










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkBoletín médico del Hospital Infantil de México
versión impresa ISSN 1665-1146
Bol. Med. Hosp. Infant. Mex. vol.62 no.6 México nov./dic. 2005
Caso clínico
Eyelid fish–hook injury: case report
Herida de párpado por anzuelo. Reporte de un caso
Dr. Dante Alejandro Fuentes–Mallozzi1, Dr. Carlos Armando Méndez–Orozco2
1Departamento de Pediatría, Hospital Infantil de Tamaulipas, Secretaría de Salud, Cd. Victoria, Tamaulipas;
2Departamento de Cirugía General, Hospital General de Tampico Dr. Carlos Canseco, Secretaría de Salud, Tampico, Tamaulipas, México.
Solicitud de sobretiros:
Dr. Dante A. Fuentes–Mallozzi,
Calle 19 y Sierra Hermosa No. 342, Fracc. Arboledas,
C. P. 87027, Cd.Victoria, Tamaulipas, México.
Fecha de recepción: 06–09–2004.
Fecha de aprobación: 09–12–2005.
Abstract
Introduction. Injuries caused by fishing gear are common, but uncommon in the eye.When hooks are involved, removal must be careful and a complete revision of the rest of eye structures must be performed.
Case report. A 13 years old male suffered a penetrating fishhook injury on the upper right eyelid. Extraction was performed under general anesthesia using an extra conjunctival horizontal technique approach with satisfactory outcome.
Conclusion. The injuries caused by these objects are dangerous and extraction must be carefully done. A multidisciplinary approach must be performed.
Key words. Fishhook; penetrating injury; eyelid.
Resumen
Introducción. Las lesiones por objetos de pesca son comunes, no así en ojos y anexos. Su extracción debe ser cuidadosa y deberá realizarse revisión minuciosa de las estructuras afectadas.
Caso clínico. Adolescente masculino de 13 años de edad que accidentalmente sufrió una herida penetrante por anzuelo en párpado superior derecho. Se realizó extracción bajo anestesia general balanceada mediante abordaje palpebral horizontal extraconjuntival, con evolución satisfactoria.
Conclusiones. Las lesiones por estos objetos son graves y su manejo debe ser integral.
Palabras clave. Anzuelo; herida penetrante; párpado.
Introduction
There are two main aspects of fishing related injuries. One is the mechanical aspect, caused by penetrating foreign bodies and the other is infection. Although, fishing injury related infections are quite common and usually trivial, they can cause severe damage an even death. The injuries caused by penetration of foreign bodies in fishing, such as hooks, harpoons, special fishing knives and even scales, are relatively common in fishing, both professional and amateur. Most of these objects are designed to catch and hold fish and many different types and sizes of fishhooks are available. There are simple single barbed, multiple barbed and treble fishhooks. Because of their very irregular shape, simple extraction by pulling is not recommended, because further damage may occur.1
Reports of ocular fishhook injuries are rare and uncommon in literature, yet potentially vision threatening. Corneal scaring, retinal detachment and endophthalmitis may result.We present a case of a male with a fishhook eyelid injury and a review of literature finding only a few cases similar to the present, none in Mexico.
Case report
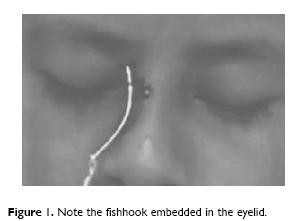
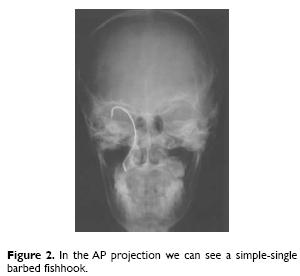
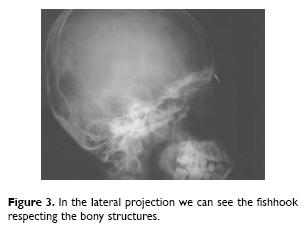
Thirteen years old male, without important previous medical history; resident of the Fishing Camp located at the Laguna Madre, 40 min away from nearby hospital. Most of the Laguna Madre population, work as fisherman. Fishing with his father, the patient located himself at his back, when he threw the fishhook, that dropped hooking and remaining embedded in the right upper eyelid of patient.The father cut off the fishing line and made no attempt to remove hook and drove to hospital. Patient arrived conscious, reactive, cooperative, with normal vital signs, just referring pain on eyelid. The eye was intact, but we found an injury of 0.2 cm located in the right upper eyelid which was the entrance site of the fishhook without exit site (Fig. 1). Normal preoperative exams were performed; lateral head x–ray revealed that fishhook was located in soft tissues around the eye not involving bony structures (Figs. 2 and 3). We decide to perform an intervention under general anesthesia to remove fishhook and a complete revision of the near soft tissues.
After normal antiseptic measures we proceed to cut the fishhook at the level of the site of entrance with pliers. Then the eyelid was infiltrated with 1% lidocaine hydrochloride with epinephrine. Using a number 15 blade, a horizontal incision was performed over eyelid from the inner to the external angle of the right eye, followed by electric cauterization of tissues for hemostasis. Then followed by soft tissue dissection and searching the fishhook point. Its extraction was easy and the surrounding structures were free of injury. We sutured muscular tissue with polyglactina 910 number 4–0 (Vycril. Ethicon, Inc. Somerville, NJ. USA) with continuous suture and the skin with nylon number 4–0 (Dermalon. Sherwood–Davis & Geck. St. Louis, MO. USA) subdermic; we applied topical chloramphenicol and the eye was covered for 24 hours. Dicloxacilin (100 mg/kg/d), metamizol (50 mg/kg/d) and tetanus toxoid booster were indicated. Patient was discharged after 48 hours on a regimen of oral dicloxacilin and acetaminophen, without pain and with normal visual acuity.After seven days he had a well clinical evolution.
Discussion
The ocular injuries by fishhook are uncommon and have a high risk of severe damage and lost of vision, for both reasons the management of this injuries is important. In the actual literature there are reports of ocular damage with penetrating or non–penetrating injuries and they are a public health problem. We found different causes of ocular trauma thus organic material even fetal monitoring spiral electrode, pens, airbags, stones, human bites or animal bites, toys, fall downs, furniture, clothing hooks, etc., had been referred in literature.2–4
In Mexico at pediatric ages there is a report by Ugalde et al.2 Found, in five years, 53 traumatic eye cases: 17 patients suffered injuries by fall downs and nine of them with clothing hooks, in 46 the injury occurred at home and a family member was witness.
Fishing is a sport and a way of life by millions of people throughout the world. It involves all age groups, and does not require special training or fancy equipment. However the injuries produced by fishing gear may occur at any moment.1 Injuries by fishhook are uncommon, actually there are a few reports on international literature, and none was found in Mexican literature.
Deramo et al.5 made a case report of a 24 years old male who suffered an ocular injury by fishhook that involved the upper eyelid and cornea of left eye, after surgery the evolution was satisfactory. Krott et al.6 reported a teenager male, that had been playing with a fishing rod while sitting on a tree, and was trying to hook fruit in the ground, the line recoiled swiftly and pierced the upper lid of the left eye and suffered an scleral rupture too. Quintyn et al.7 reported a 22 years old male with right upper eyelid injury caused by a sinker and patient lost his eye because of sinker's impact. Another similar case was reported by Coden8 in a 26 years old male who suffered a right eye injury also by a sinker, resulting in a ruptured and lost eye globe. Kamath9 reports an unusual case of a 44 years old male with a fishhook embedded in his left upper eyelid, it was loaded with nine live maggots used as bait. For extraction, the hook was rotated so that the barb emerged through the eyelid skin, the barb was snipped off using a wire cutter and the hook was rotated back and removed, with good outcome. Kalyana–sundaram et al.10 reported in 2003 a 46–year–old woman presented to the eye casualty with a three–pronged steel fishhook embedded in her left eye. She had been fly fishing using a 20 Gauge, 20 mm long salmon hook. While whipping the line back to cast her hook, she felt a blow on her eye as if she had been hit with a stone. The shank of the fishhook, with an intact fly had penetrated the medial bulbar region 5 mm posterior to the limbus. All the three prongs were lying just outside the globe, with one barb embedded in the lower lid. The visual acuity was hand movements in the affected eye. X–rays showed penetration of 18 mm of the shank of the hook into the tissues (Fig. 1), with no bony injury. Under general anesthesia, the barb was released. After much surgery the outcomes were nice.10
Patient evaluation
Most fishhook injuries are penetrating and do not involve deeper tissue structures because of the linear forces applied along the fishing line to the fishhook that drive the point parallel to the skin and keep it from deep penetration.
Many different type and sizes of fishhooks are available. When examining the hook, it is important to notice if the fishhook is single, multiple or treble, whether the hook is barbed, and the number and location of the barbs –these details will help to determine the best removal technique.
Occasionally, more serious tissue trauma occurs from fishhook injury. While not routinely performed, X–rays may aid in determining the type of fishhook and depth of penetration in difficult cases.11
Principles of removal
Five primary techniques have been described for the removal of fishhooks: retrograde, needle cover, advance and cut, string yank and vertical eyelid–splitting.5,11
1. Retrograde technique: is the simplest but has a lowest success rate. It works well for barbedless and superficially embedded hooks, downward pressure is applied to the shank of the hook, this maneuver helps rotate the hook deeper and disengage the barb, if present, from the tissue, the hook can then be back out of the skin along the path of entry.
2. Needle cover technique: it works well for the removal of large hooks with single barbs, but is most effective when the point of the fishhook is superficially embedded. An 18 –gauge or larger needle is advanced along the entrance wound of the fishhook, the direction of insertion should be parallel to the shank. The physician then should advance the fishhook to disengage the barb, pulling and twisting in a way so that the point enters the lumen of the needle. The physician can then back out the fishhook, taking care of moving the needle along the tract with the fishhook.
3. Advance and cut technique: is most effective when the point of the fishhook is located near the surface of the skin. Using pliers on needle driver, the point of the fishhook (including the entire barb) is advanced throughout the skin.The point is then cut free with pliers or another cutting tool allowing the rest of the fishhook to be backed out.
4. String yank technique: a string, such a fishing line, umbilical tape or silk suture, should be wrapped around he midpoint of the bend in the fishhook with the free ends of the string held tightly. Continue to depress the eye or distal portion of the shank of the hook, taking care to keep the shank parallel to the underlying skin. A firm quick jerk is applied while continuing to exert pressure on the eye of the fishhook.
5. Described by Deramo et al.5 in 1999, applied this technique using a vertical incision on eyelid with satisfactory results.11,12
Initially we tried to remove the fishhook using the advance and cut technique but it was not possible, because of the resistance of the fishhook and the fear of further injury to the eye. So we decided to use a blepharoplasty technique, because we have performed it before and the aesthetic results are better. The technique applied is not described for the fishhook removal in the literature and we think it should be useful.
After removal of the fishhooks, the wound should be explored for possible foreign bodies an other injuries. The uses of antibiotics are indicated such as tetanus toxoid booster. The patient must be sent to an ophthalmologist for eye revision.11,13 In the absence of this specialty in our Hospital we had to perform this surgery. All precautions must be taken when fishing, even in the company of and expert, people around fisherman should be accounted of their location.
Acknowledgments
The authors thank to Hospital General de San Fernando, Tamaulipas, Mexico; place where we made our social service and Dra. Nora I.Velazquez Quintana, for her help in the review of the manuscript and its traduction.
References
1. Dudkiewicz I, Salai M, Blankstein A, Chechik A. Fishing penetration injuries. Br J Sports Med. 2000; 34:459–62. [ Links ]
2. Ugalde–Palacios R, Ordaz–Favila JC, Salazar–León JA.Traumatismo ocular en niños: experiencia en el Instituto Nacional de Pediatría. Rev Mex Oftalmol. 2000; 74: 11–6. [ Links ]
3. Katsuya–Lauer A, Rimmer OS. Eyelid laceration in a neonate caused by an internal fetal monitoring spiral electrode. Am Ophthalmol. 1998; 125:715–7. [ Links ]
4. Lueder GT. Air–bag associated ocular trauma in children. Ophthalmology. 2000; 107: 1472–5. [ Links ]
5. Deramo VA, Maus M, Cohen E, Jeffers J. Fish hook injury of the eyelid: an unusual case removal of a fishhook in the eyelid and cornea using a vertical eyelid–splitting technique. Arch Ophthalmol. 1999; 117:541–2. [ Links ]
6. Krott R, Bartz–Schmidt KU, Heinmann K. Laceration of the eye with a fishing hook. Br J Ophthalmol. 1999; 83: 1194. [ Links ]
7. Quintyn JC, Massy J, Retout A.The hook is not the most dangerous. Arch Ophthalmol. 2000; 118:49. [ Links ]
8. Coden D. Ruptured globe caused by a fishing sinker. Arch Ophthalmol. 2002; 120:407. [ Links ]
9. Kamath GG. Fish hook injury of the eyelid: An unusual case. Br J Ophthalmol. 2000; 84:441 –2. [ Links ]
10. Kalyanasundaram TS, Depla D, Steel D.An unusual case of severe penetrating ocular injury with the shank of a triplet fish hook. Eye. 2003; 17: 663–4. [ Links ]
11. Gammons M, Jackson E. Fishhook removal. Am Fam Physician. 2001; 63: 2231–6. [ Links ]
12. Cannava PE. Fishhook removals. Arch Ophthalmol. 1999; 117: 1668. [ Links ]
13. Khaw PT, Shah P, Elkington AR. ABC of eyes: injury to the eye. BMJ. 2004; 328: 36–8. [ Links ]

