











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
The electrocardiogram is a simple and widely available method that provides a good correlation between ST segment elevation at a given location and the artery responsible for the acute ischemic episode.
The simultaneous elevation of the ST segment in the right and lower precordial leads is generally attributed to the presence of multivessel disease that causes extensive myocardial ischemia.1
Uncommonly, ST segment elevation in right precordial leads corresponds to proximal occlusion of the right coronary artery, that is to say, a lower infarct with extension to the right ventricle.1,2
The involvement of the right ventricular free wall occurs in a variable proportion (19-43%) of patients with evidence of lower or posteroinferior myocardial infarction.2 Blanke and et al.3 performed an analysis of patients who presented ST segment elevation myocardial infarction caused by occlusion of the proximal right coronary artery, documenting a presentation frequency with ST segment elevation in precordial V1 lead of 5%; V2 and V3 15%; and V4 with 8%.
The aim of our study is to present a case in which the proximal right coronary artery is responsible for rare electrocardiographic changes in right precordial leads.
Description of the case
This is a 57-year-old male patient who presented a clinical picture of acute coronary ischemic syndrome of 2 hours of evolution, in Killip-Kimball II functional class. The electrocardiogram showed a ST-segment elevation of up to 4mV in leads V1- V3, DII, DIII and aVF, and subendocardial lesion in I and aVL (Figures 1, 2 and 3). Transthoracic echocardiogram with severe hypokinesia of the anteroseptal and inferior wall. The patient underwent primary percutaneous transluminal coronary angioplasty, where the left coronary artery, circumflex and anterior descending artery were observed without stenosis (Figure 4), right coronary artery ectasic and 100% occluded at the proximal third (Figure 5).

Figure 1: Electrocardiogram with electrical axis of QRS at -35o, subepicardial lesion in the anteroseptal (V1-V3) leads, subendocardial lesion in I and aVL, subepicardial lesion in inferior leads (III, aVF).

Figure 2: Electrocardiogram after coronary angioplasty of the right coronary artery showing QS complexes in leads III and aVF and ST segment normalization in V1-V3 leads.

Figure 3: Electrocardiogram at 72 hours of patient admission in which QS complexes and inversion of the T wave in leads III and aVF and waves of subepicardial ischemia of V3-V6 are observed.


Figure 5: Angiographic image of the right coronary artery with total thrombotic obstruction in its proximal portion.
Balloon angioplasty and placement of overlapping (4.0 × 24 mm, 4.0 × 20 mm, 4.5 × 16.0 mm) Everolimus (Promus Element Plus®, Boston Scientific, USA) releasing stents were performed with successful angiographic results (Figure 6).

Discussion
Elevation of the ST Segment in the anterior leads is typically attributed to an anterior descending artery obstruction, while elevation of the ST segment in the lower leads, mainly in DIII, is due to obstruction of the Right coronary artery. The concomitant elevation of the ST Segment in the leads on the anterior and inferior surfaces is attributed to an obstruction of the right coronary artery in its proximal portion and, therefore, is associated with an infarct of the right ventricle. If the ST segment elevation on the lower face is higher in IBD, the affected vessel is likely to be the circumflex artery.4
In some cases, right ventricular infarction coexists with a lower or postero-inferior infarct of the left ventricle. This phenomenon can be explained anatomically by the fact that this occurs in patients with a dominant right coronary circulation, in which the inferior part of the left ventricle and the basal part of the interventricular septum are irrigated by this artery.5,6
When proximal obstruction of a dominant right coronary artery occurs, ST segment elevation in right precordial leads usually follows a decreasing pattern, being more noticeable in V1 and lower in V3-V4. The electrocardiographic evolution in case of infarction shows in these patients an appearance of Q waves in lower leads and a normalization of the ST segment in the previous leads.
The above mentioned electrocardiographic changes can be understood when the Grant method is used for the analysis of the electrocardiogram, starting from the premise that the ST segment can also be represented by a vector and is constituted by several vectors of smaller magnitude.
Since the vectors can have a wide variety of directions, the electric axis must be analyzed in both the frontal and the horizontal (transverse) plane, in order to obtain an electric space axis, the heart is a three-dimensional structure and the electric forces are also directed in three dimensions.
Normal values are considered for the electrical axis of the QRS complex in the frontal plane of -30 to + 90o and in the horizontal plane of 0o to -60o. Under normal conditions the magnitude of the ST segment average vector is small and its direction is relatively parallel to the vectors of the QRS complex (Figures 7 and 8).7

Pozas G. The grant method. Magazine AVANCES. 2012; 27 (9): 18-22. [figure].
Figure 7: Anatomical diagram that exemplifies the frontal plane of the thorax with the derivations and their corresponding degrees.

Pozas G. The grant method. Magazine AVANCES. 2012; 27 (9): 18-22. [Figure].
Figure 8: Anatomical diagram that exemplifies the transverse plane of the thorax with the precordial leads and their corresponding degrees.
When it is considered that the right ventricle is an anterior structure in the anatomical plane, it is easy to understand how an infarct that affects it can manifest characteristics of anteroseptal infarction of the left ventricle in the electrocardiogram.8
These electrocardiographic changes can also be favored because in the right ventricular infarction a progressive dilatation of the cavity can occur, which generates an electric rotation of this one in the horizontal plane, causing the leads V1 to V4 to register the electrical phenomena of the right ventricle.9
The mean ST segment vector has a lower, right and anterior direction when there is an infarct of the right ventricle and a superior direction, to the left and anterior when there is an anteroseptal infarct. It is necessary to emphasize that the ST segment vector always has an anterior direction in both types of infarction.
The mean ST segment vector is generally -30o to -90o counterclockwise in the frontal plane and 10o to 70o in the previous direction when there is an anteroseptal left ventricular infarction, but is higher than + 90o towards left and is directed from 10o to 40o anteriorly, when there is an infarct of the right ventricle associated with a lower left ventricle infarction (Figures 9 and 10), this results in a depression of the ST segment in DI. The postero-anterior direction of the ST segment spatial vector will produce an anterior ST segment elevation from V1 to V3 (even up to V4).10

Hans J. Cardiac anatomy and imaging techniques. 2016; [Figure]. Retrieved from http://www.radiologykey.com
Figure 9: Front view of the chest. The right and bottom arrow represents the mean ST segment vector when a right ventricular infarction is present plus an infarct of the left ventricle. The further to the right this vector is directed, the higher the possibility that the right ventricle is affected. This vector is responsible for the ST depression in DI. The arrow in the left-hand direction represents the ST segment vector when anteroseptal infarction of the left ventricle is present, which usually has a direction of -30o to -90o. RA = Right atrium, LV = Left ventricle.
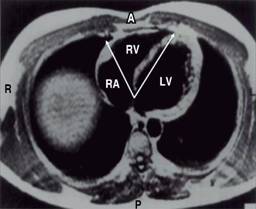
Hurst J. Comments about the electrocardiographic signs of right ventricular infarction. Clin Cardiol. 1998; 21: 289-291. [Image].
Figure 10: Computed tomography image shows that the right ventricle is located in the anterior part. The arrow with anterior and right direction represents the ST Segment vector in case of right ventricular infarction, this results in an elevation of the ST Segment in leads V1-V3 and even V4. The arrow in the left-hand direction and in the same way as in the previous example represents the mean vector of the ST Segment produced by an anteroseptal infarct, note that it will also produce an elevation of the ST Segment in leads V1-V3 and even V4. RV = Right ventricle, RS = Left atrium, LV = Left ventricle.
The right ventricle has some protection against ischemia because of its thin wall with a smaller ventricular mass and a smaller workload. In addition, the right ventricle has a large number of collateral vessels, usually originated in the descending conal arteries, with a greater collateral flow from left to right than in the reverse direction.
However, in view of higher oxygen demands, hypertrophy of the right ventricle increases the risk of heart attack, despite the presence of collateral circulation.11
Regarding the prognosis of these patients, in 2013, the group of Sadanandan and cols. evaluated the significance of combined anterior and inferior ST-segment elevation on the initial electrocardiogram in patients with myocardial infarction and correlated it with the function of the left ventricle and the extent of the infarction. The electrocardiograms were analyzed on the admission of 2,996 patients with acute myocardial infarction belonging to the GUSTO-I angiographic substudy and the GUSTO-IIb angioplasty substudy, who underwent immediate angiography. A total of 1,046 patients with anterior ST-Segment elevation (≥ 2 V1-V4 leads) were identified and divided into 3 groups: group 1, anterior plus inferior ST segment elevation (≥ 2 leads in DII, DIII, aVF, n = 179); group 2, isolated anterior ST elevation or depression of the ST segment (≤ 2 leads in DII, DIII, AVF, n = 447); group 3, anterior ST elevation plus superior ST elevation (ST segment depression in ≥ 2 of leads II, III, aVF, n = 420). Cardiac risk factors, myocardial infarction, angioplasty or prior coronary bypass, Killip score and thrombolytic therapy allocation did not differ between the 3 groups. Patients in group 1 had the highest number of leads with ST segment elevation compared to groups 2 and 3. Despite having a higher number of leads with ST segment elevation, patients in group 1 had a lower peak CPK level and less left ventricular dysfunction. From the above data, it can be concluded that the size of the infarct and left ventricular dysfunction in patients with anterior ST elevation is directly related to the direction of the deviation of the ST Segment in leads DII, DIII, aVF; least with inferior ST elevation, intermediate if there is no ST deviation and maximal with inferior ST depression.12
Conclusion
Electrocardiographic alterations in the antero-septal and inferior leads can be explained by damage to the right ventricle; however, the presence of a very prominent posterior descending artery could explain the left ventricle damage mechanism, which would explain the deviation to the left of the QRS axis on the electrocardiogram. This particular case becomes interesting because of the aforementioned left ventricular affection, without evidence of angiographic lesions of the left coronary artery.
It is necessary to perform an adequate vector analysis of the electrocardiogram in order to understand the changes observed in the case presented, and also to not assume from the first instance that the electrocardiographic manifestations are a consequence of multiple vessel disease.
When acute myocardial infarction is accompanied by ST-segment elevation in precordial leads, right ventricular damage should be considered and confirmed by the use of other invasive and non-invasive methods to establish adequate therapy and optimize patient prognosis.

