Este método se ha asentado progresivamente en el transcurso del tiempo con buenos resultados en el campo diagnóstico y con lógicas inferencias terapéuticas.
Para comprobar los resultados de la interpretación racional de las curvas eléctricas, presentamos algunos ejemplos de su aplicación en tres campos: arritmias, infarto del miocardio e hipertrofia ventricular izquierda. En los casos estudiados -dos con taquicardia, uno con infarto posterior y dos con hipertrofia del ventrículo izquierdo-se ha observado una correlación muy satisfactoria entre los hallazgos de la exploración eléctrica y los del examen directo del corazón.
Sería deseable, y provechoso, que así se analizaran los trazados eléctricos para acercarse lo más posible a la realidad, rechazando los aspectos estereotipados de una simple exploración rutinaria. A menudo, éstos inducen a errores y a ciertas aseveraciones falaces.
Palabras clave: Arritmias. Infarto miocárdico. Hipertrofia ventricular izquierda.
Introduction
Electrocardiography and vectorcardiography explore the same electric cardiac phenomenon with a different approach: analytical and local for electrocardiography, synthetic and spatial for vectorcardiography. Hence, both constitute essentially a functional exploration. Data provided by them were initially interpreted on the basis of stereotyped patterns; however, some fifty years ago, thanks to the works of Wilson and Sodi Pallares,1 the rational method was introduced to the electrical exploration of the heart, starting to interpret the electrical tracings of cardiac activity as a function of some of the known parameters, i.e., sequence of myocardial depolarization and repolarization, cardiac position and rotation, as well as some hemodynamic aspects, such as volume and work overloads in cardiac chambers. Sodi Pallares called this procedure "deductive electrocardiography".2
The first mentioned parameter has been studied quite satisfactorily in dogs heart, particularly by the group of Sodi Pallares,3 and later on in the isolated and perfused human heart.4 Hence, experimental results could be extrapolated to the live human heart (analogy).
The human heart is somewhat different from that of the dog, for example in the distribution of the Purkinje network, in the anastomosis of coronary arteries, and in the volume of the myocardial mass of the right ventricle.5 Regarding the latter one, the heart of the dog resembles more that of children, which physiologically presents, until the age of six, important electromotive forces of the antero-inferior right septal mass, or that of adults with moderate right ventricular hypertrophy.
Regarding the second parameter, i.e., influence of cardiac position, this is a well established fact based on anatomic-electrocardiographic and electro- radiological correlation works performed at our institute6 and other research centers.7
Physiopathological modifications produced by hemodynamic changes have been demonstrated by the work of Enrique Cabrera8 and his followers.9,10
At any rate, current knowledge on the intimate structure and function of myocardial fibers has been increasing and, therefore, other factors responsible for the electrical manifestations of cardiac activity must be taken into account, such as metabolic aspects. It is indispensable, therefore, to widen the spectrum of the electrical exploration of the heart and continue with the analysis of the data obtained through multiple logic procedures besides the experience gained by direct observation. in fact, a unique conducting thread of scientific thinking has persisted throughout the years: the inevitable requirement of rational foundation.11
It seems of uttermost practical usefulness to remember per summa capita the correct analysis of some electrocardiographic findings in the light of the rational approach of the Mexican School of Electrovectorcardiography.
The rational electrical exploration
Arrhythmias
A tendency to memorize and use stereotyped definitions of certain phenomena is often observed among masters and pupils, instead of penetrating into their intimate essence.
There are quite a few examples of such statements in the field of arrhythmias. it is often talked and written about ventricular tachycardia of "narrow" or "wide" QRS, without realizing the erroneous concept involved in such expressions. The term "narrow" does not correspond to reality since, in these cases, the duration of the ventricular complex is not lower than normal, to the contrary, tends to surpass the one observed in the same individual in the absence of tachycardia, and can even be above the upper normal levels, i.e., being of more than 100 msec. Based on a strict physiological approach, QRS complexes with a duration larger than 100 msec should be defined as "non-aberrant" whereas those of 120 msec or more should be considered "aberrant". What is the cause of such behaviors? They are caused, respectively, by the absence or presence of an extensive "jumping wave"1 phenomenon through the intraseptal barrier,12 a well established fact through experimental and clinical research.13 This concept-together with that of the electrical manifestation of the ventricular overloads- constitutes one of the most original and valuable contributions of the Mexican School of Cardiology.
It is, hence, logic, to speak of tachycardias or ventricular extrasystoles without "jumping wave" when the QRS complexes are not aberrant. in turn, tachycardias or ventricular extrasystoles with "jumping wave" phenomenon should be considered when the QRS complexes are aberrant and resemble those recorded in the presence of advanced degree bundle branch blocks.14 in the first condition, the tachycardia or ventricular extrasystole probably originates in specific fibers or very close to the "intraseptal barrier", i.e., close to the anatomo-functional separation existing between the right and left septal masses, a discontinuity called "ephapsis" by some physiologists.15 But, in the case of non-aberrant ventricular complexes, the arrhythmia could have a supraventricular origin, that is, above the bifurcation of the common His bundle.
Example
Figure 1 corresponds to an orthodromic supraventricular tachycardia, without "jumping wave", with a cycle length of 346 msec = 165 beats/min. The anterograde arm of the circuit is constituted by the atrioventricular node and the retrograde arm by an accessory pathway, of the left Kent bundle-type,witha VA interval of165 msec. The ventricular complexes are non-aberrant, the trace of the last strip, obtained from the tip of the right ventricle, shows signs of injury produced most likely by the catheter-electrode.
Figure 2 provides an example of a left ventricular tachycardia, with a right bundle branch blocktype morphology of the QRS complexes and a frequency of 190 beats/min. The complexes recorded in Di, V6, V1 and the tip of the right ventricle (this last one of polyphasic aspect in the terminal strip) suggest a "jumping wave" phenomenon from left to right through the intraseptal barrier.
Infarcts
Similar considerations of electrophysiological character can be made regarding the so called infarcts with or without Q waves. It is known that the unexcitable region, strictly circumscribed within the limits of the so-called electrical endocardium,16 does not produce direct electrocardiographic manifestations.17 Since the electrical endocardium constitutes an essentially functional entity, the electro-anatomical correlations are not justified to establish the significance of the presence or absence of abnormal Q waves in the leads exploring the affected region. Actually, the morphology of the corresponding ventricular complex depends on the relation existing between the size of the unexcitable region -depth and surface- and the amplitude of the electrical endocardium. To delimit the extension of the latter, it would be necessary to identify histologically the distribution of the Purkinje network or to record the potentials originated in the specific fibers (P potentials) at different levels of the parietal or septal thickness.18 The electrical endocardium reaches the specialized tissue region where P potentials can be recorded. When the excitatory impulses reach that region at the same time through the Purkinje fibers, this region depolarizes simultaneously without originating potential differences. Hence, its activation cannot provide direct signs in neither normal nor pathologic conditions. The extension of the Purkinje network varies from one individual to another, and in the same individual differs at the diverse levels of the free ventricular wall and the interventricular septum, covers approximately 50% of the parietal thickness, in its internal portion, is abundant in the lower half of the ventricles and almost absent in the upper third. under experimental conditions, it can be localized by means of P potential recordings, which was done in experiments performed in dog hearts.
On the other side, it must be considered that the electrocardiographic signs of the unexcitable zone of the diaphragmatic portion of the left ventricle -abnormal Q waves or QS complexes- are not recorded in the low aVF, DII, and DIII leads, when these, due to the horizontal cardiac position, explore the right ventricle.19 The high abdominal leads MD and ME do not capture potential variations from the right ventricle but from the left one in case of vertical, semi-vertical, or intermediate hearts. Therefore, it is necessary to identify always the cardiac position according to the left ventricular morphologies or, if not possible, by means of radiography. It is indispensable to know which structures are being explored by the unipolar leads, of these, only aVR explores usually the right atrium.
Even more, it should not be forgotten that during the acute stage of an infarct, the predominating signs of subepicardial or transmural injury can mask those of the unexcitable region. The latter ones, just as those of ischemia, will be manifested later on once the injury has been gradually reduced.20,21
Several points must be taken into account regarding the actual significance of the negative RS-T displacements in the right precordial leads in the presence of an infarct defined as postero-inferior by the conventional electrocardiogram. They might represent a mirror image of positive RS-T displacements present in opposed regions, that is, of a posterior subepicardial injury. The infarcted area -apparently inferior- can invade even medial and high portions of the posterior or postero-lateral wall of the left ventricle or of both ventricles. This demonstrates the great usefulness of the thoracic circle, which can provide direct information on the actual dimensions and the evolution of the damaged myocardial zone.22 These aspects determine the characteristics of the syndrome.
Example
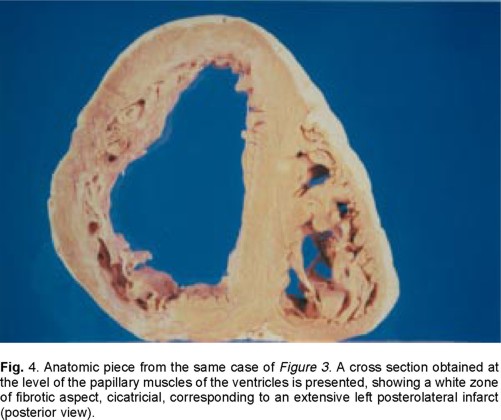
Figure 3 reproduces the electric tracings recorded in a 54 years old man, with an unexcitable myocardium in left postero-lateral regions, left posterior subdivision block (LPSB), and biventricular hypertrophy. The low postero-lateral location of the unexcitable zone is suggested by the start of the ventricular vectorcardiographic curve in the frontal and sagittal planes, which is clockwise and slurred with a 30 msec duration instead of 15 msec. This initial portion is related to the slurred Q wave recorded in aVF (of approx. 50 msec), DIII and V6. Besides, the time of transversal axis (X) crossing in the frontal plane is of 60 msec and that of the anteroposterior one (Z) in the sagittal plane is of 67 msec (normal: around 25 msec, manifestation time of vector lis). The LPSB is diagnosed by the terminal slurring of the ventricular curves, located below, to the left and behind its site of origin, and by the time of onset of the intrinsicoid deflection (TOID) of 80 msec in aVF and V6. The TOID of 60 msec in aVL, with a clean R wave, leads to consider left ventricle hypertrophy, and that of 40 msec in V2 and V3, also with clean R, suggests right ventricle hypertrophy. It must be noted that the lack of left thoracic unipolar V7 to V9 leads does not allow to detect the actual extension of the postero-lateral infarct, which in reality also involves middle-superior regions of the free left ventricular wall. In this case, the anatomic examination (Fig. 4) revealed the presence of an old extensive transmural infarct in the postero-lateral regions of the free left ventricular wall and biventricular hypertrophy with diffuse dilation and myocardial fibrosis.

Ventricular hypertrophies
Several authors state that electrocardiography does not allow to recognize signs of left ventricular hypertrophy, whereas it can be diagnosed through echocardiography. But, it is well known that the electric exploration is of functional type, whereas echocardiographic exploration provides mainly structural data. The first reflects metabolic and electrolytic conditions, as well as certain hemodynamic alterations: overloads of the cardiac chambers. The second reflects structural aspects such as compensating hypertrophy, which in general is due to a sustained systolic overload. In such a case, the electric exploration should provide initial signs of left heart compromise: ventricular overload. Besides, it allows inferring structural data derived from functional data, if a whole constellation of electrocardiographic parameters is taken into account. These must be analyzed selectively in those unipolar leads exploring closely the affected cardiac chamber so as to offer veracious information.23,24 The most valuable electrocardiographic finding consists of the prolongation of TOID, with clean R wave, in the mentioned leads.25 It is obvious to say that TOID reflects the manifestation time of the vector resulting from myocardial activation, which points towards the considered unipolar lead. The magnitude of this vector depends on the duration of the wave fronts originating it. Other data, such as the absence of the manifestation of the right basal vector (IIId) in a dextro-rotated heart without left blocks, are also valuable.
Example
1. The first example refers to a 58 years old man, with long-term systemic arterial hypertension and a dissecting aortic aneurysm, ruptured at the pericardium. The conventional electrocardiogram, taken just before his death (Fig. 5) reveals the following data: Horizontal and levo-rotated hearth with ÂQRSF at -20°. QR complexes in DI, aVL, and V6 (TOID = 50 msec in aVL). S > R from V1 to V3 (TOID = 20 msec in VI, 35 msec in V2 and V3), qRS in V4 and V5 (TOID = 45 msec). Concave negative displacement of the ST segment in aVL, V5 and V6. Chronological (prolongation of TOID in the left unipolar leads) as well as morphological data (low voltage of T wave in those leads) suggest the existence of a global hypertrophy of the left ventricle due to sustained systolic overload. There is also left atrial hypertrophy: P = 0.12 sec in DII. The aspect of the ST segment in aVL, V5 and V6, together with the relative short Q-Tc interval suggests the effects of Digitalis.
The anatomic study (Fig. 6) performed on the next day of the electrocardiogram revealed a concentric hypertrophy of the left ventricle with a 20-mm thickness at the medial portions of the free wall (normal values = 12 mm) and a thickness of 30 mm in the interventricular septum. By the way, it must be mentioned that 800 mL of blood were found in the pericardium. This fact could have cushioned the voltage of the electrical records.
2. The second example corresponds to a 65 years old woman with calcified aortic stenosis. The last electrocardiogram taken (Fig. 7) indicates a semi-horizontal cardiac position with ÂQRSF at -15°. R wave is clean and of high voltage in all left leads. Morphologies of the ventricular complexes are: R in DI, qR in aVL (TOID = 55 msec), rS with deep S in V1 and V2, S > R in V3 (TOID = 15 msec in V1, 30 msec in V2, 35 msec in V3), R > S in V4 and R in V5 and V6 (TOID = 50 msec); QS in aVR. There is a negative displacement of the ST segment in DI, aVL, and from V4 to V6. The T wave is negative with asymmetric branches in DI, DII and from V2 to V6. Q-Tc = VM + 0.04 sec in DI, aVL, V5 and V6. Prolongation of TOID and the high voltage of the R wave in the left leads (63 mm in DI and V6) as well as the negative displacement of the ST segment and the secondary-type inversion of the T wave in these leads suggest the existence of a global hypertrophy of the left ventricle due to sustained systolic overload.
Examination of the anatomic piece (Fig. 8) revealed an increased (25 mm) thickness of the interventricular septum, of the medial portions of the lateral free wall (25 mm) and of the posterior wall (25 mm) of the left ventricle. Hence, there is an important concentric hypertrophy of this ventricle. Its free wall also shows small white colored fibrotic areas. A discrete hypertrophy of the right ventricle can also be observed: thickness of the free wall = 5 mm (normal = 3 mm). Right septo-parietal hypertrophy is manifested in the electrocardiogram by the TOID values in right leads: 30 msec in V2 and 35 msec in V3.



Comment
The semiological value of interpreting rationally and not empirically the electric tracings derives from the aforementioned, as proposed in his time by Sodi Pallares.2 It is desirable that the analysis and interpretation of the electrocardiographic and vectorcardiographic curves be explained and taught in this way. In fact, application of the rational method in this field can provide reliable, complete, and low-cost information. The so called "non-diagnostic tracings" quite often correspond rather to deaf electrocardiographists than to mute electrocardiograms.
Those that deny the diagnostic value of the electrocardiogram, in general, are not concerned with the procedures followed by some authors -based on stereotyped computer programs- to fundament their negative judgment on the diagnostic value of the electrical recordings. This occurs for example in regard to left ventricular hypertrophy. Now is the moment to pose certain questions: How were those electric explorations performed? Have the potential variations of the structures of the left ventricle really been captured? Have the heart position and rotation been taken into account? Indeed, these cause the unipolar leads to explore one or other cardiac structure. Probably conventional electrocardiograms and "indices" were used, which by their same nature cannot reflect the true parameters involved. However, apparently no prospective-type research has been performed to correlate all the available electrocardiographic data with the anatomic data to diagnose the mentioned hypertrophy. The best known studies limit themselves to establish a comparison between the single electrocardiographic data, for example the value of TOID determined exclusively in V6 with echocardiographic findings. At any rate, the electrocardiographic diagnosis in these cases has a rather qualitative character, whereas aimed echocardiographic exploration, for example determination of the myocardial mass of the left ventricle,26 allows to obtain quantitative-type information.
On the other hand, the limitation of the pure deductive method is clear, which can be applied only in the field of eidetic sciences: logic and mathematics, but is not possible to be applied in the field of electrovectorcardiography, since some points regarding the electrical activity of the myocardium are still not fully known, such as the contribution of the posterior ventricular wall in the in situ human heart.
Conclusions
Masters and pupils must discard those purely passive attitudes, improper of noble and inquisitive minds. Lets accept with a critical mind all the information provided, even from the best known cardiology centers, and lets make a personal effort to understand the findings of cardiac electrical exploration using our cerebral neurons. Hence, we would avoid getting crystallized by simple appearances and would achieve a closer relation to the real essence of the phenomena we are studying. It must be kept in mind that the difference between what we call real and appearances lies in the fact that reality is ordered -commanded by laws,27 whereas appearance does not seem to be commanded by any order.
References
1. Sodi Pallares D: New bases of electrocardiography. St. Louis, MO, C. V. Mosby Co, 1956. [ Links ]
2. Sodi Pallares D, Bisteni A, Medrano GA: Electrocardiografía y vectocardiografía deductivas. México. La Prensa Médica Mexicana, 1964, p. VII. [ Links ]
3. Medrano GA, Bisteni A, Brancato RW, Sodi Pallares D: The activation of the interventricular septum in the dog's heart in normal conditions and in bundle branch block. Ann N Y Ac Sci 1957; 65: 804-817. [ Links ]
4. Durrer D, van Dam R Th, Freud GE, Janse MJ, Meijer FL, Arzbaecher RC: Total excitation of the isolated human heart. Circulation 1970; 41: 899-912. [ Links ]
5. de Micheli A: Hacia una electrocardiografía racional. Arch Inst Cardiol Mex 1968; 38(5): 613-615. [ Links ]
6. Zuckhermann R: Consideraciones electropográficas. Arch Inst Cardiol Mex 1947; 17: 533-544. [ Links ]
7. Ashman R: Estimation of heart position from the QRS complex of the electrocardiogram. Arch Inst Cardiol Mex 1964; 16: 139-153. [ Links ]
8. Cabrera E, Monroy JR: Systolic and diastolic loading of the heart. II. Electrocardiographic data. Am Heart J 1952; 43: 669-686. [ Links ]
9. de Micheli A, Medrano GA, Casanova JM: Aspectos eléctricos de las sobrecargas ventriculares experimentales diastólica y mixta. Arch Inst Cardiol Mex 1990; 60: 11-19. [ Links ]
10. de Micheli A, Medrano GA, Casanova JM: Aspectos electrovectocardiográficos de las sobrecargas sistólica y diastólica del ventrículo izquierdo. Arch Inst Cardiol Mex 1990; 60: 127-135. [ Links ]
11. de Michell A: ¿Cuándo nació la ciencia moderna? Arch Inst Cardiol Mex 2000; 70: 513-519. [ Links ]
12. Sodi Pallares D, Bisteni A, Medrano GA, Ginefra P, Portillo B, Del Río R: The "physiological barrier" of the interventricular septum. III World Congress of Cardiology. Brussels, 1958. Abstracts of communications, p. 33. [ Links ]
13. Medrano GA, de Micheli A, Aranda A, Iturralde P: ¿Es aún válido el concepto de salto de onda? Arch Inst Cardiol Mex 2000; 70: 19-29. [ Links ]
14. de Michell A, Medrano GA, Sodi Pallares D: Etude électrovectocardiographique des blocs de branche chez le chien à la lumière duprocessus d'activation ventriculaire. Acta Cardiol 1963; 18: 483-514. [ Links ]
15. Rubio R, Rosenblueth A: La organización funcional de los tejidos ventriculares. Arch Inst Cardiol Mex 1956; 26: 644-663. [ Links ]
16. Sodi Pallares D, Medrano GA, de Micheli A, Testelli M, Bisteni A: Unipolar QS morphology and Purkinje potential of the free left ventricular wall. The concept of electrical endocardium. Circulation 1961: 23: 836-846. [ Links ]
17. Medrano GA, de Micheli A: Electrocardiographic features in experimental subendocardial infarctions in canine hearts. J Electrocardiol 1994; 27(3): 263-273. [ Links ]
18. Medrano GA, Sodi Pallares D, de Micheli A, Bisteni A, Polansky BJ, Hertault J: A study of the potential of the Purkinje tissue. Am Heart J 1960; 60: 562-580. [ Links ]
19. de Micheli A, Medrano GA: El diagnóstico electrovectocardiográfico de zona inactivable miocárdica. Arch Inst Cardiol Mex 1989; 59: 195-210. [ Links ]
20. Sodi Pallares D, Bisteni A, Medrano GA: Acerca de los síndromes de insuficiencia coronaria. Principia Cardiol 1956; 3: 232-262. [ Links ]
21. de Michell A, Medrano GA: ¿Qué debemos entender por isquemia, lesión y necrosis? Arch Inst Cardiol Mex 1994; 64: 205-221. [ Links ]
22. de Micheli A, Medrano GA, Iturralde P: El círculo torácico en la exploración eléctrica del corazón. Arch Inst Cardiol Mex 2000; 70: 187-196. [ Links ]
23. de Micheli A, Medrano GA: Manifestaciones electrovectocardiográficas de los crecimientos ventricular izquierdo y biventricular. Arch Inst Cardiol Mex 1988; 58: 67-77. [ Links ]
24. de Micheli A, Medrano GA: Enfoque electrofisiológico del diagnóstico de crecimiento ventricular izquierdo. Arch Inst Cardiol Mex 1995; 65: 365-374. [ Links ]
25. Maldonado Tapia B, Calderón Colmenero J, de Micheli A, Rijlaarsdam M, Casanova Garcés JM, Attie F, et al: Aspectos electrocardiográficos y ecocardiográficos de la miocardiopatía hipertrófica en edad pediátrica. Arch Inst Cardiol Mex 2000; 70: 247-260. [ Links ]
26. Lorel BH, Carabello BA: Left ventricular hypertrophy. Pathogenesis, detection and prognosis. Circulation 2000; 102(4): 470-479. [ Links ]
27. Monod J: El azar y la necesidad. (Trad. F. Ferrer Larín). Barcelona. Tusquets Ed. 3a edición, 1985: p. 114. [ Links ]

