










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkPapeles de población
On-line version ISSN 2448-7147Print version ISSN 1405-7425
Pap. poblac vol.13 n.53 Toluca Jul./Sep. 2007
Income, income inequality and mortality in metropolitan regions of Brazil: an exploratory approach
Ingresos, desigualdad de ingresos y mortalidad en regiones metropolitanas de Brasil: un acercamiento exploratorio
Mardone Cavalcante França and Neir Antunes Paes
Universidade Federal do Rio Grande do Norte/ Universidade Federal da Paraiba
Abstract
The goal of this study is to perform an empirical verification of the hypotheses of absolute income and income inequality for 16 metropolitan regions of Brazil (MRB), based on data from the Demographic Census of 2000 and vital statistics from 1999-2001 (deaths by age, sex and causes of death). To test the hypotheses, multiple regression models were adjusted for each independent variable and the statistical significance of regression coefficients corresponding to each hypothesis was verified. The results suggest that mean income is the determinant health factor for the population residing in MRB and not income inequality.
Key words: urban health, adult mortality, income inequality, metropolitan regions, Brazil.
Resumen
El objetivo de este estudio es realizar una verificación de las hipótesis de los ingresos absolutos y de la desigualdad de ingresos para 16 regiones metropolitanas de Brasil (RMB), basada en los datos del Censo Demográfico del 2000 y de las estadísticas vitales del trienio 1999-2001 (muertes por edad, sexo y causas de muerte). Para probar las hipótesis se ajustaron modelos de regresión múltiple para cada variable independiente y verificada e significado estadístico de los correspondientes coeficientes de regresión para cada hipótesis probada. Los resultados sugieren que el ingreso medio es un factor determinante de la salud de la población que reside en las RMB y no la desigualdad del ingreso.
Palabras clave: salud urbana, mortalidad adulta, desigualdad de ingresos, regiones metropolitanas, brasil.
Introduction
The relation between socioeconomic status and health has long been controversial, with studies producing discordant results (Wolfson et al., 1999; Wildman, 2001; Wilkinson, 1994; Lynch y Davey, 2002). Socioeconomic status is generally measured by indicators of income, education, occupation, and living conditions, among others, while health is measured by morbidity, mortality and self-declared health status (Wilkinson, 1992; Kaplan et al., 1996; Kennedy et al., 1996). One of the foci of this debate has been the role of income in determining the individual or collective health of the population. The controversy that feeds the interest and scientific production centers around the following questions: Does health generate income? Or does income generate health? The former is usually supported by sociologists and the latter by economists (Lynch et al., 2001; Rodgers, 2002; Preston, 1975; Deaton, 2003).
The wealth of scientific production found in the literature is focused on the negation or corroboration of the hypotheses of absolute income and income inequality. This problem was investigated by Wilkinson in a series of articles with income as a predictive variable of health conditions. He demonstrated that absolute income (mean income) and not income inequality is important in determining the health status of individuals in poor countries (Wilkinson, 1992; Braveman, 2002; Blakely et al., 2003). During the 1990s and the first years of this decade, various studies were published in different parts of the world, correlating income level and income inequality with mortality. The results, for the most part, corroborate the hypothesis of absolute income for poor countries and the hypothesis of income inequality for rich countries (Ghosh y Kulkarni, 2004; Rossi et al., 2000).
Studies on the relation between health and income that focus on metropolitan areas have been performed, mainly in the United States and other high-income countries such as Canada, England and Australia, and demonstrate that the significance of the association between income inequality and mortality cannot be generalized for all countries (Deaton y Lubotsky, 2003; De Vogli et al., 2005). Wilkinson found a correlation of -0.81 between income inequality and life expectancy at birth for 11 industrialized countries (Wilkinson, 1992). In another study in metropolitan areas of the United States with an adult population aged between 15 and 64 years, Lynch (Lynch et al., 1998) found a strong association between indicators of income inequality and mortality, concluding that areas with high income inequality and low mean income showed excess mortality when compared to areas of low inequality and high mean income. In Latin America, studies on the relation between mortality and socioeconomic indicators are scarce, mainly those dealing with adult mortality, despite increased interest in this topic since the 1990 (Drumond y Barros, 1999). A variation in the spatial mortality pattern was verified in the Brazilian state capitals, by comparing proportional mortality for the principal causes of death (Sichieri et al., 1992). In Brazil, alterations in epidemiologic profile are also associated to the aging population and rapid urbanization.
In the 1980s and 1990s the effects of the epidemiologic transition were already being seen, with the increase in diseases associated to the lifestyle of modern metropolises, while deaths from infectious and parasitic diseases declined. In 1930, around 46 per cent of all deaths occurring in Brazilian state capitals were caused by infectious/parasitic diseases, while only 12 per cent were related to diseases of the circulatory system. In 1995, this picture was completely altered, with seven per cent of deaths caused by infectious/parasitic diseases and 33 per cent by circulatory system disorders. In recent decades the metropolitan regions of Brazil (MRB) have been the preferred destination of population migrations from small cities and rural areas, triggering a chaotic growth in the large metropolises and consequently, promoting a process of spatial and residential segregation that has caused peripheral areas to expand vertiginously, giving rise to large numbers of slums and an increase in urban violence (Szwarcwald et al., 1999). Despite the number of studies that have used life expectancy at birth, infant mortality and general mortality as well as specific causes of death among different countries or within a country itself, no definite conclusion has been arrived at to put an end to the controversy over the socioeconomic determinants of health in individuals or communities.
In spite of the importance, there are few studies on the relation between socioeconomic status and health in Brazilian metropolitan populations. The goal of this study was to perform, by means of an ecologic study, an empirical and exploratory verification of the hypotheses of absolute income and income inequality in 16 MRB, in 2000.
Data and sources
The data used in this article come from four basic sources: a) The Information System on Mortality (SIM) of the Ministry of Health, from where information was obtained on deaths by sex, age, area of residence and causes of death (ICD-10), considering mean number of deaths occurring from 1999 to 2001 to calculate adult mortality rates; b) The Brazilian Institute of Geography and Statistics (IBGE), using the Demographic Census of 2000 to obtain the population data necessary to calculate the adult mortality rates of individuals aged 10 to 64 years; c) Regional Accounts of Brazil for per capita GDP values of metropolitan regions and d) The Human Development Atlas of Brazil (ADHB)-2000, elaborated by the United Nations Development Program (UNDP), in partnership with the Institute of Applied Economic Research (IPEA) and IBGE. From ADHB were obtained indicators of life expectancy at birth (both sexes), infant mortality rate (per 1000 live births), per capita family income (in Reais - $R) and Gini's index, all aggregated for the 16 MRB. The quality of the death-related data used to calculate adult mortality can be considered satisfactory, given that the MRBs are highly urbanized areas encompassing state capitals and neighboring municipalities. Reporting in these areas is almost total and the proportion of deaths classified as «of undetermined cause» is at acceptable levels (mean six per cent).
Methods
The following hypotheses were tested: a) the hypothesis of absolute income: «the health status (measured by life expectancy at birth, infant mortality and adult mortality from specific causes) of the population of metropolitan regions of Brazil is associated to absolute income (measured by GDP per capita, per capita family income);» b) the hypothesis of inequality of income: «the health status (measured by life expectancy at birth, infant mortality and adult mortality from specific causes) of the population of metropolitan regions is not associated to unequal income distribution (measured by Gini's index).» Two statistical analysis strategies were used to verify the two hypotheses: first, Pearson's bivariate correlation test was used between indicators of mortality and income. Therefore, correlations were calculated between life expectancy at birth, infant mortality and adult mortality (10 to 64 years) standardized by sex and age for cancer and cardiovascular diseases and the indicators of income, per capita GDP, per capita family income and Gini's index. Second, the adjustment of multiple regression models with life expectancy at birth, the coefficient of infant mortality and adult mortality rates standardized by sex and age for cardiovascular diseases and cancer included in the models as dependent variables and verifiers of the health status of the population. On the other hand, per capita GDP, per capita family income and Gini's index are included as independent variables.
Four multiple regression models were adjusted, one for each dependent variable. The significance of the models was tested by Analysis of Variance (ANOVA) and the regression coefficients correspondent to each of the explanatory variables by student's t-Test.
Results
Descriptive statistics
The 16 MRB considered in this study are composed of 263 municipalities distributed by the five main geographic regions in the country-North, Northeast, Midwest, Southeast and South. Each MRB has the capital of its corresponding state as a nucleus and the remaining municipalities are confined to the contiguous geographic area that makes up its periphery. Figure 1 and Table 1 show respectively, the map of Brazil with the spatial administration of MRBs and the corresponding descriptive statistics. The 16 MRBs, used as analysis units, represent 23.4 per cent of the total population and 42.6 per cent of the urban population, accounting for 28.2 per cent of the country's GDP. There was an average of 170 thousand deaths in individuals aged 10 to 64 years between 1999 and 2001. The total population of MRBs varied from 17.9 million for the São Paulo MR to 709 thousand inhabitants for the Florianópolis MR. Life expectancy at birth ranged from 74.6 years for Florianópolis to 65.2 for the Maceió MR, while infant mortality rate extended from 11.9 to 43.0/1000 live births.
Income inequality, measured by Gini's index, lay between 0.56 and 0.68, while the coefficient of variation in table 1 revealed that population and per capita GDP showed the greatest relative variability with 1 211, seven and 38.5 per cent, respectively. Life expectancy at birth and Gini's index appear as the lowest coefficients of variability, with 2.8 and 9.2 per cent, respectively.
Bivariate correlation
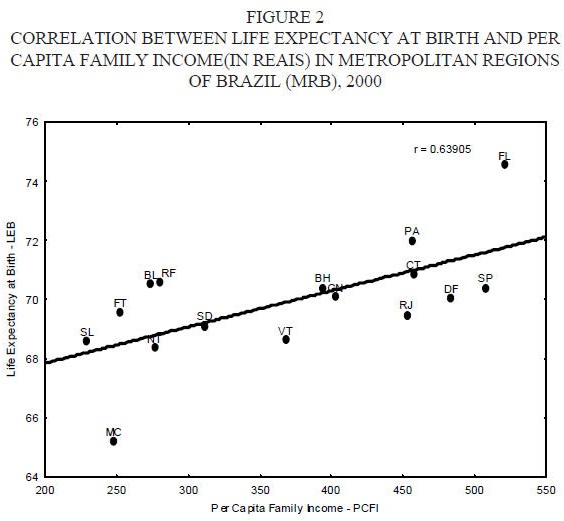
The results of bivariate correlation between the variables, shown on the correlation matrix in table 2, reveals that life expectancy at birth has a positive association r = 0.64, (p = 0.008) with per capita family income, while infant mortality rate correlates inversely with this variable r = -0.84, (p = 0.00). A significant positive correlation was also observed between adult mortality rates for cancer, cardiovascular diseases and log(per capita GDP) and the respective values for correlation coefficient (r = 0.53, p = 0.035 and r = 0.64, p=0.008). No significant correlation was detected with Gini's index for any of the mortality measures used in this study. These results point to a significant correlation between health status and mean income (absolute) of the population with no direct association between health status and income inequality.
Figure 2 shows the dispersion diagram and trend line for the correlation between life expectancy at birth and per capita family income, while Figure 3 depicts the trend lines for the association between adult mortality from cancer and cardiovascular diseases and log(per capita GDP).
Regression models
The results of adjusting regression models 1 and 2 for life expectancy at birth and infant mortality are presented in table 3, with R2 values of 0.45 and 0.75, respectively, showing that only the coefficients of per capita income were significant (p < 0.01) in explaining the variation in life expectancy at birth and infant mortality rate. On the other hand, no statistic significance was found for the regression coefficients associated to Gini's index for the same variables. With respect to models three and four in table 3, which show adult mortality rates for cancer and cardiovascular diseases as dependent variables and log(per capita GDP) and Gini's index as explanatory variables, the coefficient associated to per capita GDP was significant (p < 0.01) for cancer but not for cardiovascular diseases. The regression coefficients associated to Gini's index were not significant (p > 0.05).
Discussion
Brazil is a country of continental dimensions and great social, economic and demographic diversity that has high indices of poverty in its metropolitan areas.
The evidence that this study reveals regarding the absolute income hypothesis confirms the previously known results that in poor countries the income that individuals possess to supply their basic needs is the most important factor in determining the health status of the population and not income inequality, although it is an aggravating factor to be considered (Wilkinson, 1992; Fiscella y Franks, 1997).
The international life expectancy curve versus per capita GDP elaborated by Preston in 1975 and revised by Deaton (Preston, 1975; Deaton, 2003) with data from the year 2000 for more than 100 countries in different stages of development, both in terms of income and epidemiologic transition shows a non-linear relation between these two variables. For the MRBs, however, this relation suggests a linear tendency, as shown in figure 2. In this sense, Brazil's position on the curve stands out, lying exactly on the intermediate part between the almost-vertical segment of poor countries and the beginning of the plateau, where the more developed countries are situated. This finding is consistent with the historical development process of Brazil, which, from the economic point of view, has alternated between periods ofhigh growth and periods of stagnation.
This process has elevated the prevalence of chronic and degenerative diseases concomitantly with the accelerated aging of the population, mainly in metropolitan areas. The wealth of the country is concentrated in these regions, where a large part of the population enjoys a lifestyle that incorporates routine habits that predispose to cancer and cardiovascular diseases, among others, while another part live in poverty and social degradation, subjecting these individuals to infectious/parasitic diseases and all forms of urban violence. It is in this setting, mixed with opulence and poverty, that environmental, microbiological, physical and chemical factors increase the risk of contracting diseases, for both rich and poor (Braveman, 2002; McMichael, 2000).
Since the beginning of the 1990s the Brazilian government has been implementing public income transfer policies for families whose per capita monthly income is less than % of the minimum wage (USD33). In 2004, according to the National Research per Sample of Domiciles (PNAD/2004), government social programs reached 50.3 per cent of households belonging to this income stratum.
In this sense, the corroboration of the absolute income hypothesis, that is, that mean income is an important factor in determining the health status of the population in MRBs, points towards public income transfer policies for the poorest strata of the population that result in an increase of mean family income and consequent improvement in health status.
Although the logic of income transfer policies in Brazil is correct, since they benefit a large number of extremely needy individuals, they leave something to be desired because the values transferred are generally insufficient to be used for health care. In fact, the resources transferred contribute, above all, to meeting basic food needs that ensure survival.
The research data for Brazil as a whole reveal that only 42 per cent of domiciles benefiting from income transfer programs have proper sewage removal; 69 per cent have indoor plumbing and 66 per cent receive trash collection service. These numbers suggest that the mere transfer of money without concomitant investment in infrastructure services that improve the quality of health of the population is not the definite solution to the health question in Brazil, mainly in highly-populated urban areas such as the MRBs.
Conclusion
The results suggest that income inequality is not directly associated with the health of the population that live in the metropolitan regions of Brazil, corroborating many of the studies that point to mean income and not income inequality as the most important for the health of individuals in developing countries. The age-standardized adult mortality rate for cancer yielded Pearson's correlation coefficient of 0.53 (p < 0.035) in table 2 and figure 3, when correlated with the log(per capita GDP), signifying that the higher the per capita GDP, the higher the mortality rates for cancer in the adult population of the MRBs examined in this study. However, no significant correlation was found between adult mortality from cancer and Gini's index. With regard to cardiovascular diseases, table 2 and figure 3 show a correlation coefficient of 0.64 (p = 0.008) but no statistical significance with Gini's index. It is important to point out that these results are, to a certain extent, a result of the epidemiologic transition process in Brazil and consistent with international trends.
Notwithstanding the reservations and criticisms of using aggregate data to test these hypotheses (Gravelle, Wildman y Sutton, 2002) the results found in this study continue to be important, since they broaden information on this question in countries at a similar development stage to that of Brazil, in addition to showing agreement with many experiments that found similar outcomes (Van Doorslaer et al., 1997; Braveman et al, 2002; Blakely et al, 2003; Ghosh et al., 2004).
It is important to point out, however, the need for widening the scope of this study in future investigations. Therefore, the country should be divided into smaller spatial units, using individual data that allow these relationships to be examined in more detail and with more accuracy in order to minimize problems implicit in ecologic studies when testing this type of hypothesis.
Bibliography
BLAKELY, T, J. Atkinson and D. O'Dea, 2003, "No association of income inequality with adult mortality within New Zeland: a multi-nivel study of 1.4 million 25-64 year olds", in J Epidemiol Community Health, 57. [ Links ]
BRAVEMAN, P. and E. Tarimo, 2002, "Social inequalities in health within countries: not only an issue for affluent nations", in Soc Sci Med, 11. [ Links ]
DE VOGLI, R., R. Mistry, Gnesotto and G. Cornia, 2005, "Has the relation between income inequality and expectancy disappeared? Evidence from Italy and top industrialized countries", in J Epidemiol Community Health, 59. [ Links ]
DEATON, A. and D. Lubotsky, 2003, "Mortality, inequality and race in American cities and States", in Soc Sci Med, 56(6). [ Links ]
DEATON, A, 2003, "Health, inequality and economic development", in Journal of Economic Literature, vol XLI. [ Links ]
DRUMOND, Jr. M. and M. Barros, 1999, "Desigualdades socioespaciais na mortalidade do adulto no município de São Paulo", in .Rev Bras Epidemiol, 2(1-2). [ Links ]
FISCELLA, K. and P. Franks, 1997, "Poverty or income inequality as predictor of mortality: longitudinal cohort study", in BMJ, 314. [ Links ]
GHOSH, S. and P. Kulkarni, 2004, "Does the pattern of causes of death vary across socioeconomic classes within a population? An exploratory analysis for India", in Genus, LX, núm.. 2. [ Links ]
GRAVELLE, H., J. Wildman and M. Sutton, 2002, "Income, income inequality and health: what can we from aggregate data?", in Soc Sci Med, 4. [ Links ]
LYNCH, J. and S. Davey, 2002, "Commentary: income inequality and health: the end of the story?", in Int J Epidemiol, 31(3). [ Links ]
LYNCH, J., G. Kaplan, E. Pamuk, 1998, "Income inequality and mortality in metropolitan areas of the United States", in Am J Public Health, 88(7). [ Links ]
KAPLAN, G., E. Pamuk, J. Lynch, R. Cohen, and J. Balfour, 1996, "Inequality in income and mortality in the United States: analysis of mortality and potential pathways", in BMJ, 312(7037). [ Links ]
KENNEDY, B., I. Kawachi and D. Pothrow-Stih, 1996, "Income distribution and mortality: cross sectional ecological study of the Robin Hood index in the United States", in BMJ, 312. [ Links ]
LYNCH, J., S. Harper, G. Smith, N. Ross, M. Wolfson and J. Dunn, 2004, "US regional and national cause-specific mortality and trends in inequality: descriptive findings", in Demographic Research, special colletion 2, article 8. In http://www.demographic-research.gov. Accessed out 14, 2005. [ Links ]
McMICHAEL, A., 2000, "La salud y el entorno urbano en um mundo cada vez más globalizado: problemas para los países em desarrollo", in Bulletin of World Health Organization, 78(9). [ Links ]
PRESTON, S., 1975, "The changing relation between mortality and of economic development", in Popul Stud, 29. [ Links ]
RODGERS, G., 1979, "Income and inequality as determinants of mortality: an international cross-section analysis", in Popul Stud. [ Links ]
ROSS, N., M. Wolfson, J. Dunn, J. Berthelot, G. Kaplan and J. Lynch, 2000, "Income inequality and mortality in Canada and the United States: a cross-sectional assessment using census data and vital statistics" in BMJ, 320. [ Links ]
SICHIERI, R, C. Lolio, V. Correia and J. Everarth, 1992, "Geographical patterns of proportionate mortality for the most common causes of death in Brazil", in Rev saúde púb, 26(6). [ Links ]
SZWARCWALD, C., F. Bastos and C. Andrade, 1999, "Income inequality and homicide rates in Rio de Janeiro, Brazil", in American Journal of Health, 89(6). [ Links ]
TEIXEIRA, C., 2004, "Epidemiological transition, health care model, and social security in Brazil: an analysis of trends and policy options", in Ciênc saúde coletiva, 9, núm.4, in http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232004000400003&lng=en. Accessed June 26, 2005. [ Links ]
VAN DOORSLAER, E, A. Wagstaff, H. Bleichrodt, 1997, "Income related inequalities in health: some international comparisons", in J Health Econ, 16. [ Links ]
WILDMAN, L, 2001, "The impact of income inequality on individual and societal health: absolute income, relative income and statistical artefacts", in Health Econ, 10(4). [ Links ]
WILKINSON, R., 1994, "Divided we fall. The poor pay the price of increased social inequality with their health", in BMJ, 308. [ Links ]
WILKINSON, R., 1992, "Income distribution and life expectancy", in BMJ, 304. [ Links ]
WILKINSON, R., 1992, "National mortality rates: the impact of inequality?", in Am J Public Health, 82. [ Links ]
WOLFSON, M, G. Kaplan, J. Lynch, N. Ross and E. Backlund, 1999, "Relation between income inequality and mortality: empirical demonstration", in BMJ, 319. [ Links ]
Información sobre los autores
Mardone Cavalcante França. Profesor adjunto del Departamento de Estadística de La Universidad Federal de Río Grande del Norte, Brasil. Investigador de la Base de Pesquisa Grupo de Estudos Demográficos. Obtuvo su maestría en Bioestadística en la Universidad de São Paulo-USP-Brasil. Actualmente es doctorando en Ciencias de la Salud por la Universidad Federal de Río Grande del Norte. Sus campos de investigación son: Bioestadística, Demografía de la Salud, Estadística Social y Económica. Docente en Estadística y Demografía. Los trabajos más recientes abordan cuestiones demográficas y sociales de Brasil, tales como: The city as the stage of demographic diversity: the case of the of city Natal, presentado en la XXIV General Conference of the International Union for the Scientific Study of Population Salvador Brazil, 2001; "Socioeconomic conditions as determining factors in the prevalence of systemic and ocular toxoplasmosis in Northeastern Brazil"; (coautor) en la revista Ophthalmic Epidemiology, 2004; Estudo da concentração da posse da terra na região Nordeste e no Estado do Rio Grande do Norte Brasil, Editora da UFRN/EDUFRN, 2006. Correo electrónico: mardonefranca@globo.com
Neir Antunes Paes. Profesor asociado del Departamento de Estadística de la Universidad Federal de Paraíba, Brasil, e investigador del Conselho Nacional de Desenvolvimento Cientifico e Tecnológico (CNPq-Brasil). Posdoctorado en Estudios de la Población por la Johns Hopkins Public School Baltimor y Doctorado en Demografía Médica por la London School of Hygiene and Tropical Medicine de la Universidad de Londres. Sus campos de investigación son: mortalidad, métodos demográficos indirectos y demografía de la salud. Docente de Estadística y Demografía. Ha realizado trabajos recientes sobre la calidad de las estadísticas vitales en el Noreste de Brasil. Entre sus publicaciones recientes están: "Qualidade das estatísticas de óbitos por causas desconhecidas dos Estados brasileiros" en la Revista Public Health Journal, 2007; "Avaliação da cobertura dos registros de óbitos dos estados brasileiros em 2000" en la Revista Public Health Journal, 2005; "Doenças infecciosas e parasitárias no Brasil: uma década de transição", en Revista Panamericana de Salud Pública, OPS, 2004; "Mortalidad por accidente en la vejez en Brasil", en Papeles de Población Núm. 37, 2003 . Correo electrónico: antunes@de.ufpb.br

