











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Multiple myeloma could be considered as the malignant counterpart of plasma cells in which there is cell proliferation with multiple organic involvement, with particular affinity for bone and bone marrow.1 It represents 1% of all cancers and 10% of hematological cancers, which is why it ranks second in this group. The average age of diagnosis is 65 years. There is a predominance in males and the incidence is double in African-American patients compared to Caucasians. The most recent update of the criteria of the International Myeloma Working Group (IMWG) postulates that the diagnosis requires three of the following components: > 10% of monoclonal plasma cells in bone marrow and/or a biopsy with evidence of plasmacytoma; serum and/or urinary monoclonal protein and have at least one of the «CRAB» criteria: calcium elevation, renal failure, anemia or lytic bone lesions greater than 5 mm.2 Up to 80-90% of cases will have skeletal involvement.3 The spine is the most frequently involved site, affecting up to 60% of patients at presentation and up to 15-30% of patients developing new lesions in late stages. For this association, the spine specialist must have a clear understanding of this entity and include it in differential diagnoses during the systematic approach of the patient with vertebral destruction syndrome, since early recognition and timely multidisciplinary intervention will improve the patient’s functional prognosis and will impact your quality of life. The purpose of this study is to describe the clinical characteristics at the presentation of patients with histological diagnosis of multiple myeloma, as well as to detail the diagnostic and treatment algorithm used, from the moment of presentation to the decision of a definitive treatment.
Material and methods
A retrospective, descriptive and cross-sectional design study was carried out in the period from March 2012 to February 2017 with the authorization of the hospital’s research and ethics committee under code CEI-29-16. A review was made of the electronic files of patients with a diagnosis of vertebral destruction syndrome who were referred to the Spine Surgery Service of a third-level care center, including only those patients with a histological diagnosis of multiple myeloma. In addition to demographic data, clinical information was sought: presence of pain, ASIA scale and categorized according to the Durie-Salmon classification at diagnosis; levels involved and type of surgery.
Diagnostic algorithm
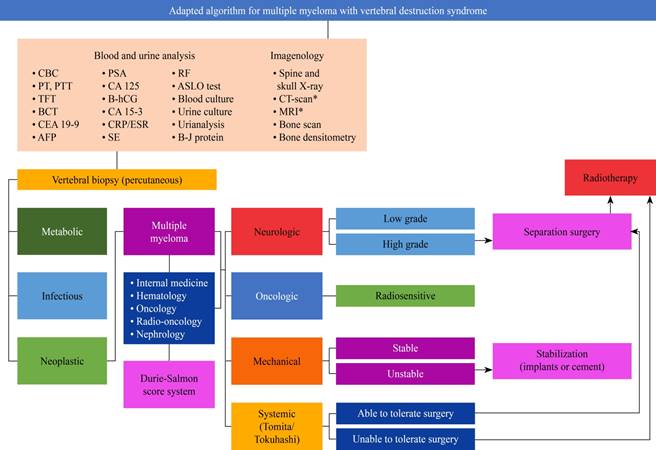
All patients attended by the hospital’s spinal service for vertebral destruction syndrome require completing the protocol described by Alpizar-Aguirre et al. and modified by our institution, which includes a series of serum and urine tests; Conventional radiographs, magnetic resonance imaging, computed axial tomography and bone scan. After an analysis of these elements, a biopsy of the spinal tissue involved is performed.4 This allows us to increase the sensitivity of our diagnostic approach by differentiating between the three etiologies of vertebral destruction: infectious, metabolic, and neoplastic. After having a histological diagnosis, the patient is sent to the internal medicine, hematology, oncology and radio-oncology service to provide medical treatment, prognosis and multidisciplinary follow-up. In the case of patients with multiple myeloma, the staging described by Durie-Salmon5 (Figure 1) is used and additionally it refers to the nephrology department. After this comprehensive assessment, the joint decision is made in accordance with the NOMS reference framework (Neurologic, Oncologic, Mechanical, and Systemic),6 the most appropriate definitive surgical treatment with the least possible morbidity. This allows the management of the increasingly frequent population with spinal cord compression due to malignancy (CMEM) to be standardized. The algorithm used is presented (Figure 2).
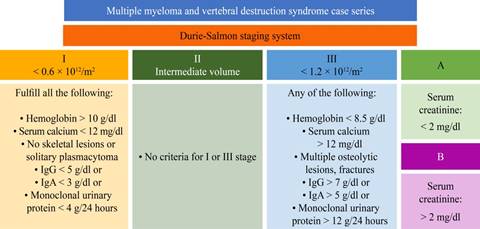
Modified from: Durie BG, et al.5
Figure 1: Durie-Salmon clinical staging system. Clinical criteria to estimate the spread of neoplastic cells in multiple myeloma.
BH = complete blood count; TP = prothrombin time; TTP = thromboplastin time; PFT = thyroid function tests; QC 6 = clinical blood chemistry of 6 elements; AFP = alphafetoprotein; APE = prostate specific antigen; B-hCG = fraction B human chorionic gonadotrophin; PCR/ESR = C reactive protein and erythrocyte sedimentation rate; SE = serum electrolytes; RF = rheumatoid factor; EGO = general urine test; B-J = Bence-Jones protein; CAT = computerized axial tomography; MRI = magnetic resonance imaging. * Simple and contrasted.
Figure 2: Proposal of management algorithm used.
Results
Ten patients with histological diagnosis of vertebral multiple myeloma were included in the study period obtained by the spine surgery service, with an average age of 61.4 years (49 to 83). 30% women and 70% men. All the patients were approached with the modified protocol of the vertebral destruction syndrome described and subsequently underwent percutaneous biopsy. All presented axial pain at some point in the evolution. At diagnosis 60% had an incomplete spinal cord injury classified as ASIA D, 30% were in ASIA A and only in one patient was there integrity with ASIA E. The patients were categorized according to the Durie-Salomon stages for multiple myeloma, half of the patients were in stage III, 40% in stage II and only one patient was classified as I. Anemia was diagnosed in 60% of the patients, of these four patients with hemoglobin levels below 7.5 g/dl. One patient was diagnosed with kidney failure. Two patients had hypercalcemia.
Of the total number of patients, there were 17 vertebrae involved. The most frequently affected segment was the thoracic with 59% (n = 10) of the total vertebrae. Followed by the lumbar with six vertebrae and the sacrum with a vertebra involved at this level.
The distribution of levels affected by patient was variable, half of the patients presented with only one vertebral level involved. 4 patients 2 levels and only one patient with 4 levels involved.
After multiple myeloma diagnosis by fluoroscopy-guided percutaneous biopsy in all the patients, they were sent to the oncology service where they received hematological medical treatment and subsequently underwent a surgical procedure according to the NOMS reference framework in 9 of them. Fusion with posterior instrumentation was performed in 8 patients; in 6 of them, vertebroplasty was additionally performed. Only in one patient was vertebroplasty used as the only form of definitive treatment. The summary of the series is presented in (Table 1).
Table 1: Case series characteristics.
| Multiple myeloma and vertebral destruction syndrome case series | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age | Gender | Axial pain at diagnosis | ASIA | Durie-Salmon | Serum hemoglobyn (g/dl) | Serum creatinine (mg/dl) | Serum calcium (mg/dl) | Affected level | Surgery |
| 76 | F | Y | D | 3 A | 7.0 | 0.4 | 9.6 | T12 | Fusion |
| 31 | M | N | E | 1 A | 15.9 | 1.0 | 8.3 | C2 | Vertebroplasty-fusion |
| 54 | M | Y | D | 2 A | 14.0 | 0.8 | 8.0 | L3 | Fusion |
| 54 | M | Y | D | 2 A | 13.9 | 1.0 | 9.0 | T2, S1 | Biopsy |
| 53 | F | Y | A | 2 A | 12.2 | 0.4 | 8.0 | T9, T10 | Vertebroplasty + fusion |
| 49 | M | Y | A | 2 A | 15.1 | 0.6 | 9.8 | T4, T5 | Fusion |
| 67 | F | Y | E | 3 A | 6.3 | 1.2 | 9.4 | L1 | Vertebroplasty + fusion |
| 64 | F | Y | D | 3 A | 7.4 | 1.9 | 10.6 | L1 | Vertebroplasty + fusion |
| 60 | M | Y | E | 3 A | 10.0 | 0.8 | 8.0 | T3, T5, T7 | Vertebroplasty + fusion |
| 56 | M | Y | D | 3 B | 7.9 | 2.1 | 14.0 | L3, L4 | Vertebroplasty |
M = male, F = female; Y = yes, N = no.
Discussion
The association of multiple myeloma with vertebral lesions is classically described in the literature. In a series of 1027 patients, Kyle et al reported that radiographic bone abnormalities were found at some point in the disease in 84% of the patients, such as lytic lesions, pathological fractures, vertebral compression fractures and osteopenia.7 Most of these injuries affect the vertebral body, but they can be found in posterior bony elements: facets, pedicles, transverse and spinous processes. Weakness results in asymmetric vertebral wedging with potential compromise of spinal stability and neurological function,8 since multiple myeloma has been reported to be one of the most frequent causes of CMEM, being responsible for up to 11.1% of hospitalizations for this complication in the United States, only two places behind lung cancer (24.9%) and prostate cancer (16.2%).9
In the presented series, all patients obtained a first-time diagnosis and began their study by a spinal surgery service at a third-level center. Most had some degree of spinal compression at the time of initial assessment. It is not uncommon for the initial presentation of this neoplasm to include spinal compression. In the Benson et al series, 66% of patients with multiple myeloma presented with paraplegia, which in most were preceded by axial pain, sensory deficit, or progressive paraparesis.10 For the spinal surgeon treating a patient with vertebral destruction, it is advisable to have systematized management methods. The spectrum of differential diagnoses is very broad and includes, in addition to primary and metastatic neoplasms, simulatory processes such as infections and injuries due to metabolic diseases. Standardized diagnostic approaches that cover the different causes, such as the previously used modification, will allow identifying the disease that is being faced and consequently making better decisions.
Once a primary or metastatic tumor has been identified, the degree of compression and the presence of instability should be considered and evaluated. A reproducible method for the latter is the Spinal Instability in Neoplastic Disease (SINS) classification system that defines whether the patient requires stabilization,11 either with fusion or with vertebral augmentation. If you are a suitable candidate or not, will depend on your general condition. There are objective evaluations for this purpose in the literature, such as the Tomita12 and Tokuhashi13 scores that help to make an individualized decision, based on evidence and in conjunction with a multidisciplinary medical-surgical team, the patient and their family members. Although implant fusion surgeries still play a role as stabilizing procedures, their large approaches lead to greater morbidity and complications in immunologically and nutritionally disadvantaged patients, which has allowed exploring less invasive alternatives. With the development and refinement of minimal invasive spine surgery (MISS) techniques, its field of application is expanding and CMEM is no exception. Kyphoplasty, percutaneous vertebroplasty alone, and their combination with radiofrequency ablation have been shown to reduce pain, improve mobility, and provide stability to vertebral bodies affected by multiple myeloma.14 These methods of vertebral augmentation have proven to be true stabilization methods for the anterior and medial spines, and have shown encouraging results in pain control in combination with radiofrequency.15
Although a review of hematological medical management is beyond the objectives of this work, the role of radiotherapy should be highlighted, since multiple myeloma is classically considered a radiosensitive tumor. The use of radiosurgery has shown to improve pain in up to 41% of patients in a period of 1.6 months, however, close radiological follow-up by the spinal specialist is necessary since its association with instability complications with a cumulative incidence for radiographic failure at 6 and 12 months, of 6% and 9% respectively; and a cumulative risk of vertebral fracture of 18% at 6 and 12 months.16 In general, the use of radiation therapy should be limited as much as possible to avoid worsening the already diminished bone marrow production. Patients who benefit from radiosurgery are those with soft tissue tumors or plasmacytomas who have not responded to systemic therapy, patients who cannot receive systemic therapy, refractory to treatment, as a palliative measure in patients with poor functional states, severe pain associated with effect of tumor mass or in the case of patients who will undergo procedures of vertebral augmentation with cement in which a decrease in tumor volume is required. With the development of better non-invasive techniques and pharmacological measures, the quality and expectation of patients has had a positive impact.
The chapter on vertebral metastasis disease has seen a dizzying and contrasting evolution over more than 40 years, with different controversial works that have resulted in algorithms or frames of reference that seek to facilitate decision-making.17 A review of these simplified methods and a deep understanding of current oncological concepts applied to the surgical field should not be neglected.
Conclusions
The participation of the spine surgeon in the medical and surgical management of patients with multiple myeloma is very active in different stages of the disease: from the presentation, at the final diagnosis, in the care of complications throughout the natural evolution of the disease or inherent in therapeutic methods. The use of systematized management algorithms will allow better decisions to be made in conjunction with a multidisciplinary group for the care of multiple myeloma with vertebral involvement.

