text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkWhen Eduardo Lazcano invited me to collaborate in the preparation of the book Cancer: Advances in diagnosis, treatment, prevention and control, edited by the National Institute of Public Health, I considered the convenience of presenting a document stating some of the unique characteristics of leukemia, both acute and chronic, in Mexico. After being involved in this field for more than 30 years and having participated in the diagnosis, treatment and follow-up of more than 1 200 patients with diverse types of leukemia in our country, I have been able to perform various observations of the disease that I will attempt to summarize in a concise way.
Acute lymphoblastic leukemia (ALL)
Immunologic classification of acute leukemia has been conducted in Mexico since 1983. Prior to 1983 and beginning in 1953, the diagnosis and classification of leukemia were merely supported by morphologic criteria. This change has led to a significant improvement in the prognosis of patients with leukemia in Mexico.1,2 Since 1994, implementation of ALL molecular markers such as BCR/ABL, TEL/AML1, FLT3, NPM-1 chimeric genes and mutations in IKAROS, which are widely and routinely used in Mexico, has allowed a better classification, selection and treatment follow-up of these leukemias.3 However, nutritional aspects of patients are critical in our environment; malnourished children with ALL have a worse evolution than well-nourished children. These observations, initially performed in Mexico,4 have been corroborated in other developing countries where it has been found that nutritional status is associated with the socioeconomic condition of patients and adherence to treatment, among other variables.5
Combined highly aggressive polychemotherapy treatment schemes for ALL - type HyperCVAD - are associated with higher morbimortality in treated patients. In Mexico, outcomes obtained with less aggressive and complex schemes are as efficient as other approaches but are associated with lower morbimortality.6 In addition, these schemes can be administered on an outpatient basis and are associated with better quality of life for the treated patient. For high-risk or relapsing patients with ALL, bone marrow transplantation (BMT) performed with reduced-strength schemes and on an outpatient basis is associated with favorable outcomes that are better than those obtained with combined chemotherapy.7 Introduction of tyrosine kinase inhibitors (TKIs) for treatment in patients with ALL and the Philadelphia chromosome has dramatically improved their prognosis.8 New drugs for the treatment of patients with ALL, such as clofarabine and blinatumomab, have been used rarely in Mexico due to their high costs.
Acute myeloid leukemia (AML)
Acute promyelocytic (M3) and megakaryoblastic (M7) leukemias are more prevalent in Mexico than within Caucasian populations, likely owing to genetic causes.9,10 The poor prognosis of promyelocytic leukemia in the past has dramatically changed with the use of retinoid and arsenic trioxide. Mexico took part in a multinational study directed to improve the prognosis of patients with M3 AML using a simplified and affordable treatment and achieving very satisfactory outcomes.11 The use of AML molecular markers such as AML1/ETO, inv16, PML/RARa, FLT3, NPM1 and BCR/ABL has significantly improved AML diagnosis and classification and has allowed a treatment response follow-up, which is critical for these diseases.12 AML with core-binding factor (CBF) mutations is similarly prevalent in Mexico and Caucasian countries and is associated with a better prognosis than AML without these mutations.13 In Mexico, novel treatments for AML such as gemtuzumab-ozogamicin have been restricted due to their high costs. The introduction of BMT with reduced-intensity conditioning on an outpatient basis is associated with favorable AML outcomes. There has been over 20 years of BMT experience in Mexico, which has been reproduced in other developing countries, thereby improving the prognosis of patients with AML, mainly in transplants performed during first remission.14 The acquired knowledge in Mexico regarding acute hybrid leukemia has demonstrated a poor prognosis, which has also been described in other populations worldwide.15
Chronic myeloid leukemia (CML)
In Mexico, these diseases usually occur in younger patients compared with those in Caucasian populations. Routine BCR/ABL tests, available since 1994 in Mexico, have allowed molecular verification of the diagnosis of CML, patient follow-up and, more recently, choice of treatment.16 Treatment with TKIs, such as imatinib, dasatinib, and nilotinib, among others, remains the treatment of choice for patients with CML. Regrettably, TKI treatments are highly expensive, restricting their use in limited economies, which are prevalent in Mexico.17 BMT is considered the only curative therapy for the treatment of CML patients in Mexico.18 It is estimated that with the costs of less than one year of TKI treatment, it is possible to defray a complete BMT by means of the "Mexican method", characterized by reduced-intensity conditioning on an outpatient basis. In many cases in Mexico, decisions on whether to offer TKI or BMT treatment to CML patients depend on economic conditions, access to public or private health services, and stable employment.19 The trend to reduce BMT in patients with CML observed in developed countries is not seen in Mexico owing to the previously described causes; a similar trend is observed in Latin American and other developing countries. The "Mexican method" for bone marrow transplant in patients with leukemia has been implemented in other countries with unfavorable economies, such as ours, and has shown similar outcomes.18,19 The availability of molecular biology methods for the diagnosis and follow-up of patients with this neoplasm has considerably improved its prognosis.16 Compared with other leukemias, CML has shown the most improved prognosis during the last decade due to the availability of molecular treatment and BMT implementation. Overall survival of patients with CML has significantly increased during the last decade despite the fact that suboptimal TKI treatment responses in mixed-blood Mexicans have been documented compared with that described in Caucasian populations.20 In this regard, there should be real support for the implementation of BMT in Mexican patients with CML.
Chronic lymphocytic leukemia (CLL)
CLLs are the most common leukemias in Caucasian countries but are rare in Mexico,21 most likely because of the genetic composition in mixed-blood Mexicans, with a high proportion of Asian genes. Accurate identification of this neoplasm and its variants using multiparametric flow cytometry, available since 1983 in Mexico, has been highly improved and, in some cases, is determinant for treatment election.22,23 Hairy-cell leukemia or leukemic reticuloendotheliosis, a CLL variant, is infrequent in Mexico and displays a geographic distribution that may be associated with exposure to agrochemicals.24 The use of monoclonal antibody therapies such as rituximab, which targets the CD20 antigen found in several CLL variants, has improved therapy responses, especially when combined with drugs such as fludarabine and cyclophosphamide. The low prevalence of CLL in Mexico21 has resulted in little experience at the national level regarding new drug treatments such as obinutuzumab, ofatumumab, ibrutinib and idelalisib, which have drastically altered the prognosis of patients with CLL.
Donor cell leukemia (DCL)
The cumulative experience regarding allogeneic BMT25 over the last 20 years has led to the discovery of numerous DCL characteristics, which were considered unusual in the past but are now recognized as having been under-estimated with respect to their prevalence.26-28 Understanding the mechanisms of leukemogenesis within iatrogenic conditions has allowed great advances in the knowledge of the origin of leukemias27 as well as the design of strategies for their optimal treatment.27,28
Conclusions
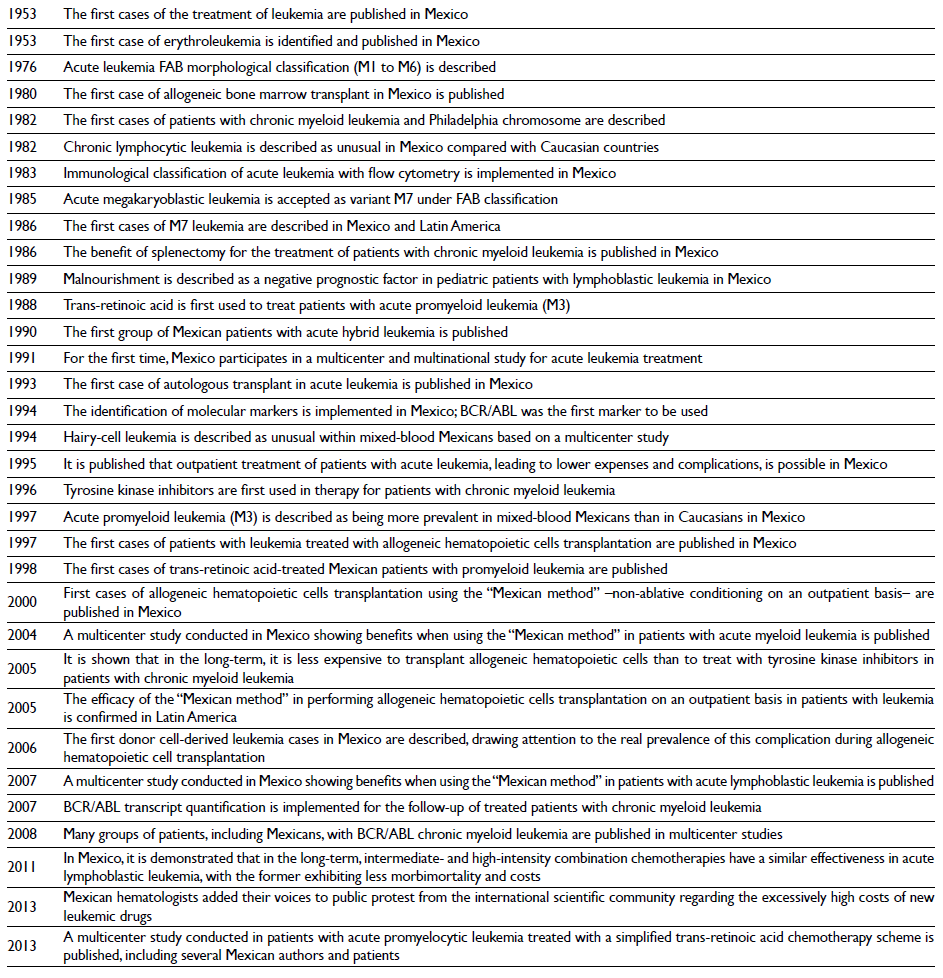
In Mexico, the distribution of leukemic types and subtypes is different compared with other countries. The implementation of novel technologies such as flow cytometry and molecular biology in the last three decades has allowed the discovery of details regarding acute and chronic leukemia in Mexico (figure 1). Leukemia treatments have been adapted to economic conditions in Mexico and have occasionally served as the basis of treatments in other developing countries. Studies conducted in Mexico on these diseases have been confirmatory but have also generated new knowledge (table I).
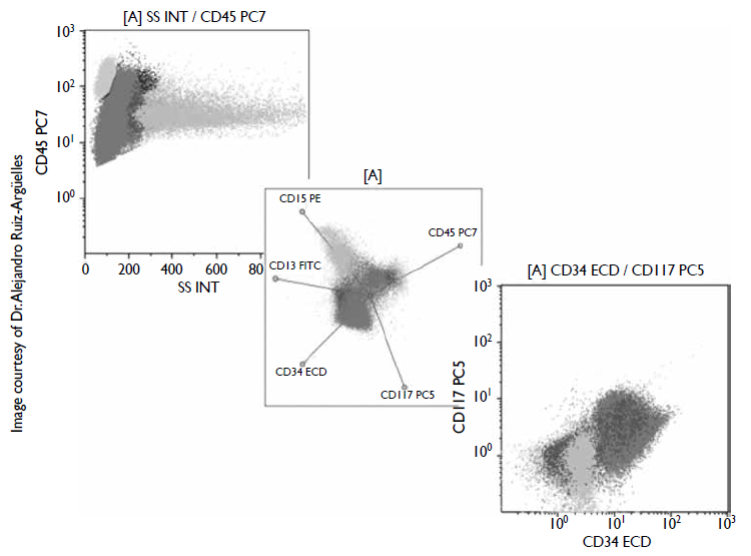
Figure I Bone marrow multiparametric flow cytometry from a patient with myeloid leukemia. Blasts (red) show bimodal expression of CD45 antigen and coexpression of CD34 and CD117 early antigens. Differing from normal granulocytes (green), blasts express very little CD13 and CD15 maturation antigens.