











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Congenital cystic adenomatoid malformation (CCAM) is a condition with different clinical presentations and is sometimes a little symptomatic. It occurs when bronchial dilations become infected or bleed. Among its characteristics, abnormal dilation of the airways with mucous cell proliferation stands out, leading to the appearance of cysts1. Given their congenital origin, some symptoms can appear during gestation, in the 1st h after birth and the first 2 years of life. In the pre-school stage, it manifests itself by repeated infections; thus, the differential diagnosis must be made to rule out bronchiectasis or other suppurative lung diseases2-4; in some cases, the presentation may take place later on5. This alteration of lung development was initially described by Civin and Tang in 1949, who observed certain pseudoglandular lung developments in stillbirths and premature newborns with hydrops, which refers to generalized subcutaneous edema with an accumulation of fluid in pulmonary cavities1,6.
Clinical case
A 19-year-old male patient with the genetic load by maternal inheritance for diabetes mellitus and systemic hypertension, smoker since the age of 15, at a rate of five cigarettes/day, who denied having any chronic degenerative diseases.
His condition began 2 months before admission, with unchecked fever, mostly in the mornings, which was partially subsided by the administration of oral antipyretics, with worsening of his overall condition, as well as coughing fits with purulent sputum. The patient received antimicrobial-based medical treatment, presenting no fever 3 weeks after the treatment onset. Subsequently, the patient began with pleuritic chest pain in the right hemithorax of moderate intensity. Hence, chest radiography was performed, where three cystic images of variable diameters were observed.
In the physical examination of the right hemithorax, there was a decrease in vocal vibrations, minor dull, or thud-like lung sounds and a decrease in respiratory sounds at the interscapular vertebral space in its middle portion, coarse crackles, 92% saturation in ambient air, and the remainder of his physical examination without alterations. Respiratory function tests within age, sex, weight, and height parameters.
Regarding radiological studies, a cystic image was observed, of approximately 6 cm in diameter in the right hilar region, heterogeneous opacity of defined edges with some cystic areas, triangular going from the right hilum to the diaphragm with a negative silhouette. The right lateral radiograph shows a radiolucent image with defined edges occupying the posterior region, showing a hydroaeric level in one of the cystic images. The tomographic section shows a well-circumscribed posterior image on the right side, more or less homogeneous with some radiolucent areas, and some cystic images. No vessels within the images or abnormal vessels were observed with the contrast medium.
Clinical and radiological data were presented, and the right lower lobectomy was performed without any surgical contraindications, which was carried out without problems. The presence of cysts with purulent sputum was confirmed, with bronchiolar lung tissue and dilated alveoli, lined with ciliated pseudostratified columnar epithelia, and no malignancy data. The other lung tissues had a normal structure. However, it was decided, due to the patient’s age, good previous lung function, and integrity of the remaining parenchyma, to perform the lobectomy (Fig. 1).
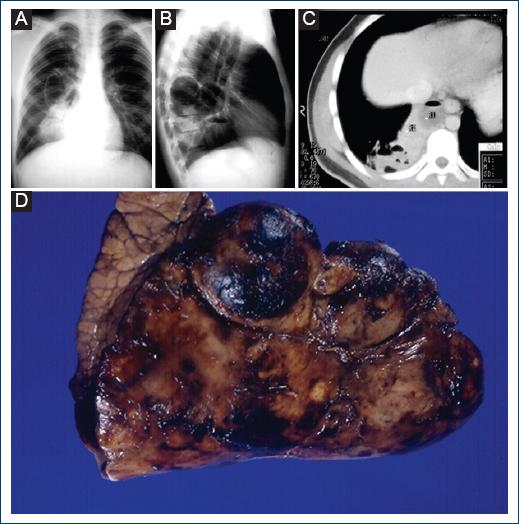
Figure 1 A: chest X-ray with a cystic image of 6 cm in diameter and heterogeneous opacity of defined edges with cystic zones, going from the hilum to the diaphragm with negative silhouette sign. B: radiolucent image with defined edges in the posterior region and hydroaeric level. C: computed tomography scan shows a posterior circumscribed image on the right side with radiolucent areas and cystic images. D: resected lung lobe, where multiple cystic images of different sizes are observed.
The patient’s condition improved and was discharged. The patient visited the outpatient clinic for follow-up with a good clinical evolution without presenting any recurrences.
Discussion
CCAM is a benign lung lesion, in which patients are presented with symptoms since childhood. Conversely, when patients can reach adolescence or adulthood, with this condition being undetected. Patients can present symptoms of respiratory infection, sometimes hemoptysis. These last two conditions make early diagnosis and treatment important, as the infection can affect other areas of the lung, with the development of the chronic pulmonary disease, which can be serious and may lead to greater complications and even death.
CCAM is a sporadic non-hereditary disease associated with genetic syndromes such as trisomy 18 and hereditary renal dysplasia; its pathogenesis is still unknown, apparently, there is a failure in the interaction of the endoderm with the mesoderm, or due to lack of irrigation or an imbalance between cell proliferation and apoptosis during lung development1-3,7.
This disease is classified into three types (Table 1). In this study, the patient was an adolescent without respiratory disease history, presenting symptoms 2 months before admission. An X-ray was taken, in which a circumscribed image was observed. Thus, a chest computed tomography (CT) scan was requested, where it was evidenced that the disease was limited to the lower lobe and was a Type I cystic adenomatoid disease. A lower lobectomy was performed, as this procedure ensured good residual lung function, and major complications such as recurrent pneumonia, chronic suppurative lung disease (CSLD), and hemoptysis would be avoided1,2,8,9. The calculated loss of lung function from a lobectomy is only 10%, which does not compromise the patient’s function. Therefore, without smoking or exposure to other pneumotoxic agents, the patient will lead a normal life10,11.
Table 1 Classification of congenital cystic adenomatoid malformation5,12
| Type I | One or more cysts of 2 cm or more, lined with ciliated pseudostratified columnar epithelia, surrounded by elastic tissue, smooth muscle bands, fibrovascular membranes, and cartilage. Alveoli with normal characteristics between the cystic structures. This type corresponds to 60-70% of cases. |
| Type II | Multiple cysts of uniform size, smaller than 2 cm, with terminal bronchioles of aberrant architecture between structures similar to large alveoli. They consist of a columnar or cuboidal epithelial wall surrounded by a thin fibromuscular layer and rarely have cartilage. It constitutes 20 to 30% of the cases; 50% associated with extra lobar pulmonary sequestration (ELS). |
| Type III | Voluminous solid mass, consisting of millimeter-like structures similar to bronchioles, separated by masses of alveolar type structures of cuboidal epithelium. It corresponds to 10% of cases. |
Associated malformations, especially those of Type II, are observed in up to 42% of patients, such as genitourinary disorders, renal agenesis, and Potter syndrome. Malformations are related to cardiovascular abnormalities in 21% of patients (persistence of the ductus arteriosus, dextrocardia, and among others), rib cage malformations in 16% of patients (pectus excavatum), and other malformations in 5% of patients. These include pyloric stenosis, pulmonary hypoplasia, diaphragmatic hernia, hydrocephalus, jejunal atresia, and Pierre-Robin syndrome that consist of micrognathia and glossoptosis and accompanied by a cleft lip and palate, as well as lesions of the hard and soft palate, high-arched palate, or the presence of hemi-vertebrae7,12,13. It is suggested that for cases of adenoid cystic malformation, genitourinary disorders should be investigated due to the possibility of association with alterations at this level12,13.
As for the differential diagnosis in children, diseases such as diaphragmatic hernia, where the presence of abdominal viscera is found in the thoracic space, pulmonary sequestration that can be differentiated from CCAM, because pulmonary sequestration receives the blood supply from an accessory artery of the aorta, which can observed by Doppler ultrasound. In addition, bronchogenic cysts that are most commonly located in the mediastinum and carina, and congenital lobar emphysema commonly associated with congenital heart disease. Lesions in children with one or multiple cysts of 5 mm or more in diameter have a better prognosis, allowing treatment in utero, by means of thoracentesis (fluid aspiration) or lobar resection, which reduces the risk of pulmonary hypoplasia2,6,9,14. Endobronchial obstructive infections or causes and mass lesions can be completely ruled out by clinical-radiological findings or by bronchoscopy2,14.
These cases are commonly diagnosed during childhood, as patients are presented with some symptoms from an early age. In the case under study, the patient had symptoms, as reported, up to the age of 19. Subsequently, the patient remained asymptomatic, a situation that is very significant, as the manifestation of CCAM is more frequent in children under the age of two6,7.
The diagnosis can be supported by imaging studies, which can initially be a diagnostic suspicion, by means of a simple chest X-ray, where a radiolucent image can be seen that may lead to a diagnostic suspicion and rule out other diseases. With this diagnostic suspicion, a chest CT scan should be requested, as it allows a clearer view of the lesions, their extension, the involvement with adjacent structures, and their relationship with the pulmonary and systemic circulation so that the diagnosis can be refined.
A differential diagnosis with radiological imaging in patients is related to cases of patients with giant bronchiectasis, as in some types of bronchiectasis, they tend to form cysts that are histologically different from this disease, but unlike adenomatoid disease, bronchiectasis is a CSLD15.
There are reports, in which they have found different types of the disease in the area of the affected lung. However, this does not affect the decision regarding the type of surgical procedure chosen for each case. The lesions in the case under study were confined to a large part of the lower lobe; thus, lower lobectomy was the procedure of choice. Large lesions are associated with hypoplasia of ipsilateral or contralateral lung lobes, and no predilection for a particular site of the lung parenchyma has been described7,16.
In our review for the present case, we found few reports regarding the association of adenocarcinoma with the cystic adenomatoid disease. However, in reality, there are so few cases that we cannot say that the latter alone is a risk for cancer9. Malignancy of the cystic lesion, leading to rhabdomyosarcoma or pleuropulmonary blastoma, is reported in some cases, which occurs for Type I in < 1%6,8,11.
Conclusion
CCAM is a rare pathology that must be taken into account from gestation to birth, as well as being a differential diagnosis for other congenital diseases that affect the chest. Once the diagnosis is made, the possibilities for resolution are high, which will depend on the type of involvement according to its classification. This includes searching for other alterations in other apparatuses and systems. Overall, the prognosis is good, and no hereditary pattern has been found. In the reported case, the late onset of the disease was observed in a 19-year-old male patient with a good post-operative evolution.

