











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
In 2019, the WHO estimated that 703,000 people had died from suicide worldwide, accounting for 1.3% of all deaths. The overall suicide rate, standardized by age, was 9.0 per 100,000 population for both sexes, and higher in men (12.6 per 100,000) than women (5.4 per 100,000). Globally, suicide is one of the leading causes of mortality, which is why the WHO considers it a serious public health problem (World Health Organization [WHO], 2021).
One of the groups at the greatest risk of suicide is young people ages 15 to 29. In 2019, 22.8% of suicides occurred in this age group, making it the fourth leading cause of death, after traffic accidents, tuberculosis, and interpersonal violence. In women and men, respectively, suicide was the third and fourth leading cause of death among young people worldwide (WHO, 2020; 2021).
Suicide is preventable, as borne out by the fact that suicide mortality rates have declined in various countries. Between 2000 and 2019, the global suicide rate decreased by 36%, with reductions ranging from 17% in the Eastern Mediterranean Region to 47% in the European Region and 49% in the Western Pacific Region. The only region where an increase in suicide rates was observed was the Americas, where they rose by 17% (WHO, 2021).
In 2019, suicides were one of the leading causes of death from injury in Latin America. Between 1990 and 2019, the number of deaths from suicide increased significantly in most countries in the region. The greatest growth occurred in Paraguay (268.2%), Ecuador (244.9%), and Mexico (188.9%; Dávila-Cervantes, 2022).
In Mexico, various authors have observed a significant increase in suicide in recent decades. Between 1990 and 2000, suicide in young people ages 15 to 24 increased by 74%. Already one of the most severely affected populations, this group accounted for 28% of all suicides in 2007 (Borges et al., 2009). From 1970 to 2007, suicide rose by 275%, particularly among those ages 15 to 29, becoming one of the leading causes of death in this age group (Borges, Orozco, Benjet, & Medina-Mora, 2010).
Between 1970 and 2016, the suicide mortality rate in young people almost quintupled, rising from 1.13% in 1970, through 2.63% in 1990, to 5.2% in 2016. In the population ages 15 to 29, it was the third leading cause of death in both sexes and one of the main causes of years of life lost due to premature death (Dávila-Cervantes, 2019). Between 1990 and 2017, the suicide burden in Mexico rose mainly in young men and women, although the increase in older adults poses an additional challenge for health services.
A study analyzing conventional and gray literature on suicidal behavior in the Mexican population ages 15 to 29 between 1980 and 2014 found that the majority of documents reported risk factors, and that only a small percentage (9.37%) explored protective factors, which is why it is important to explore youth suicide from a public health perspective (Vázquez-Vega, Piña-Pozas, González-Forteza, Jiménez-Tapia, & Mondragón-Barrios, 2015).
In short, in 2020, suicide was the third leading cause of death in Mexico in young people ages 15 to 29, accounting for 43.0% of the total number of suicides reported (Bravo-García, 2022), making it a major public health issue. The objectives of the present study were to explore the changes in the geographical distribution of suicide rates by state, and to analyze the magnitude, distribution, and pattern of suicide mortality rates in Mexican youth ages 15 to 29 between 1990 and 2020.
METHOD
Design of the study
Descriptive, ecological, time-series study on suicide in Mexican youth from 1990 to 2020.
Participants/sample description
Young people ages 15 to 29 who died by suicide from 1990 to 2020, primarily resident in Mexico. This period was chosen because of the availability of official information on deaths registered in Mexico, whose annual databases can be downloaded from the INEGI website (Instituto Nacional de Estadística y Geografía[INEGI], 2022a). Deaths by suicide in the period 1990-1997 were identified using codes E950-E959 of the 9th revision of the International Classification of Diseases (ICD; Pan American Health Organization[PAHO], 1975). As of 1998, when the 10th revision of the ICD began to be used in Mexico, they were identified with codes X60-X84 (PAHO, 1995).
Measurements
The following variables were included: sex (biological sex of the person who died); age number of years completed between birth and date of death); state of residence (state where the deceased resided permanently during their last six months).
Procedure
The official population estimates compiled by CONAPO (Consejo Nacional de Población, 2012) were used to calculate standardized suicide mortality rates, taking the number of suicide deaths in young people ages 15 to 29 years as a numerator and the population corresponding to this age range, multiplied by 100,000, as a denominator. Standardization was conducted using the direct method, using the age and sex structure of the 2005 Population and Housing Count of INEGI as the reference population, since this was the survey taken closest to the midpoint of the period studied (INEGI, 2008). The evolution of national mortality and its disaggregation by sex and state were described.
Statistical analysis
The Joinpoint segmented regression model was used for the time analysis of suicide mortality. Based on a log-linear model, it identifies the points where the direction or magnitude of the trend changes significantly, to determine whether a multisegmented line is statistically more useful for describing the time evolution of a set of data than a straight or less segmented line (Kim, Luo, Kim, Chen, & Feuer, 2014; Kim, Fay, Feuer, & Midthune, 2000). This model makes it possible to detect the points where significant changes occur in mortality trends (in other words, whether they remain stable, or increase or decrease) and also estimates the APC and AAPC (Annual Percentage Change and Average Annual Percentage Change) for each segment of the linear regression and the entire time series respectively as well as their 95% confidence intervals and level of significance (Torres-Sánchez, Rojas-Martínez, Escamilla-Núñez, de la Vara-Salazar, & Lazcano-Ponce, 2014). To select the model with the best data fit, the method using the sequence of permutation tests was used to guarantee that the approximate likelihood of a Type I error would be less than .05. This method involves conducting several tests to choose the number of points of union, using the Bonferroni correction for multiple tests (Kim et al., 2000). The analyses were conducted using Joinpoint v. 4.5.0.1 regression software (National Cancer Institute, 2016). For its graphic representation, the same mortality scale was used (with a rate of 0 to 15 deaths per sex and 0 to 25 deaths per 100,00 for the states).
To prepare the thematic maps of suicide mortality rates, the period of study from 1990 to 2020 was divided into six five-year periods, except for the first period covering six years. Mortality rates were grouped into four categories, using the quartiles of the distribution of suicide mortality in the states during the last five-year period (2016-2020) as criteria, so that the most recent five-year period served as a benchmark: low mortality (.0-6.5 per 100,000 population); average mortality (6.6-8.8 per 100,000 population); high mortality (8.9-11.3 per 100,000 population); and very high mortality (for states with mortality rates of 11.4 or more per 100,000 population). Using this uniform criterion in the six periods made it possible to observe how the geographical distribution of suicide mortality rates in young people changes over time. It was therefore possible to visualize the evolution of suicide mortality in young people ages 15 and 29 in every state in the country using the QGIS mapmaking software version 3.4 (QGIS Developer Team, 2019).
Ethical considerations
This study did not involve intervention in human subjects, since the analysis was conducted using freely accessible secondary information sources, which do not contain personal or confidential data that must be protected. It therefore does not need to be approved by an Ethics Committee.
RESULTS
From 1990 to 2020, 58,928 suicides were recorded in Mexico in young people ages 15-29 (82.2% males and 17.8% females), accounting for 43.0% of the total suicides in the country. The standardized suicide mortality rate tripled during this period, rising from 3.2 to 9.6 suicides per 100,000 young people ages 15 to 29, equivalent to a 198% increase. In general, the risk of dying by suicide is three times higher in men than in women. However, the mortality rate increased at a faster rate in women (285%) than men (178%). Suicide mortality in young women rose from 1.1 to 4.4 per 100,000 population, whereas in men it increased from 5.3 to 14.7 per 100,000 population (Table 1).
Table 1 Suicide mortality rates in young people ages 15 to 29, by sex and year of registration. Mexico, 1990-2020
| Young people ages 15 to 29 | Males ages 15 to 29 | Females ages 15 to 29 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Year | Total suicide deaths |
Number
of deaths |
Standardized Mortality Rate * |
Number
of deaths |
Standardized Mortality Rate * |
Number
of deaths |
Standardized Mortality Rate * | ||
| 1990 | 1,914 | 836 | 3.2 | 687 | 5.3 | 149 | 1.1 | ||
| 1991 | 2,091 | 946 | 3.7 | 791 | 6.3 | 155 | 1.2 | ||
| 1992 | 2,225 | 991 | 3.7 | 825 | 6.1 | 166 | 1.2 | ||
| 1993 | 2,316 | 995 | 3.6 | 839 | 6.1 | 156 | 1.1 | ||
| 1994 | 2,557 | 1,129 | 4.1 | 920 | 6.6 | 209 | 1.5 | ||
| 1995 | 2,849 | 1,336 | 4.8 | 1,093 | 7.7 | 243 | 1.7 | ||
| 1996 | 2,979 | 1,392 | 4.9 | 1,116 | 7.9 | 276 | 1.9 | ||
| 1997 | 3,328 | 1,659 | 5.8 | 1,334 | 9.3 | 325 | 2.3 | ||
| 1998 | 3,282 | 1,600 | 5.6 | 1,303 | 9.1 | 297 | 2.1 | ||
| 1999 | 3,300 | 1,606 | 5.6 | 1,338 | 9.3 | 268 | 1.9 | ||
| 2000 | 3,440 | 1,621 | 5.6 | 1,330 | 9.2 | 291 | 2.0 | ||
| 2001 | 3,760 | 1,692 | 5.8 | 1,358 | 9.4 | 334 | 2.3 | ||
| 2002 | 3,826 | 1,723 | 5.9 | 1,399 | 9.6 | 324 | 2.2 | ||
| 2003 | 4,070 | 1,794 | 6.1 | 1,445 | 9.9 | 349 | 2.4 | ||
| 2004 | 4,061 | 1,750 | 5.9 | 1,426 | 9.7 | 324 | 2.2 | ||
| 2005 | 4,273 | 1,826 | 6.1 | 1,460 | 9.9 | 366 | 2.4 | ||
| 2006 | 4,230 | 1,774 | 5.9 | 1,417 | 9.6 | 357 | 2.4 | ||
| 2007 | 4,362 | 1,796 | 6.0 | 1,428 | 9.6 | 368 | 2.4 | ||
| 2008 | 4,638 | 1,920 | 6.3 | 1,499 | 9.9 | 421 | 2.8 | ||
| 2009 | 5,147 | 2,075 | 6.8 | 1,588 | 10.4 | 487 | 3.2 | ||
| 2010 | 4,960 | 2,052 | 6.7 | 1,595 | 10.7 | 457 | 3.0 | ||
| 2011 | 5,662 | 2,489 | 8.1 | 1,903 | 12.6 | 586 | 3.8 | ||
| 2012 | 5,503 | 2,363 | 7.6 | 1,841 | 12.1 | 522 | 3.3 | ||
| 2013 | 5,838 | 2,398 | 7.7 | 1,873 | 12.1 | 525 | 3.3 | ||
| 2014 | 6,270 | 2,530 | 8.0 | 1,964 | 12.6 | 566 | 3.6 | ||
| 2015 | 6,354 | 2,657 | 8.4 | 2,016 | 12.8 | 641 | 4.0 | ||
| 2016 | 6,292 | 2,618 | 8.2 | 2,072 | 13.0 | 546 | 3.4 | ||
| 2017 | 6,426 | 2,676 | 8.3 | 2,108 | 13.2 | 568 | 3.6 | ||
| 2018 | 6,443 | 2,628 | 8.2 | 2,055 | 12.8 | 573 | 3.6 | ||
| 2019 | 7,018 | 2,916 | 8.9 | 2,289 | 13.8 | 627 | 3.9 | ||
| 2020 | 7,699 | 3,140 | 9.6 | 2,442 | 14.7 | 698 | 4.4 | ||
| Total | 137,113 | 58,928 | 46,754 | 12,174 | |||||
Source: Compiled by the authors based on (Instituto Nacional de Estadística y Geografía, 2022a).
Note: Only deaths of young people with known sex and age, who mainly resided in Mexican s tates, were included.
*Standardized mortality rate per 100,000 young people ages 15 to 29.
Using the most recent five-year period as a starting point, the states with the highest annual standardized suicide mortality rates in young people between 2016 and 2020 were Chihuahua (18.5 suicides/100,000 young people), Aguascalientes (16.6/100,000), Yucatán (14.4/100,000), Guanajuato (14.1/100,000), and San Luis Potosí (12.9/100,000). These five states accounted for 23.0% of the total suicide deaths in young people. Conversely, Guerrero, Veracruz, Sinaloa, Tamaulipas, and Hidalgo had annual mortality rates of 6.0 per 100,000 population or less, well below the national mortality rate, and accounting for just 9.0% of total suicides. There is enormous heterogeneity among the country’s states, since suicide mortality rates are six times higher in Chihuahua than Guerrero (Table 2).
Table 2 Suicide mortality rates in young people ages 15 to 29 and their most recent trend, by state. Mexico, 1990-2020
| Period 2016-2020 | Period 1990-2020 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| States |
State
deaths by suicide |
% | Mortality rate & |
Na-
tional ranking |
Number of
segments |
Last
segment |
Years
of last segment |
APC # |
Trend
of last segment |
|
| Aguascalientes | 302 | 2.2 | 16.6 | 2 | 1 | 1990-2020 | 31 | 6.73* | Upward | |
| Baja California | 295 | 2.1 | 6.2 | 27 | 4 | 2018-2020 | 3 | -27.05 | Downward | |
| Baja California Sur | 93 | .7 | 8.1 | 19 | 1 | 1990-2020 | 31 | -.13* | Downward | |
| Campeche | 148 | 1.1 | 11.5 | 8 | 2 | 1990-2020 | 31 | .07 | Stable | |
| Coahuila | 478 | 3.4 | 12.2 | 6 | 2 | 1998-2020 | 23 | 2.48* | Upward | |
| Colima | 93 | .7 | 9.1 | 15 | 1 | 1990-2020 | 31 | 1.07* | Upward | |
| Chiapas | 504 | 3.6 | 6.5 | 24 | 2 | 2016-2020 | 5 | -15.30* | Downward | |
| Chihuahua | 889 | 6.4 | 18.5 | 1 | 3 | 2008-2020 | 13 | 7.36* | Upward | |
| Ciudad de México | 661 | 4.7 | 6.5 | 25 | 5 | 2018-2020 | 3 | 27.39 | Upward | |
| Durango | 255 | 1.8 | 10.8 | 12 | 5 | 2012-2020 | 9 | 6.56* | Upward | |
| Guanajuato | 1,126 | 8.1 | 14.1 | 4 | 4 | 2015-2020 | 6 | -1.85* | Downward | |
| Guerrero | 161 | 1.2 | 3.2 | 32 | 1 | 1990-2020 | 31 | .97 | Stable | |
| Hidalgo | 222 | 1.6 | 6.0 | 28 | 4 | 2011-2020 | 10 | -.26 | Stable | |
| Jalisco | 1,198 | 8.6 | 11.3 | 9 | 4 | 2011-2020 | 10 | 1.96* | Upward | |
| México | 1,579 | 11.3 | 7.1 | 23 | 3 | 2018-2020 | 3 | 23.25 | Upward | |
| Michoacán | 536 | 3.8 | 8.7 | 17 | 3 | 2017-2020 | 4 | 26.45* | Upward | |
| Morelos | 200 | 1.4 | 7.9 | 20 | 1 | 1990-2020 | 31 | 3.29* | Upward | |
| Nayarit | 137 | 1.0 | 8.6 | 18 | 1 | 1990-2020 | 31 | 3.26* | Upward | |
| Nuevo León | 609 | 4.4 | 9.3 | 14 | 2 | 2006-2020 | 15 | 1.16 | Stable | |
| Oaxaca | 337 | 2.4 | 6.3 | 26 | 3 | 2017-2020 | 4 | 21.52 | Upward | |
| Puebla | 762 | 5.5 | 9.0 | 16 | 1 | 1990-2020 | 31 | 5.01* | Upward | |
| Querétaro | 307 | 2.2 | 11.2 | 11 | 1 | 1990-2020 | 31 | 4.26* | Upward | |
| Quintana Roo | 285 | 2.0 | 12.1 | 7 | 1 | 1990-2020 | 31 | 1.79* | Upward | |
| San Luis Potosí | 479 | 3.4 | 12.9 | 5 | 1 | 1990-2020 | 31 | 3.51* | Upward | |
| Sinaloa | 182 | 1.3 | 4.6 | 30 | 1 | 1990-2020 | 31 | 1.15* | Upward | |
| Sonora | 441 | 3.2 | 11.3 | 10 | 3 | 2010-2020 | 11 | 4.92* | Upward | |
| Tabasco | 248 | 1.8 | 7.7 | 21 | 2 | 2011-2020 | 10 | -6.57 | Downward | |
| Tamaulipas | 236 | 1.7 | 5.2 | 29 | 1 | 1990-2020 | 31 | .28 | Stable | |
| Tlaxcala | 126 | .9 | 7.4 | 22 | 1 | 1990-2020 | 31 | 4.63* | Upward | |
| Veracruz | 456 | 3.3 | 4.3 | 31 | 1 | 1990-2020 | 31 | .90* | Upward | |
| Yucatán | 415 | 3.0 | 14.4 | 3 | 3 | 2014-2020 | 7 | 8.09* | Upward | |
| Zacatecas | 218 | 1.6 | 10.3 | 13 | 1 | 1990-2020 | 31 | 3.10* | Upward | |
| National | 13,978 | 100.0 | 8.7 | 6 | 2018-2020 | 3 | 7.21 * | Upward | ||
Source: Compiled by the authors based on (Instituto Nacional de Estadística y Geografía, 2022b; H.J. Kim et al., 2000).
&Standardized mortality rate per 100,000 young people ages 15 to 29.
#APC = Annual Percentage Change.
*The annual percentage change (APC) is significantly different from zero in alpha = .05
An exploratory analysis made it possible to visualize the evolution of suicide mortality in young people through five-year thematic maps of mortality, except for the first period covering six years. Between 1990 and 1995, only Campeche and Tabasco had high or very high mortality, while the remaining 30 states had medium or low mortality rates. From 1996 to 2000, mortality rates were very high in Campeche; and high in Baja California Sur, Chihuahua, Tabasco, and Yucatán, while the remaining 27 states had medium or low mortality rates. From 2001 to 2005, very high mortality rates were reported in Campeche and Tabasco, together with high mortality rates in Baja California Sur, Chihuahua, Sonora, and Yucatán, while the remaining 26 states had medium or low mortality. From 2006 to 2010, there were already four states with high or very high mortality. Between 2011 and 2015, 13 states in the country had a high (seven states) or very high (six states) suicide mortality rate. And in the most recent period, from 2016 to 2020, eight states recorded very high mortality; eight states, high mortality; seven states, average mortality; and nine states, low mortality rates. In short, the visual representation reflects the evolution of suicide mortality rates in young people, with the most recent period showing that suicide mortality rates in young people in half the country are high or very high. The states with very high suicide mortality rates are located in the center and north of the country, as well as the Yucatán Peninsula (Figure 1).

The regression model showed six time segments in suicide mortality rates in young people, all of which increased. The first was from 1990 to 1993 (APC = 3.49); the second from 1993 to 1997 (APC = 10.65); the third from 2007 to 2008 (APC = .88); the fourth, from 1998 to 2011 (APC = 7.82); the fifth from 2011 to 2018 (APC = 1.12); and the sixth from 2018 to 2020 (APC = 7.21). The analysis of mortality rates throughout the period showed a significant upward trend (AAPC = 3.6; 95% CI [2.4, 4.7] p < .001), reflecting the increase from 3.2 to 9.6 deaths/100,000 young people between 1990 and 2020 (Figure 2).
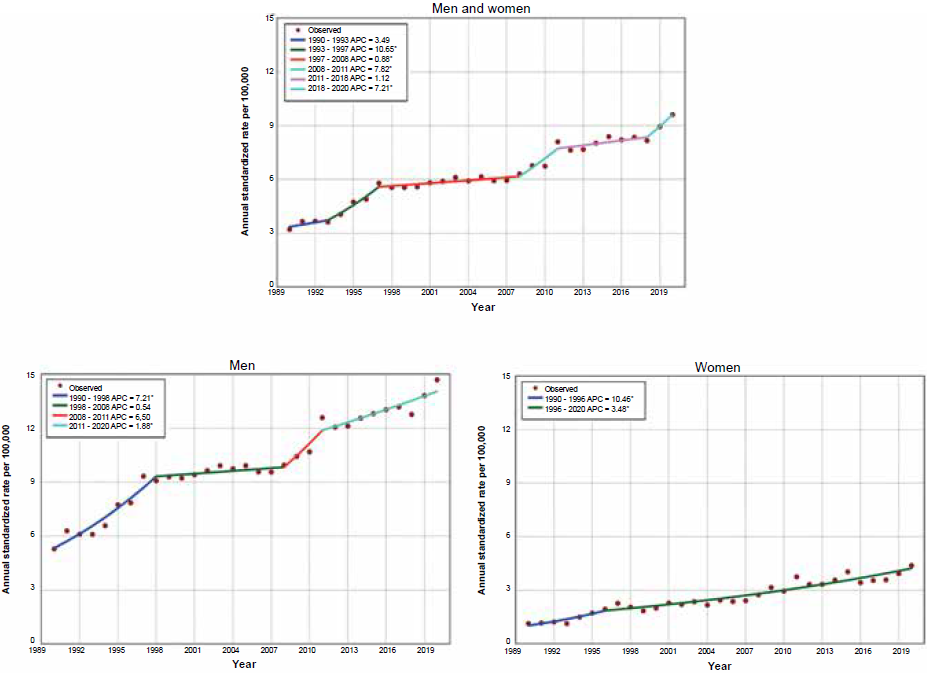
Figure 2 Standardized annual mortality from suicide in young people 15-24 years old, by sex. Mexico, 1990-2020.The annual percentage change (APC) is significantly different from zero at alpha = .05.
The evolution of suicide mortality rates in young men had four-time segments: the first displayed an upward trend from 1990 to 1998 (APC = 7.21); the second showed stable behavior from 1998 to 2008 (APC = .54); the third rose from 2008 to 2011 (APC = 6.50) while the fourth also increased from 2011 to 2020 (APC = 1.88). In women, the evolution of suicide mortality rates contained only two segments, both of which increased, from 1990 to 1996 (APC = 10.46) and from 1996 to 2020 (APC = 3.48; Figure 1). The time analysis of the entire period (1990 to 2020) showed an upward trend in both sexes, with a greater increase in women (AAPC = 4.8; 95% CI [3.5, 6.2] p < .001), than in men (AAPC = 3.3; 95% CI [2.1, 4.5] p < .001).
In addition to the number of deaths and the risk of dying by suicide, the most recent trend in suicide mortality was analyzed within the period 1990-2020. Suicide mortality in young people increased in 22 of the 32 states in Mexico. It decreased in five whereas in the remaining five states, it remained stable (Table 2). The highest annual growth rate corresponded to Michoacán (26.45), followed by Yucatán (APC = 8.09), Chihuahua (APC = 7.36), Aguascalientes (APC = 6.73), Durango (APC = 6.56), and Puebla (APC = 5.01). Mexico City (APC = 27.39), the state of Mexico (APC = 23.25), and Oaxaca (APC = 21.52) displayed significant increases that were not statistically significant.
Conversely, Chiapas recorded a significant decrease in mortality (APC = -15.30), followed by Guanajuato (APC = 1.85) and Baja California Sur (-.13). For their part, Baja California and Tabasco experienced significant decreases (APC = -27.05 and -6.57) respectively, which were statistically significant (Table 2 and Figure 3).

DISCUSSION AND CONCLUSION
WHO data show that, between 1995 and 2019, suicide mortality rates decreased in all the world regions, except for the Region of the Americas, where they increased by 17% (WHO, 2021). During that same period, suicide increased by 188.9% in Mexico (Dávila-Cervantes, 2022). Our study showed that, among young people ages 15 to 29, this increase was greater, amounting to 198%. Globally, suicide in young people accounted for 22.8% of total suicide deaths (WHO, 2020), while the data presented here show that in Mexico, this proportion is 43.0%.
This study shows that suicide mortality in young people has grown steadily for over three decades (1990-2020), which is consistent with the upward trends reported by previous studies analyzing other shorter time periods (Borges et al., 2009; 2010; Dávila-Cervantes, 2019). The regression analysis in this study showed average annual growth in suicide mortality rates in young people of 3.6%, with a greater increase in women (4.8%) than men (4.3%). The rise in all forms of violence against women, which rose from 66.1% to 70.1% between 2016 and 2021, may be a key factor in the more rapid increase in youth suicide among girls and women (INEG, 2022b). The aspect of greatest concern, however, is that there is no indication of a reduction in mortality in any period. Some authors suggest that the sustained growth of youth suicide in recent decades is related to growing economic and social deterioration, school dropouts, difficulty finding jobs, and low salary levels (Hernández-Bringas & Flores-Arenales, 2011) while others consider that it is associated with marital status, underemployment, high alcohol consumption and having family members who died by suicide or suffered mental disorders (Dávila-Cervantes, Torres, & Casique, 2015). The fact is that a great deal of research is required to demonstrate rather than just state the main causes of this increase.
This study updates the geographic distribution, at the state level, of suicide mortality rates in young people, presented in previous studies (Borges et al., 2010). The main contribution, however, consists of the presentation of epidemiological trends and mortality maps in the 32 states in Mexico, showing which states should be prioritized for suicide prevention in young people, depending on their magnitude and epidemiological trends.
Since 2020, the first year of the COVID-19 pandemic, was included in the analysis, it is important to note that a study of 33 middle- and high-income countries or regions in the first 9 to 15 months of the pandemic found no evidence in most of them of a higher number of suicides than expected (Pirkis et al., 2022). In Mexico City, an overall increase in suicides was reported during the first nine months of the COVID-19 pandemic (Borges et al., 2022). And although this study also reports an increase in suicide rates for young people in Mexico City during the period 2018-2020, the result was not statistically significant. It is therefore not yet possible to draw conclusions about the impact of the COVID-19 pandemic on the suicide rate. Future research with information on the most critical years of the COVID-19 pandemic (2020-2022), will undoubtedly allow solid conclusions to be drawn.
Finally, it is important to note that, to date, youth suicide has not been a priority of the federal government as a public health problem, since it continues to grow at an alarming rate, seriously affecting young people ages 15 to 29, who represent the future of the country. Unless action is taken soon, suicide will continue to increase in the coming years.
This situation could change, due to the recent publication of the first National Suicide Prevention Program in Mexico, promoted by the federal Ministry of Health. Its implementation could help modify the growing trend of suicide in Mexico, by “implementing prevention, care and monitoring actions for suicidal behavior at the sectoral level to reduce mortality from this cause, through evidence-based clinical and community strategies” (Secretaría Técnica del Consejo Nacional de Salud Mental, 2022). It could also mitigate the damage to the families and communities affected. Unfortunately, the program lacks explicit goals and fails to define the priority population groups or geographic areas, which will hamper its management and evaluation.
The study of mortality rate trends presented in this study could contribute to the management of a national strategy for the prevention of suicide in young Mexicans, providing support for public health decision making, such as the identification of federal states. and regions of the country that should be prioritized.
Because it is a descriptive study, its main limitation is that it does not explain the causes associated with the total, differentiated increase in suicide mortality rates in young Mexicans. Future research could answer these questions. A second limitation is the under-reporting of deaths due to suicide, related to the stigma associated with this type of death, the limited functioning of the medical or judicial registration systems regarding the cause of death and the “incorrect completion” of death certificates (Sánchez-Cervantes, Serrano-González, & Márquez-Caraveo, 2015).

