











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
The period of transition to fatherhood is marked by significant changes that constitute a source of stress for men. These are often accompanied by depression, psychological distress, and anxiety (Glasser & Lerner-Geva, 2019; Philpott, Leahy-Warren, FitzGerald, & Savage, 2017; Chhabra, McDermott, & Li, 2020). The study of paternal perinatal mental health, which begins when a man’s partner becomes pregnant and lasts through the first year after birth, has received much less attention than that of mothers (Chhabra et al., 2020).
There is ample evidence that perinatal depression and anxiety in mothers have negative consequences on the family, the fetus, and the baby (Falah-Hassani, Shiri, & Dennis, 2017). Likewise, maladaptive responses in perinatal fathers have an impact on the family and the development of the infant (Chhabra et al., 2020; McCoy, 2012; Giallo, Cooklin, Wade, D’Esposito, & Nicholson, 2014). The study of paternal mental health is therefore very much needed as a first step to prevent its negative consequences.
Perinatal depression in fathers has been the main research focus with fewer studies addressing psychological distress. Psychological distress extends beyond the restrictive symptoms associated with depression to include anxiety and stress (Schulz, 2016). Psychological or emotional distress is also often related to coping, with psychological distress generally involving a maladaptive psychological response and a range of symptoms such as anxiety, stress, and depression, arising from a variety of stressors (Button, Thornton, Lee, Shakespeare, & Ayers, 2017). Measurement of non-specific psychological distress is important to cover the whole spectrum of psychological and behavioral responses in a clinically meaningful way (Skari et al., 2002), as well as to distinguish community cases based on severity rather than purely on diagnosis (Kessler et al., 2002).
Mild to severe psychological distress has been estimated in perinatal fathers, ranging from 6.7% to 12.5% (Depression, Anxiety, and Stress Scales) (DASS-42)1 (Lovibond & Lovibond, 1995) from week six to 36 during pregnancy and from 7.8% to 11.1% during the postpartum period (Schulz, 2016), with clinically important psychological distress at 13% (General Health Questionnaire) (GHQ)2 (Goldberg, 1978) and severely intrusive stress symptoms (Impact of Event Scale) in 2% of fathers (Skari et al., 2002). The prevalence of paternal depression during the perinatal period estimated in meta-analyses ranges from 8.4% (Cameron, Sedov, & Tomfohr-Madsen, 2016) to 10.4% (Paulson & Bazemore, 2010) and from 2.3% to 8.4% (Glasser & Lerner-Geva, 2019), and in a systematic review, paternal perinatal anxiety affects between, 2% and 18% of fathers (Leach, Poyser, Cooklin, & Giallo, 2016). Paternal perinatal depression may be experienced together with feelings of loss of control and impotence in face of the demands of infant care and the sudden changes in the dynamics of the couple relationship. In some cases, fathers also express feelings of guilt at spending more time at work and being unable to be more involved in the infant’s care (McCoy, 2012).
Compared to mothers (37%), fathers experience psychological distress less frequently (13%) in the postpartum period, as measured by the GHQ (Skari et al., 2002). This finding has also been reported by other authors (Vismara et al., 2016).
A systematic review finds that risk factors for men’s psychological distress during the perinatal period have been related to low relationship satisfaction, financial burden, and poor job quality (Leach et al., 2016). These authors remark that distress at this time can also result from extreme fatigue, poor partner and/or infant health, and feelings of inadequacy as a parent. For other mental health problems, Philpott, Savage, Leahy-Warren, and FitzGerald’s (2020) narrative review identified several sociodemographic variables that contribute to depression in perinatal fathers, including paternal age, lower educational attainment, parity, unplanned pregnancy, and maternal depression.
Fathers share with mothers some risk factors for psychological distress. A few days after birth, being a single parent increases the risk of distress (GHQ) in both parents; but, for mothers, current birth complications, multiparity, and previous traumatic birth are additionally important risk for distress. At six weeks after birth, risk factors for distress for mothers and fathers are very different: anxiety is relevant for mothers and having previous children, for fathers (Skari et al., 2002).
Paternal mental health has scarcely been addressed in Latin America. The only published study on Mexican fathers identified 10% with a major depressive episode during pregnancy and 4.6% and 3.8% in the fourth and eighth weeks postpartum, respectively (Ocampo, Heinze, & Ontiveros, 2007). In Brazilian fathers, paternal clinical depression is reported in 4.5% between weeks four and eigth postpartum (Pinheiro et al., 2011) while depressive symptoms are reported in 11.9%, from week six to 12 (Pinheiro et al., 2006).
In recent decades, men have become increasingly willing and capable of cooperating with their children, but it would appear they have only recently assumed significant levels of responsibility despite that the new ideals of ‘involved’ fatherhood are still highly debated (Wall & Arnold, 2007). In this respect, the authors argue that to the extent that involvement exists, it still occurs within the framework of fathers as part-time, secondary parents, and their relationship with children remains less important than mothers.
Regarding Mexican fathers, they seem to be redefining their concepts about their parental role through their attitudes and fathering practices, but only recently have some fathers begun to attempt to reconcile work with raising and caring for their offspring (Ramírez Rodríguez & Cervantes Ríos, 2013). However, this change from the traditional role of provider to include the care of their children too is not easy, due to the absence of paternity leaves and the lack of well-payed part-time jobs that include social benefits, generating psychological distress (Tena, 2014).
Paternal psychological distress has negative consequences for infants associated with motor and socioemotional development problems in one-year-olds. A longitudinal study of over 2,000 fathers reported that fathers with high distress in the postnatal period were significantly more likely to parent with high levels of hostility, which affects the emotional and behavioral areas of their children from four to five years of age (Giallo et al., 2014).
The dearth of studies on perinatal paternal mental health in Latin America, which represent low- and middle-income countries (LMICs), with a predominance of traditional beliefs about fathers’ role (Morales, Catalán, & Pérez, 2018), warrants further research. Accordingly, the aim of the study is to explore the prevalence of psychological distress and the associated sociodemographic factors (age, marital status, occupational status, income, educational attainment, and parity) in Mexican fathers. Based on the previous review, psychological distress is expected to be higher in the postpartum than in pregnancy and that younger parents, unemployed, with lower educational levels and with more children will show higher rates of psychological distress.
The results of this study will contribute to the knowledge of paternal psychological distress in this area and provide evidence of the need for screening and prevention to reduce consequences for the father and improve the mental health of mothers and infants.
Method
Design of the study
The study was cross-sectional. The data was collected as part of the National Survey on Drug, Alcohol, and Tobacco Use ‒Spanish acronym ENCODAT‒ (ENCODAT, 2016).3 The main objective of ENCODAT was to estimate the prevalence of tobacco, alcohol, and other drugs use in the population aged 12 to 65 years, as well as assessing consumption trends, antecedents, and determinants of these problems. In addition, other mental health issues of national interest were analyzed, such as suicidal ideation and attempt, partner violence, gambling, and emotional distress.
Participants
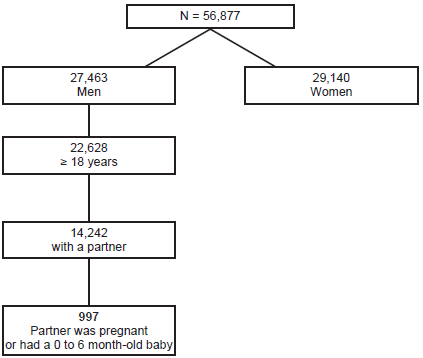
The target population of ENCODAT was people ages 12 to 65 living in the households surveyed. The sample design was probabilistic and stratified by socioeconomic variables, defined by the availability of services in the community and household characteristics. Selection of the sample involved several stages based on the Basic Geostatistical Areas (AGEB’s for its acronym in Spanish),4 blocks, households, and lastly one person was selected per household together with a teenager ages 12 and 17 if they lived in the selected household. It was possible to conduct more than one interview in each home. The households selected were visited about four times to obtain a response rate of 70%. The sample estimate was 64,000 people. The 2016 ENCODAT had national, regional, and state representation, a total response rate (household + individual) of 73.6% and a final sample of 56,877 complete interviews (27,463 men and 29,414 women), of which 9,563 were adolescents and 47,314 adults.
For the aim of this study, a sample of 997 perinatal fathers (515 during pregnancy and 482 in the postpartum period) was selected based on the following criteria: a) men who reported having a partner; b) were > 18 years old; and c) whose partner was pregnant or in the first six months postpartum period (Figure 1).
Instruments
ENCODAT comprises several sections. For this study, only the following variables were analyzed.
Sociodemographic data: age, marital status, employment status (unemployment was defined as not having engaged in paid employment in the past 30 days), income, educational attainment, number of children, and perinatal period (pregnancy/postpartum).5
Psychological distress. The Kessler Psychological Distress Scale (K6) was used to measure this aspect (Kessler et al., 2002). The six-item scale measures feelings of nervousness, hopelessness, restlessness, depression, uselessness, and overexertion. It provides a measure of the severity of symptoms and general levels of psychological distress. The total scores of the scale range from 0 to 24 points. A standard cut-off score of ≥ 13 is used to identify people with severe psychological distress, in other words, individuals with a high probability of presenting a diagnosable mental disorder severe enough to cause functional limitations and require treatment (Kessler et al., 2003). A cut-off score of ≥ 5 indicates moderate psychological distress that remains clinically relevant and therefore requires some form of intervention.
Mexico participated in the international validation of K6 through its application as part of the World Mental Health Survey conducted in 14 countries (Kessler et al., 2010). A factor analysis assessed its internal consistency at the primary care level, yielding a single factor that explained 53.4% of the total variance with internal consistency of α = .901 (Vargas, Villamil, Rodríguez, Pérez, & Cortés, 2011).
Procedure
Data collection was undertaken in various stages. Once a household had been selected, an individual was chosen for interviewing based on a questionnaire. The interview included several sections (e.g., drug and alcohol use, partner violence, harm to others, psychological distress), with only those relevant to the present study being recorded. The field work was supervised by researchers specifically trained in this task. The training of interviewers was carried out from May 16 to 30, 2016, while data collection took place June 1 to October 30 of that year.
Statistical analysis
Data was analyzed with Stata version 13.1 (STATA, 2013), using the complex survey analysis module, svy, which considers the sample design that includes the definition of weight, stratum, and grouping variable to obtain more accurate estimates. Prevalence estimates were obtained for demographic characteristics and psychological distress. In addition, differences in the prevalence of psychological distress by demographic variable were estimated with the adjusted prevalence ratio (PR), based on generalized linear models (GLM) with log link and binomial distribution. For GLMs, 95% confidence intervals (CI) were estimated.
Ethical considerations
The ENCODAT 2016 survey protocol was approved by the IRBs of the Ramón de la Fuente Muñiz National Institute of Psychiatry (Instituto Nacional de Psiquiatría Ramón de la Fuente Muñiz, INPRFM) and the National Institute of Public Health (Instituto Nacional de Salud Pública, INSP), which was also involved in the survey. All the participants were read a letter of consent and information was only gathered on those who agreed to participate. The actual analysis was approved by the IRB of the INPRFM (06/18/2018).
Results
Table 1 shows the demographic characteristics of the sample. As can be seen, participants were mostly young (19-29 years) and over half were married (52.5% pregnancy and 54.4% postpartum). Few participants were unemployed (6% pregnancy and 3% postpartum). Over half had a monthly family income of ≤ 4 minimum wages (79.8% pregnancy and 70.7% postpartum) and an educational attainment of ≤ Junior high school (58.6% pregnancy and 61.8% postpartum). The majority had one or two children (69% pregnancy and 58.8% postpartum).
Table 1 Demographic characteristics of fathers
| Pregnancy | Postpartum | ||||||
|---|---|---|---|---|---|---|---|
| n = 515 | N = 276,386 | % | n = 482 | N = 258,579 | % | ||
| Age | |||||||
| 18-29 years | 254 | 136,292 | 49.3 | 198 | 106,090 | 41.0 | |
| 30-39 years | 148 | 79,632 | 28.7 | 162 | 86,983 | 33.6 | |
| 40-49 years | 78 | 42,131 | 15.2 | 84 | 45,101 | 17.4 | |
| 50-65 years | 35 | 18,601 | 6.7 | 38 | 20,586 | 8.0 | |
| Marital status | |||||||
| Co-habiting | 245 | 131,283 | 47.5 | 219 | 117,653 | 45.5 | |
| Married | 270 | 145,103 | 52.5 | 263 | 140,926 | 54.5 | |
| Employed | |||||||
| Yes | 483 | 259,369 | 93.8 | 465 | 24,2799 | 96.5 | |
| No | 32 | 17,017 | 6.2 | 17 | 8,961 | 3.5 | |
| Monthly family income | |||||||
| ≤ 4 minimum wages* | 411 | 220,546 | 79.8 | 341 | 183,125 | 70.7 | |
| ≥ 5 minimum wages | 104 | 55,839 | 20.2 | 141 | 75,634 | 29.3 | |
| Educational attainment | |||||||
| ≤ Junior high school | 302 | 162,015 | 58.6 | 298 | 159,948 | 61.8 | |
| ≥ Senior high school | 213 | 114,370 | 41.4 | 184 | 98,812 | 38.2 | |
| Number of children | |||||||
| 0 | 48 | 25,954 | 12.3 | 40 | 21,616 | 8.5 | |
| 1-2 | 269 | 144,655 | 69.0 | 277 | 148,706 | 58.8 | |
| ≥ 3 | 73 | 39,283 | 18.7 | 154 | 82,916 | 32.7 | |
Note:
*Four monthly minimum wages equal $8,764.00 Mexican pesos ($455.28 US dollars).
Moderate psychological distress prevalence was 24.9% (pregnancy) and 29.5% (postpartum period), with no significant differences being observed between these periods. As for severe psychological distress, 1.0% presented this condition in pregnancy and 1.9% in the postpartum period, with no statistically significant differences (Table 2).
Table 2 Prevalence of psychological distress in perinatal fathers
| Pregnancy | Postpartum | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n = 515 | N = 276,386 | % | n = 482 | N = 258,579 | % | X 2 | p | ||
| Moderate Psychological Distress (K6 ≤ 5) | |||||||||
| Yes | 128 | 68,787 | 24.9 | 142 | 76,417 | 29.5 | 2.6 | .06 | |
| No | 387 | 207,598 | 75.1 | 340 | 182,343 | 70.5 | |||
| Severe Psychological Distress (K6 ≥ 13) | |||||||||
| Yes | 5 | 2,920 | 1.0 | 9 | 4,953 | 1.9 | 1.4 | .17 | |
| No | 510 | 27,3465 | 99.0 | 473 | 253,806 | 98.1 | |||
Men over 50 years of age (38.4%) presented moderate emotional distress, as well as married men (28%), those with higher income (29.4%), less educational attainment (28.8%), three or more children (30.7%), and those whose wife is in the postpartum period (29.5%) (Table 3). However, the PR-adjusted analysis for moderate psychological distress showed that none of the variables was associated with the criterion variable (Table 3).
Table 3 Prevalence ratio of moderate psychological distress (K6≥5) by demographic characteristics
| n = 270 | n = 145,204 | % (95% CI) | PR | 95% CI | p | |
|---|---|---|---|---|---|---|
| Age | ||||||
| 18-29 | 116 | 62,150 | 25.7 (20.8-31.0) | 1 | - | - |
| 30-39 | 70 | 37,810 | 22.7 (17.8-28.5) | .92 | .65-1.31 | .67 |
| 40-49 | 56 | 30,121 | 34.6 (24.7-45-8) | 1.19 | .76-1.84 | .43 |
| 50-65 | 28 | 15,123 | 38.4 (26.1-52.7) | 1.38 | .85-2.26 | .18 |
| Marital status | ||||||
| Married | 149 | 80,007 | 28.0 (23.2-33.4) | 1 | - | - |
| Co-habiting | 121 | 65,197 | 26.2 (21.4-31.4) | .89 | .66-1.20 | .45 |
| Employed | ||||||
| Yes | 257 | 138,053 | 27.1 (23.6-30.8) | 1 | - | - |
| No | 13 | 7,151 | 27.1 (16.4-42.2) | 1.12 | .79-2.35 | .26 |
| Monthly family income | ||||||
| ≥ 5 minimum wages | 72 | 38,805 | 29.4 (22.3-37.8) | 1 | - | - |
| ≤ 4 minimum wages | 198 | 106,399 | 26.3 (22.6-30.4) | 1.05 | .74-1.49 | .76 |
| Educational attainment | ||||||
| ≤ Junior high school | 172 | 92,783 | 28.8 (24.5-33.4) | 1 | - | - |
| ≥ Senior high school | 98 | 52,421 | 24.7 (19.3-30.6) | 1.07 | .78-1.45 | .66 |
| Number of children | ||||||
| 0 | 30 | 16,263 | 29.2 (18.2-43.2) | 1 | - | - |
| 1-2 | 159 | 85,380 | 25.1 (20.9-29.8) | .90 | .05-0.55 | .69 |
| ≥ 3 | 81 | 45,561 | 30.7 (23.3-39.0) | 1.07 | .01-0.44 | .78 |
| Perinatal period | ||||||
| Pregnancy | 128 | 68,787 | 24.9 (20.3-30.0) | 1 | - | - |
| Postpartum | 142 | 76,417 | 29.5 (24.7-34.8) | 1.32 | .98-1.79 | .06 |
Note: Analysis was performed with men who had a pregnant partner or during the first six months of their partners’ postpartum (N = 534,965, n = 997).
As for severe psychological distress, men older than 50 years (3.4%), more frequently presented severe emotional distress, as well as men without employment (2.4%), with less educational attainment (2.2%), without children (6.2%), and those and those with his wife are in postpartum (1.9%) (Table 4). The PR-adjusted analysis found that fathers aged 40 to 49 were at a lower risk for severe psychological distress than those aged between 18 and 29 (PR = .10; CI [.01, .79]); while having lower educational attainment (PR = 5.59; CI [1.19, 26.21]) increased the risk of severe psychological distress. Those with one or two children (PR = .16; CI [.05, .55]) or ≥ 3 (PR = .08; CI [.01, .44]) had a lower risk of severe distress than first-time fathers, while postpartum fathers (PR = 4.11; CI [1.00, 16.78]) had a higher risk of presenting severe psychological distress than fathers during their partners’ pregnancy.
Discussion and conclusion
This study found a moderate level of psychological distress in a quarter of prenatal (24.9%) and postnatal (29.5%) fathers. These percentages are higher than those reported previously by Schulz (2016), who found rates of 6.7% to 12.5% in fathers during pregnancy, and of 7.8% to 11.1% during the postpartum period; Skari et al. (2002) observed rates of 13% after childbirth. The higher prevalence found among Mexican perinatal fathers may partly be due to the differences in screening methods used, but also to the effect of living conditions on fathers in a developing country, an effect also noted in Mexican women with perinatal depression (Fisher et al., 2012; Lara, Navarrete, & Nieto, 2016). Populations in lower income countries have limited access to mental health services (Borges et al., 2006), and a high proportion experience poverty, exposing them to an increased risk of disability, where, even in the absence of absolute poverty, social inequalities and relative poverty can lead to stress, which can worsen both mental and physical health and functioning (Banks, Kuper, & Polack, 2017).
A very small percentage of Mexican fathers reported severe psychological distress (K6 ≥ 13): 1.0% during pregnancy and 1.9% in the postpartum period. The only relatively comparable study in this respect is the one by Skari et al. (2002), who found a prevalence of 2% of postpartum fathers with severe intrusive stress symptoms. Further research is required to confirm the magnitude of severe stress in perinatal Mexican fathers to rule out the fact that this low level is not due to men´s tendency to underreport mental health problems (O’Brien et al., 2017), or to mask these symptoms with externalized behavior and disorders such as substance abuse, avoidance behavior, and anger (Addis, 2008; Cochran & Rabinowitz, 2000).
Age was associated with severe psychological distress and younger fathers were found to be more distressed. Becoming a father before the mid-20s could mean that higher education is postponed because of the need to secure full-time employment to support one’s family. Parental age has been considered a mediating factor for social and psychological dynamics affecting the new parent’s emotional well-being (Bergström, 2013). However, in a systematic review, Philpott et al. (2017) found contradictory evidence regarding the contribution of age to stress levels to confirm this finding.
Severe psychological distress in perinatal fathers was also associated with low educational attainment. Despite the lack of evidence on the influence of education on paternal perinatal stress, low educational attainment reduces the ability to cope with stress (Kubzansky, Kawachi, & Sparrow, 1999), and may also reduce the opportunities for securing a better paid job.
Table 4 Prevalence ratio of severe psychological (K6 ≥ 13) distress by demographic characteristics
| n = 15 | N = 7,874 | % (95% CI) | PR | 95% CI | p | |
|---|---|---|---|---|---|---|
| Age | ||||||
| 18-29 | 10 | 5,378 | 2.2 (1.1-4.3) | 1 | - | - |
| 30-39 | 2 | 984 | .6 (.1-2.3) | .35 | .07-1.80 | .21 |
| 40-49 | 1 | 189 | .2 (.1-1.5) | .10 | .01-0.79 | .02 |
| 50-65 | 2 | 1,323 | 3.4 (.5-17.1) | .31 | .05-1.70 | .18 |
| Employed | ||||||
| Yes | 14 | 7,228 | 1.4 (.7-2.5) | 1 | - | - |
| No | 1 | 646 | 2.4 (.3-15.7) | 3.68 | .50-26.80 | .19 |
| Educational attainment | ||||||
| ≤ Junior high school | 13 | 7,040 | .4 (.1-1.6) | 1 | - | - |
| ≥ Senior high school | 2 | 834 | 2.2 (1.1-4.0) | 5.59 | 1.19-26.21 | .02 |
| Number of children | ||||||
| 0 | 6 | 3,433 | 6.3 (2.2-16.0) | 1 | - | - |
| 1-2 | 7 | 3,748 | 1.1 (.4-2.7) | .16 | .05-0.55 | .00 |
| ≥ 3 | 2 | 693 | .5 (.1-2.1) | .08 | .01-0.44 | .00 |
| Perinatal period | ||||||
| Pregnancy | 6 | 2,921 | 1.1 (.3-2.8) | 1 | - | - |
| Postpartum | 9 | 4,953 | 1.9 (.9-3.7) | 4.11 | 1.00-16.78 | .04 |
Note: Analyses were performed of men who had a pregnant partner or in the first six months of their partners’ postpartum (N = 534,965, n = 997).
Subsequent fathers were found to be less likely to experience severe psychological distress than first-time fathers. Philpott’s et al. (2017) systematic review and Darwin’s et al. (2017) study on fathers’ mental health during the perinatal period lend do not support our findings. Darwin et al. (2017) observed that, although subsequent fathers may feel less stress because of the experience gained in the previous birth, they may also experience anticipatory anxiety concerning the new birth, and face new challenges, such as having to meet the needs of the new baby and its siblings. This aspect warrants further study.
As for our finding that there is an increase in the risk for psychological distress in the postpartum, compared to the prenatal period, this contradicts the evidence that pregnancy rather than the postpartum period is a period of higher stress in men in the transition to parenthood (Condon, Corkindale, & Boyce, 2004). Differences in results could be explained by Schulz’s (2016) longitudinal study, which included three measurement points in pregnancy and three in the postpartum, finding that levels of stress, depression, and anxiety vary within each period. Fathers’ stress peaked just before and after the birth of the baby yet remained similar at other time points. After birth, depression peaked at 12 weeks and six months postpartum, and anxiety at 12 weeks postpartum. These findings point to the need for further longitudinal studies to understand the sources of stress and their effect on fathers’ mental health along the perinatal period.
There is an almost total absence of studies on the reactions of fathers to childbirth and the impact to their mental health in Latin America. The present population study is the first of its kind in Mexico. Our findings suggest that Mexican fathers experience psychological distress in the perinatal period, which needs to be further addressed. Due to the nature of this survey, no other variables could be included to provide a more comprehensive view of paternal perinatal distress, such as the impact of fathers’ involvement in childcare or sociodemographic variables during the perinatal period.
The strengths of this study are as follows: a. Findings are based on a population-based sample, which means that they can be extended to the general population of Mexican perinatal men, b. This is the first population study targeting perinatal risk for psychological distress in Mexican fathers. c. The measurement of psychological distress extends beyond the restrictive symptoms associated with depression so as to include anxiety and stress, and psychological and behavioral responses in a clinically meaningful way (Button et al., 2017); and d. The K6 scale is a valid instrument to distinguish community cases based on severity rather than purely on diagnosis (Kessler et al., 2002).
Some of the main limitations that should be considered when interpreting these findings include the fact that a) This was a cross-sectional study, which does not allow predictions from pregnancy to be extrapolated to the postpartum period; b) The primary survey contained a long section on addictions, meaning that very few questions could be included on the remaining topics, such as a longer depression scale and certain relevant psychosocial predictors, which would have shed more light on paternal perinatal depression and distress, nor any possible confounding variables; c) The study does not account for the changes over time e.g., after birth than at six months postpartum that may occur within the perinatal period in psychological distress; d) It would have been interesting to investigate the differences by states, however, this analysis could not be carried out, since out of the total N (997), the N by state was very small. It is worth mentioning that the variation by states was very small (between 2% and 5%).
Focusing on fathers’ mental health during the perinatal period is important because of the suffering it causes them, as well as its impact on mothers and infants.
As mentioned earlier, mild psychological distress was suffered by a quarter of the fathers sampled. According to Kessler et al. (2003) and Condon et al. (2004) mild psychological distress involves maladaptive psychological responses and a range of psychological symptoms, such as anxiety, stress, and depression, which are clinically relevant and therefore warrant some form of minimum preventive or efficacious minimum interventions provided by health institutions. Some elements of a universal prevention policy should include offering sources of support and advice; tailor-made information for first-time fathers about perinatal depression (Baldwin, Malone, Sandall, & Bick, 2018), infant care, their role as fathers, and potential relationship changes or strains that might be expected with their partners in routine care (Kumar, Oliffe, & Kelly, 2018).
Only a small proportion of new fathers in the sample presented severe psychological distress; this suggests that these fathers were extremely likely to present a diagnosable mental disorder severe enough to cause functional limitations and require treatment, as Kessler et al. (2003) have noted. It has been observed that severe psychological distress leads to a progression towards externalizing behavior such as anger, breaking the law, and self-harm or suicide (Schulz, 2016). Consequently, it has been suggested that both mothers and fathers should be screened for psychological status, bearing in mind that men may display the aforementioned behavior and disorders rather than typical depression symptoms (Chhabra et al., 2020). Moreover, many men have negative attitudes towards help-seeking, and are therefore less likely to seek professional care due to masculine gender norms (Addis, 2008).
These findings suggest that it is necessary to go beyond the traditional approach in prenatal health care, which is centered on the mother and tends to overlook fathers.

