











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink1. Introduction
Exposure to ultraviolet radiation (UVR) from the sun is one of the main factors associated with the high incidence of skin cancer worldwide (Leiter et al., 2020). Extended exposure to UVR can also lead to premature skin aging, photo-dermatosis, and damage to hair and the eyes (NRPB, 2002). By contrast, UVR exposure can also benefit vitamin D synthesis to prevent diseases like osteoporosis, type 1 diabetes, some cancers, and immune system dysfunctions (Young, 2006; Ponsonby et al., 2005; Holick, 2004).
However, the negative effects of sun exposure are more concerning. National statistics published by the Ministry of Health in Chile estimate more than 3,451 newly diagnosed cases of non-melanoma skin cancer (NMSC) between 2003-2007, corresponding to an Age-adjusted Incidence Rate (IAT) of 25.4 for men and 19.2 for women. Regarding NMSC, 368 new cases were registered nationally, corresponding to an IAT of 3.0 for men and 2.4 for women over the same period (MSC, 2012). The northern region of Chile is a desert area with a very high incidence of diffused solar radiation. Furthermore, many areas are above 3000 m, which further increases exposure to surface UVR.
The UVR spectrum is divided into three levels for physical and biological reasons, UVA (315 to 400 nm), UVB (280 to 315 nm), and UVC (100 to 280 nm) (ICNIRP, 2004). The amount of UVB reaching surface levels is strongly related to absorption in the ozone layer, while UVA is related to greater atmospheric transmission. Even small amounts of UVB radiation exposure can be harmful to health (Rivas et al., 2009), and UVB levels are especially high in northern Chile (Rivas et al., 2017).
Data on UVR levels are publicly available through the global solar Ultraviolet Index (UVI). The UVI is a dimensionless scale comprising whole numbers between 0 and 11+, and its use is recommended by the World Health Organization (WMO) to indicate possible health risks due to UVR exposure (WMO, 2002). One UVI unit corresponds to 0.025 Wm-2 of UV irradiance, weighted by the photobiological response of erythema (McKinlay and Diffey, 1987) and skin reddening caused by UVR exposure. The WMO recommends publishing UVIs referent to solar noon (SN), which also coincides with the maximum daily UVR level during a clear day.
2. Methods
UVI measurements were taken from 2008 to 2019 with a calibrated YES-UVB-1 broadband biometer (YES, 2006). The equipment is located on the rooftop of the UV solar radiation laboratory at the Department of Physics at the College of Sciences at the University of Tarapacá (UTA in Spanish), in Arica city, Chile (latitude: 18.30ºS, longitude: 70.32ºW, altitude: 25 m). This equipment is part of the UV measurement network for the Chilean Meteorological Agency (DMC) and is run in cooperation with the University of Tarapacá. It is calibrated according to the recommendations of the World Meteorological Organization (WMO).
Arica is a port city located in northern Chile close to the borders with Peru and Bolivia (Fig. 1). The city has a desert climate and homogeneous temperatures. According to the Chilean Meteorological Agency (DMC in Spanish), the average maximum temperature is 27.4ºC, and the average minimum temperature is 13.2ºC. In Arica, the predominant cloud type is marine stratocumulus, characteristic of the southeastern Pacific tropical environment. This region’s very regular climate conditions are characterized by overcast early mornings and cloudless noon and afternoons (Luccini et al., 2011). Despite cloud presence, there is practically no rainfall throughout the year. The annual average accumulated rainfall is around 0.2 mm. The city’s population is approximately 230 000 people, and Arica is a seaside resort that attracts many tourists who participate in water sports.

Fig 1 Map of South America, with the location of Arica shown in bold (red circle). Source: Google Earth.
Erythemal doses (ED) were calculated from UVI measurements using the following formula:
Where 40 is the UVI conversion factor for erythemal irradiance [W/m2]. By definition, each unit of the dimensionless UVI scale represents 25 mW/m2 of erythemal irradiance. Δt is the integrated time interval.
3. Results and discussion
Figure 2 shows the average monthly UVI values measured before and after SN (red), SN ± 1h (green), and SN ± 0.5h (blue) between 2008 and 2019. During the summer, most days are clear, and UVI levels can extend well above the scale limit. UVI > 13 was observed for almost ¼ of all SN measurements in the summer. In other words, there are no safe sun exposure conditions during summer, i.e., UVI lower than moderate scale levels at times close to SN. The maximum monthly average was UVI = 14.4 ± 1.7 in January. Between November and February, about 90% of all UVI levels were higher than UVI>8.

Fig 2 Monthly UVI boxplot for data around SN: ± one hour (green boxes); ± half-an-hour (blue boxes); maximum daily values (red boxes), at Arica (2008-2019). The circles and horizontal lines show the mean and median, respectively. The vertical bars show 5 - 95% of the sample. The small horizontal segments are the maximum and minimum values for the period.
Most UVI measured data were very high or extreme during the spring and fall, corresponding to unhealthy levels. The winter showed more suitable sun exposure conditions. However, even during the winter season, about ¼ of all UVI measurements still showed a high potential for health risks. It should be highlighted that almost 70% of all UVI measurements taken at times close to SN measured between 2008 and 2019 were very high on the scale (Fig. 3). As was noted in previous studies, these UVI values are typical to subtropical latitude regions (de Paula Corrêa and Pires, 2013; Silva et al., 2019). In Arica, hot arid summers are relatively cloudy, while winters are cold and humid with generally clear skies. However, the UVI data showed high values throughout the year. Recent studies show that the protective effect of cloud cover may be insufficient in significantly attenuating UVR in tropical or subtropical regions (de Paula Corrêa et al., 2021). The data show that the registered UVI levels were above the moderate level about 98.4% of the time. It should be noted that the moderate level is the first level of attenuated photoprotection. The data show that people living in this area are exposed to excessive radiation levels throughout the year.
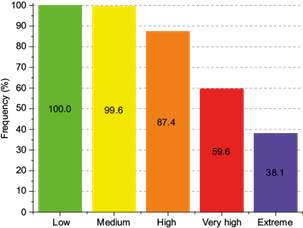
Fig 3 Distribution of accumulated UVI frequencies in Arica between 2008 and 2019, per health risk exposure scale. Risk: a) Low (GREEN): IUV ≤ 2; b) Medium (YELLOW): 3 < IUV < 5; c) High (ORANGE): 6 < IUV < 7; d) Very High (RED): 8 < IUV < 10; and, e) Extreme (VIOLET): IUV ≥ 11.
Figure 4 shows simulations for the accumulated ED around SN under three different conditions: a) integrated doses ± 1 hour around SN, considering the average maximum UVI values observed at that time; b) integrated doses ± 1 hour around SN, considering the average UVI values observed between SN-1h and SN+1h; and, c) integrated doses ± ½ an hour around SN, considering the average UVI values observed between SN-0.5h and SN+0.5h. As expected, the maximum values occur during the summer and can reach ED above 2000 J/m2 after two hours of exposure (between SN-1h and SN+1h). For example, in February, the maximum average dose was 1791±470 J/m2 for maximum UVI around SN. These doses are only slightly lower (1643±418 J/m2) when considering the averages observed between SN±1h. These doses can go above 1000 J/m2 after just one 1 of exposure, as seen via the SN-0.5h and SN+0.5h (992±150 J/m2) integrations.

Fig. 4 Average erythemal doses (ED) between 2008-2019, integrated: a) ± 1 hour around SN, considering the average maximum UVI values observed at that time (RED); b) ± 1 hour around SN, considering the average UVI values observed between SN-1h and SN+1h (BLUE); and, c) ± ½ an hour around SN, considering the average UVI values observed between SN-0.5h and SN+0.5h (GREEN). The vertical bars show the standard deviations.
It is important to note that these values indicate very high ED. UVR availability in Arica may be similar to that observed in Brazil. Corrêa and Pires (2013) showed that ED at summer noon can be enough to cause erythema in higher skin phototypes, results similar to those measured in Arica. On the other hand, the increase in UVI for every degree of latitude toward the equator is around 3.5% (Godar, 2005). This makes it easier to compare our results with studies from the northern hemisphere. Bilbao and de Migue (2020) showed a statistical analysis of UVR measurements performed in Valladolid, Spain (41.7ºN; 4.7ºW; altitude 702 m) between 2013 and 2019. During the summer, mean SN±1h ED is close to 1400 J/m2, with a maximum observed value of around 1870 J/m2. Accumulated doses were lower than those observed in this study. However, Mahé et al. (2011) showed that even in situations of low availability of solar radiation, as in Paris, France (48.0ºN; 2.2ºN, altitude 35 m), the cumulative effect of UVR can be harmful to health.
Another important feature to be noted is the marked seasonality of UVR in Arica. As the region has little cloud cover at solar noon, maximums and minimums are observed in the summer and winter months, respectively. The ED extremes may not coincide with the seasons in locations with significant synoptic systems. For example, monsoons in Southeast Asia can shift the UVR maximum to spring (Tan et al., 2018).
To better understand the order of magnitude for these observed doses, they should be compared with Minimum Erythema Doses (MED). MED is the lowest energy level needed to develop erythema on skin exposed to UVR. For example, individuals with lighter skin and hair, i.e., lower phototypes, require less exposure to UVR for skin reddening to occur after sun exposure. By contrast, individuals with darker skin and hair, i.e., higher phototypes, can withstand higher doses of UVR before presenting skin sensitivity. Table I shows the MED values for different phototypes.
Table I MEDs for phototypes I-VI (adapted from Fitzpatrick et al., 1995)
| Phototype | Skin color | After sun exposure | MED (J/m2) | |
| Burning | Tanning | |||
| I | White | Yes | No | 200 |
| II | Yes | Minimal | 250 | |
| III | Yes | Yes | 300 | |
| IV | No | Yes | 450 | |
| V | Brown | No | Yes | 600 |
| VI | Black | No | Yes | 1000 |
We can see that those doses of just up to 1 hour of sun exposure around SN (SN±0.5h) may be sufficient to cause damage to individuals with darker skin tones (i.e., higher phototypes). During the summer, individuals can receive more than six times the radiation dose after 2 hours of exposure close to SN. Such amounts of UVR can cause erythema in phototype III individuals, i.e., the most common phototype of Chileans (Contreras et al., 2016). Thus, the accumulated ED in Arica is similar to ED in subtropical Brazil within similar latitude ranges. In Brazil, ED between 1700 and 2120 J/m2 was measured between SN±1h (Corrêa et al., 2013), similar to Arica. These were 20 times greater than the UVR daily dose recommended by the main occupational health protection agencies, around 108 Jm-2 per day on unprotected skin (ICNIPR, 2004; ACGIH, 2019; ARPANSA, 2020).
4. Conclusions
In general, meteorological reports and news only disclose maximum daily UVI values related to the SN. However, the effects of UVR exposure are cumulative. For this reason, this study analyzed accumulated ED calculated from SN UVI measurements performed in Arica city, in the far north of Chile, from 2008 to 2019.
87% and 37% of all UV measurements at ±1h SN were above the high-risk and extreme-risk exposure category scale, respectively (WHO, 2002). In the summer, virtually all UVI measurements around SN were within the highest health risk portion of the scale. Even in winter, there was evidence of the need for photoprotection since UVI values varied between medium and high for most measurements.
As expected, ED around solar noon is very high in the region. Accumulated ED up to 1 (SN±0.5h) or 2 hours (SN±1h) was 3 to 6 times higher than the MED to cause erythema in skin types III and IV individuals, i.e., most Chileans living in the region. ED above 2000 J/m2 accumulated in 2 hours around SN were frequently observed during the summertime. Such doses are about 20 times higher than those recommended for healthy sun exposure.
There is an immediate need to review the information contained in weather reports to improve and make them more compatible with everyday exposure levels. Furthermore, the region needs to institute photoprotection educational programs, not only for the city’s permanent residents but also for the tourists who come to the city to participate in leisure and sporting activities.

