











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
Burnout syndrome (BOS), describes a set of symptoms and attitudes summarized as emotional exhaustion, perception, and detachment from problems, as well as reduced personal accomplishment in those affected. This phenomenon characteristically occurs in individuals engaged in caring for others and is probably related to the chronic stress caused by the psychosocial demands that patients present during their care process (Maslach & Jackson, 1981). Hopelessness, self-invalidation, and the inability to act to improve one’s own condition are some examples of the conditions this phenomenon can produce (Gajewski, Boden, Freude, Potter, & Falkenstein, 2017).
Instruments such as the (MBI) have been developed and validated as a practical way of identifying affected populations and for some years now they have been used in most studies evaluating this phenomenon (Olivares-Faúndez, Mena-Miranda, Jélvez-Wilker, & Macía-Sepúlveda, 2014). Official sources have noted that BOS is a problem of global significance. In Mexico alone, it affects up to 75% of workers (El Universal, JADF, 2015). The consequences of failing to address this problem can affect personal as well as organizational spheres, constituting a risk factor for developing problems such as substance abuse, other psychiatric disorders, absenteeism, and decreased work performance. (Gutiérrez Aceves, Celis López, Moreno Jiménez, Farias Serratos, & Suárez Campos, 2006). A Mexican review that included over thirteen thousand employees, from various professions in various states in Mexico, reported average values for experiencing burnout corresponding to the category of “once a month or less” on the BOS symptom frequency scale (Juárez-García, Idrovo, Camacho-Ávila, & Placencia-Reyes, 2014).
WHO statistics for 2015 reported that there were 139 doctors per 100,000 inhabitants worldwide. In Mexico, according to a 2011 census (the latest census conducted by the Instituto Nacional de Estadística y Geografía [INEGI]), there were 157 doctors for every 100,000 inhabitants. In 2015, the Organization for Economic Cooperation and Development (OECD) reported the existence of more specialist doctors than General Practitioners and family doctors (65% and 35%, respectively) in Mexico. In 2017, there were 147,910 medical specialists in the country (Heinze-Martin, Olmedo-Canchola, Bazán-Miranda, Bernard-Fuentes, & Guízar-Sánchez, 2018). A total of 54.2% of the latter were concentrated in Mexico City, Estado de México, Jalisco and Nuevo León, with the remaining 45.8% being distributed among the other 28 states. Of the 32 states in Mexico, Mexico City was the one with the highest rate of specialist doctors (505.7/100,000 inhabitants), followed by Nuevo León (185.3/100,000 inhabitants) and Jalisco (172/100,000 inhabitants) (Heinze-Martin et al., 2018), a reflection of a very low density of physicians in large regions of Mexico, which can easily translate into a greater workload. Given the characteristics of the health system in Mexico, it is only to be expected that a significant percentage of this burden will be directly reflected in medical specialists in training.
Although there are studies of BOS in medical residents, incidence rates vary greatly from 18% to 82% in some studies (Willems, Monten, & Portzky, 2018). Other studies report verbal, psychological and physical abuse, and harassment during residency, generally from hierarchical superiors, affecting up to 90% of the doctors surveyed (Acosta-Fernández, Aguilera-Velasco, & Pozos-Radillo, 2017). The dual role of worker and student, the multiple lines of communication to which they have to respond, and the constant demand for attention in the performance of their work, added to the load of working hours, make trainee doctors particularly vulnerable to BOS.
BOS currently represents a serious health problem worldwide, requiring increasing attention from health prevention agency agendas in both high- and medium-income countries (Staff, 2017). Reports suggest that Mexico is one of the countries most severely affected by this problem, causing enormous losses to the productive sector every year (Celis, 2016). Health professions, particularly the medical practice are also among the most severely affected professions in this country. As mentioned earlier, during the training process, doctors are subjected to constant stress due to having to absorb large amounts of information in a short time and to develop the ability to use it in a timely manner, while at the time working in clinical fields (as in the case of medical residencies in the specialization process). The dual role of worker and student, the multiple lines of communication, and the constant demand for attention in everyday tasks, coupled with long working hours, create the ideal conditions for the development of BOS in this vulnerable population. Nevertheless, probably due to its recent phenomenological description, its incidence, effects on health and job performance, as well as its treatment, continue to be a subject of great interest despite the lack of available information. In Mexico, until recently there were no clear official regulations to protect workers from BOS. Fortunately, since 2018, the NOM-035-STPS-2018 (Norma Oficial Mexicana) on Psychosocial Risk Factors at Work has constituted a good first approach in this regard in regulatory matters. However, its dissemination and effective application are less than optimal in certain areas (Diario Oficial de la Federación, 2018).
The main objectives of this article are to describe the association between burnout syndrome and medical training by specialty in first-year residents at the Fray Antonio Alcalde Guadalajara Civil Hospital, and to identify individual or clinical/academic in-hospital characteristics that could be associated with the presence of BOS.
Method
Sample description
The study was carried out on first-year medical residents at the Fray Antonio Alcalde Guadalajara Civil Hospital, including a sample of all first-year specialties (therefore excluding sub-specialties, high specialties, and fellowships), in order to have a sample with a more acute exposure to the in-hospital stress to which medical residents are usually exposed.
A non-probabilistic study by consecutive inclusion was conducted, calculating the sample size to estimate the detection of BOS in our population. The sample size was calculated to be 54, using the CDC Epi Info software, based on the study by Willems et al. (2018).
Place
Subjects were resident doctors in their first year of training as specialists at the Fray Antonio Alcalde Civil Hospital of Guadalajara, the largest public hospital in Western Mexico, which provides medical care for people with no other social security services, meaning that the population that attends this institution is large and predominantly local.
Measurements
Those who agreed to participate in the study were included. The sociodemographic data of the sample were obtained to subsequently administer the evaluation instrument (Maslach Burnout Inventory). The MBI comprises 22 items assessing three spheres: emotional exhaustion, depersonalization, and personal accomplishment at work. In keeping with the design of the instrument, a case affected by BOS is considered to be a person who scores high on the subscales of emotional exhaustion and depersonalization, (≥ 26 and 9 points respectively) and low on the personal accomplishment subscale (≤ 34 points).
Procedures
The protocol for this research was submitted to the Subdirectorate of Postgraduate Teaching, requesting the contacts of first-year residents, who were contacted by different means: personalized letters and social network groups (WhatsApp), and invited to the general auditorium of the hospital unit for a brief psychoeducational talk on BOS. The battery of questions in this study was administered after it had been explained and subjects had been asked to give written informed consent. Those who were unable to answer the questionnaire at that meeting were contacted in person in their respective workplaces.
Data on the study subjects are completely confidential and were only extracted by a physician with standardized psychiatry training in the methods used. These data were extracted and captured using a coded instrument, and subsequently transferred to an electronic database for statistical processing.
Monitoring
Psychology and Psychiatry consultation services within the Fray Antonio Alcalde Guadalajara Civil Hospital were offered to those study subjects who achieved significant scores in the Burnout Diagnosis.
Statistical analysis
The normality of the distribution of the quantitative variables of interest was established using the Kolmogorov-Smirnov test. A statistical analysis of free distribution (medians) or parametric (means) was chosen as a function of symmetry. Descriptive statistics were used for quantitative variables and measured with medians and ranges or means, variance, and standard deviation. Proportions were used for the qualitative variables, and confidence intervals (95%) were used to measure accuracy.
For inferential statistics, a comparison of independent samples for two groups was performed using the Mann-Whitney U for ordinal variables, Student’s t for scalars, and Chi2 for the dichotomous comparison. The comparative analysis by specialty was undertaken using Kruskall-Wallis and one-factor variance analysis. A value of p < .05 was considered significant. To determine association and correlation, Pearson’s r2 correlation test was used for scalar variables and the Phi correlation coefficient for dichotomous variables.
The study adhered to the STROBE guidelines for observational (cross-sectional) epidemiological studies. Data were processed using the IBM SPSS version 20.0 program for Windows 7; Epidat produced by the Xunta de Galicia and the Pan American Health Organization version 3.1 and Epi Info version 7.0 developed by Atlanta CDC.
Results
Eighty-eight patients were included in the study. There were no losses to follow-up. The Kolmogorov-Smirnov normality test showed a normal population distribution. The mean age was 26.6 years (SD = 1.5 years). There were slightly more males in the sample (n = 45, 51.1%), and more clinical (n = 45, 51.1%) than surgical residents (n = 43, 48.9%). The most frequent specialty area was Surgery (n = 16, 18.2%), followed by Pediatrics (n = 12, 13.6%), Internal Medicine (n = 10, 11.4%), Anesthesiology and Traumatology and Orthopedics (n = 9, 10.2% each), Gynecology, Imagenology, Rehabilitation and Ophthalmology (n = 5, 5.7% each), and lastly Pathological Anatomy, Geriatrics, Genetics, Otolaryngology (ENT), Psychiatry and Medical Emergencies (n = 2, 2.3% each).
Of the sociodemographic variables of interest, most of the sample reported being single (n = 78, 88.6%). There were more subjects from Guadalajara than elsewhere (n = 51, 58% vs. n = 37, 42%), while most of the sample reported living near the hospital unit (n = 58, 65.9%). Only 9.1% of the sample had children (n = 8). Living with the family was the most common housing arrangement (n = 50, 56.8%) followed by living with roommates (n = 16, 18.3%), living alone (n = 12, 13.6%), and finally only with parents (n = 10, 11.4%). The average number of people with whom they shared a dwelling was two (SD 1.43). A total of 40.9% of the sample reported having additional financial support to the scholarship granted by the medical residency (n = 36).
Regarding the variables of interest in the workplace, the average workload per week was 95.2 hours (SD 32.1), with a mean load of 48.1 on-call hours per week (SD 27) and a mean load duration during a “post-on-call” period of 9.6 hours (SD 4.7). The most prevalent on-call schedule was AD (n = 46, 52.3%), followed by AC (n = 17, 19.3%), AF (n = 11, 12.5%), and AE (n = 10, 11.4%), while, 4.5% reported that they did not performed any on-call shifts.
The mean number of hours of academic activity during the on-call period was 1.7 (SD 3.8). The activity most commonly reported as consuming the greatest amount of time in the working day were clinical notes (n = 25, 28.4%), followed by procedures (n = 20, 22.7%), rounds (n = 19, 21.6%), patient interviews (n = 13, 14.8%), other (n = 10, 11.4%), and lastly academic activities (n = 1, 1.1%).
During a typical working day, the average number of hours spent on patient interviews was 4.4 hours (SD 4.2), the average number of hours for daily academic activities was 1.7 (SD 1.4), the average number of hours spent making clinical notes was 5.4 hours (SD 4.2), and, finally, the mean number of hours used for procedures was 4.5 hours (SD 4.1).
Regarding intrahospital communication, upward communication was reported as being poor in 35.2% of cases (n = 31), followed by good (n = 26, 29.5%), fair (n = 23, 26.1%), very poor (n = 5, 5.7%), and excellent (n = 3, 3.4%). As for lateral communication, most of the sample reported it as good (n = 44, 50%), followed by excellent (n = 27, 30.7%), fair (n = 8, 9.1%), poor (n = 7.8%), and very poor (n = 2, 2.3%). In the case of downward communication, most of the sample reported it as good (n = 44, 50%), followed by excellent (n = 27, 30.7%), fair (n = 8, 9.1%), poor (n = 7.8%), and very poor (n = 2, 2.3%).
Support from medical personnel was reported as fair in most of the sample (n = 29, 33%), followed by good (n = 26, 29.5%), poor (n = 23, 26.1%), excellent (n = 5, 5.7%), and very poor (n = 5, 5.7%). Finally, support from administrative staff was reported as fair (n = 32, 36.4%), poor (n = 26, 29.5%), good (n = 14, 15.9%), very poor (n = 12, 13.6%), and excellent (n = 4, 4.5%).
Burnout syndrome was present in 21.6% of the sample (n = 19) with the mean score being 71.5 points (SD 14.8). A total of 53.4% of the sample displayed emotional exhaustion (n = 47) with a mean score of 28.1 (SD 10.86), while 53.7% showed depersonalization (n = 47) with a mean score of 10 points (SD 5.3), and finally 39.8% presented reduced personal accomplishment (n = 35) with a mean score of 33.8 points (SD 5.8) (Figure 1).

Figure 1 Distribution of frequencies of Burnout Syndrome and of the three categories evaluated in the Maslach Burnout Inventory.
The sample was divided into two groups for analysis based on whether they had burnout syndrome (Table 1).
Table 1 Results as a function of the presence or absence of Burnout Syndrome
|
Presents
Burnout |
Does not
present Burnout |
||
|---|---|---|---|
| Variable | (n = 19) | (n = 69) | p |
| Sex, n (%) | .711 | ||
| Female | 10 (52.6) | 33 (47.8) | |
| Male | 9 (47.4) | 36 (52.2) | |
| Age, mean (SD) | 26.9 (1.5) | 26.5 (1.6) | .519 |
| Group, n (%) | .883 | ||
| Surgical | 9 (47.4) | 34 (49.3) | |
| Clinical | 10 (52.6) | 35 (50.7) | |
| Specialty, n (%) | .879 | ||
| General Surgery | 4 (21.1) | 12 (17.4) | |
| Gynaecology | 2 (10.5) | 3 (4.3) | |
| Pediatrics | 4 (21.1) | 8 (11.6) | |
| Internal Medicine | 2 (10.5) | 8 (11.6) | |
| Anesthesiology | 2 (10.5) | 7 (10.1) | |
| Imagenology | 1 (5.3) | 4 (5.8) | |
| Ophthalmology | 1 (5.3) | 4 (5.8) | |
| Psychiatry | 1 (5.3) | 1 (1.4) | |
| Traumatology | 1 (5.3) | 8 (11.6) | |
| Emergency Medicine | 1 (5.3) | 1 (1.4) | |
| Pathology | 0 (0) | 2 (2.9) | |
| Geriatrics | 0 (0) | 2 (2.9) | |
| Genetics | 0 (0) | 2 (2.9) | |
| Rehabilitation | 0 (0) | 2 (2.9) | |
| ENT | 0 (0) | 2 (2.9) | |
| Origin, n (%) | .596 | ||
| Local | 10 (52.6) | 41 (59.4) | |
| Elsewhere | 9 (47.4) | 28 (40.6) | |
| Residence, n (%) | .405 | ||
| Near | 11 (57.9) | 47 (68.1) | |
| Far | 8 (42.1) | 22 (31.9) | |
| Marital status, n (%) | .716 | ||
| Single | 16 (84.2) | 62 (89.9) | |
| Married | 2 (10.5) | 3 (4.3) | |
| Living together | 1 (5.3) | 3 (4.3) | |
| Divorced | 0 (0) | 1 (1.4) | |
| Children, n (%) | .512 | ||
| No | 18 (94.7) | 61 (89.9) | |
| Yes | 1 (5.3) | 7 (10.1) | |
| People, n (%) | .330 | ||
| Alone | 2 (10.5) | 10 (14.5) | |
| Parents | 1 (5.3) | 9 (13) | |
| Family | 10 (52.6) | 40 (58) | |
| Roommates | 6 (31.6) | 10 (14.5) | |
| Financial support | .047 | ||
| No | 15 (78.9) | 37 (53.6) | |
| Yes | 4 (21.1) | 32 (46.4) | |
| Workload, average hours/week (SD) | 98.4 (16.9) | 94.3 (35.2) | .032 |
| Weekly workload, n (%) | .032 | ||
| Over 80 hrs. | 18 (20.3) | 49 (55.3) | |
| Under 80 hrs. | 1 (1.1) | 20 (22.6) | |
| On-call workload (hours/week), mean (SD) | 56.6 (10.7) | 46.4 (29.7) | .001 |
| On-call workload, n (%) | .001 | ||
| Over 48 hrs. | 19 (100) | 43 (62.3) | |
| Under 48 hrs. | 0 (0) | 26 (37.7) | |
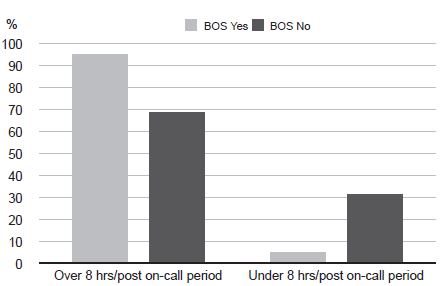
| “Post-on-call” (hours/period), mean (SD) | 10.1 (2.5) | 9.51 (5.1) | .019 |
| “Post-on-call” workload, n (%) | .019 | ||
| Over 8 hrs. | 18 (94.7) | 47 (68.1) | |
| Under 8 hrs. | 1 (5.3) | 22 (31.9) | |
| On-call schedule, n (%) | .487 | ||
| AC | 5 (26.3) | 12 (17.4) | |
| AD | 11 (57.9) | 35 (50.7) | |
| AE | 2 (10.5) | 8 (11.6) | |
| AF | 1 (5.3) | 10 (14.5) | |
| No | 0 (0) | 4 (5.8) | |
| Time available for meals (min), mean (SD) |
58.3 (39.1) | 67.4 (55.8) | .009 |
| Academic workload per on-call shift (hours), mean (SD) |
1.1 (0.6) | 1.9 (4.3) | .900 |
| Activity that takes up most time, n (%) | .586 | ||
| Interviews | 2 (10.5) | 11 (15.9) | |
| Academic | 0 (0) | 1 (1.4) | |
| Notes | 5 (26.3) | 20 (29) | |
| Rounds | 7 (36.8) | 12 (17.4) | |
| Procedures | 3 (15.8) | 17 (24.6) | |
| Other | 2 (10.5) | 8 (11.6) | |
| Hours/day of interviews, mean (SD) | 4.6 (4.1) | 4.3 (4.3) | .415 |
| Hours/day of academic activities, mean (SD) |
1.4 (1.09) | 1.8 (1.5) | .546 |
| Hours/day of notes, mean (SD) | 6.2 (3.4) | 5.2 (4.3) | .003 |
| Hours/day of procedures, mean (SD) | 5.1 (3.1) | 4.3 (4.4) | .004 |
| Downward communication, n (%) | .014 | ||
| Excellent | 0 (0) | 3 (4.3) | |
| Good | 0 (0) | 26 (37.7) | |
| Fair | 8 (42.1) | 15 (21.7) | |
| Poor | 11 (57.9) | 20 (29) | |
| Very poor | 0 (0) | 5 (7.2) | |
| Lateral communication, n (%) | .393 | ||
| Excellent | 5 (26.3) | 22 (31.9) | |
| Good | 9 (47.4) | 35 (50.7) | |
| Fair | 1 (5.3) | 7 (10.1) | |
| Poor | 4 (21.1) | 3 (4.3) | |
| Very poor | 0 (0) | 2 (2.9) | |
| Downward communication, n (%) | .267 | ||
| Excellent | 2 (10.5) | 21 (30.4) | |
| Good | 13 (68.4) | 32 (46.4) | |
| Fair | 2 (10.5) | 13 (18.8) | |
| Poor | 2 (10.5) | 3 (4.3) | |
| Very poor | 0 (0) | 0 (0) | |
| Medical staff support, n (%) | .014 | ||
| Excellent | 0 (0) | 5 (7.2) | |
| Good | 2 (10.5) | 24 (34.8) | |
| Fair | 7 (36.8) | 22 (31.9) | |
| Poor | 10 (52.6) | 13 (18.8) | |
| Very poor | 0 (0) | 5 (7.2) | |
| Administrative staff support, n (%) | .575 | ||
| Excellent | 0 (0) | 4 (5.8) | |
| Good | 2 (10.5) | 12 (17.4) | |
| Fair | 9 (47.4) | 23 (33.3) | |
| Poor | 5 (26.3) | 21 (30.4) | |
| Very poor | 3 (15.8) | 9 (13) |
Note: SD = Standard deviation; ORL = Otolaryngology.
There were no differences in presenting BOS by sociodemographic characteristics, group, or type of specialty. An association was found between presenting BOS and not receiving financial assistance in addition to the specialty grant (ro = .212, p = .047). A slight, statistically significant association directly proportional to the size of the workload was found with the presence of BOS (ro = .229, p = .032). Residents with a workload of over 80 hours were 7.3 times more likely to present burnout than those with a smaller workload (RR 7.34, CI 95% [2.1, 58.7]). Moreover, an association was found between residents who were on call for over 48 hours a week and the presence of burnout (ro = .34, p = .001) (Figures 2 and 3 ).


There was a statistically significant, slight and directly proportional association between the number of hours in the “post-on-call” period and the presence of burnout (ro = .249, p = .019). Residents with more than eight “post-on-call” hours were 8.4 times more likely to present burnout than those with fewer hours (RR 8.42; 95% CI [2.4, 67.1]) (Figure 4).
Residents with fewer than 60 minutes a day for meals were four times more likely to present burnout compared to the rest (RR 4.06; 95% CI [2.1, 12.04], p = .009). Regarding work activities, an association was observed between the number of hours spent on notes and the presence of BOS (ro = .319, p = .003). Residents who spent more hours on their notes were 13 times more likely to have BOS than those who spent fewer hours on this task (RR 13.05; 95% CI [2.01, 103.3]).
Moreover, a statistically significant association was observed between the number of hours spent on procedures and the presence of BOS (ro = .303, p = .004). Residents who spent over two hours a day on procedures were 7.3 times more likely to have BOS than those who spent fewer hours on this (RR 7.3; 95% CI [1.99, 34.2]).
Emotional exhaustion was statistically significantly associated with the length of time of being on-call (p = .001). The presence of depersonalization was also significantly associated with the length of time of being on call (p = .022), time for eating (p = .013), and hours spent on notes (p = .024). At the same time, there were differences in reduced personal accomplishment between residents with and without additional financial support (p = .056) and the number of hours spent on procedures (p = .043). The perceived quality of upward communication (z = -1.953, p = .050) and medical support (z = -2.167, p = .030) is different among residents who presented exhaustion.
Discussion and conclusion
The research shows that the prevalence of BOS in first-year residents at the Fray Antonio Alcalde Guadalajara Civil Hospital varies between each of the specialties, with a higher frequency of cases occurring in Pediatrics and General Surgery services. However, no significant association was found with the group or type of specialty, unlike what has been reported in other studies. The high incidence of BOS (66%) in both services is striking. This phenomenon could be explained by the teaching style used and the way medical practice is carried out: 1. These are services with a high caseload, requiring long working days, with fewer care personnel than is usually required; 2. Traditional medical education systems tend to be rigid and hierarchical, fostering communication styles that easily turn into workplace bullying and harassment. It would be important to replicate similar studies both in the specialties identified with high BOS rates and the others, and to identify the characteristics that might be responsible for this maladaptive response.
Despite the fact that the total incidence of BOS within the sample (which, as previously noted, includes physicians about to complete their first year of residency) does not include most of the participants, it is still relevant and significant, particularly if a separate analysis is conducted of each of the categories, in which over half the sample scores high on the “Emotional exhaustion” and “Depersonalization” sections. It is worth mentioning the fact that since the instruments used are self-reports, this could skew results, creating responses that underestimate the absolute value of the MBI. Many of the factors associated with the development of symptoms of illness due to BOS which appear both in the literature already discussed and in these results are related to the organizational climate and workloads. Mexican regulations establish clear parameters, although they are still far from those suggested by equivalent systems in other countries. However, for whatever reasons, there are still cases where these guidelines are not followed.
A study such as this one creates new knowledge that acts as a situational diagnosis of the work stress conditions affecting medical residents who perform their work at the institution. It helps determine the scope of the problem and encourages one to consider possible factors that contribute to its origin and maintenance. This information also sets a precedent for formulating various action plans, whose impact on the mental health and well-being of the population affected could subsequently be compared. BOS must be prevented. However, it is also necessary to promote and establish remedial measures for existing conditions, which may have repercussions on the training institutions and the patients themselves.
It is also clear that it is feasible to conduct this type of evaluation in a structured way as a mechanism for monitoring working conditions. It is essential to design and implement intervention programs for BOS prevention and management.
The main limitations identified by the authors are related to the possible biases due to the self-applicable nature of the MBI, which may under-estimate symptoms. Moreover, variations in the number of participants by specialty make it difficult to establish more robust associations between them.
Data for certain first-year residents could not be included, mainly due to external rotations and vacation periods.

