










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista odontológica mexicana
Print version ISSN 1870-199X
Rev. Odont. Mex vol.20 n.4 Ciudad de México Oct./Dec. 2016
https://doi.org/10.1016/j.rodmex.2016.11.004
Original research
Effectiveness of trichoroloacetic acid in treatment of focal epithelial hiperplasia lesions
*DDS, MS in Molecular Microbiology, Specialist in Surgery and Stomatology, Teacher, University Corporation Rafael Nuñez, Colombia.
§ DDS, M Sc in Education, Specialist in Stomatology, Full Professor at the University of Cartagena, Colombia.
|| DDS, PhD in Biomedical Sciences, M Sc in Education, Specialist in Periodontics, Full Professor at the University of Cartagena Colombia.
Objective:
The aim of the present study was to assess effectiveness of trichloroacetic acid therapy in the treatment of oral lesions produced in focal epithelial hyperplasia cases.
Material and methods:
In the present study 11 patients were included. Patients exhibited clinical and histopathological characteristics of focal hyperplasia and were willing to participate in the study. Convenience sampling was executed in patients attending clinical consultation at the Dental Clinic of the Rafael Nuñez University Corporation and the University of Cartagena. Patients underwent excision biopsy in one of the lesions so as to establish anatomical-pathological diagnosis. Subsequently, 80% trichloroacetic acid was applied every two weeks on the lesions, until lesions disappeared.
Results:
Out of 11 pediatric patients 63.64% were female, average age nine years. Locations of greater involvement in the mouth were upper and lower labial mucosa (representing 100%). Anatomical-pathological study revealed in all cases presence of epithelial acanthosis, papillomatosis and koilocytiosis. The greatest number of acid applications was three and four episodes with 27%, average time for lesion disappearance was 61.3 days. No relapse was observed in 100% of cases.
Conclusion:
Trichloroacetic acid application in focal epithelial hyperplasia cases is an effective technique which achieves rapid, atraumatic stress-free lesion resolution which did not generate fear in involved patients.
Key words: Trichloroacetic acid; focal epithelial hyperplasia; papillomavirus infections
Propósito:
El propósito del estudio fue evaluar la efectividad de la terapia con el ácido tricloroacético en el tratamiento de las lesiones orales producidas en la hiperplasia epitelial focal.
Material y métodos:
Se incluyeron 11 pacientes que presentaron características clínicas e histopatológicas de hiperplasia epitelial focal y que aceptaron participar en el estudio, se aplicó muestreo por conveniencia, en pacientes que asistieron a consulta de la clínica odontológica de la Corporación Universitaria Rafael Núñez y la Universidad de Cartagena, se les realizó biopsia excisional en una de las lesiones para establecer diagnóstico anatomopatológico, posteriormente se aplicó ácido tricloroacético al 80% sobre las lesiones cada quince días hasta que desaparecieron.
Resultados:
De un total de 11 pacientes pediátricos el 63.64% fueron de género femenino, promedio de edad fue nueve años, los sitios de mayor afección en cavidad bucal fueron mucosa labial superior e inferior representando un 100%, en el estudio anatomopatológico se describió la presencia de acantosis epitelial, papilomatosis y coilocitosis en todos los casos, el mayor número de aplicaciones con el ácido fue tres y cuatro veces con un 27%, el promedio de desaparición de las lesiones fue de 61.3 días, no se ha presentado recidiva en el 100% de los casos.
Conclusión:
La aplicación del ácido tricloroacético en la hiperplasia epitelial focal es una técnica efectiva, consiguiendo la resolución de las lesiones en forma rápida, poco traumática, sin generar ansiedad y temor en los pacientes.
Palabras clave: Ácido tricloroacético; hiperplasia epitelial focal; infecciones por papillomavirus
INTRODUCTION
Focal epithelial hyperplasia is a benign, chronic illness, mainly affecting children. It manifests in the oral mucosa and is caused by human papilloma virus. It is related to subtypes 13 and 32;1,2 it is common in North American native subjects. In Colombia it is mostly found in the Antioquìa and Chocó districts.3,4 It is clinically characterized by presence of multiple papules involving the whole of the oral mucosa. Lesions can be found in the gums, labial and buccal mucosa and the tongue. Lesions are asymptomatic and of variable size5,6
Histopathological study of lesions reveals formation of parakeratin layers and extensive acanthosis. Epithelial cells of the stratum spinosum show large nuclei with vacuolated cytoplasm indicating koilocyte degeneration.7,8
From a therapeutics perspective, the disease tends to exhibit spontaneous regression, and this regression can persist for 10 up to 30 years, which implies that patients will exhibit lesions during all their childhood, adolescence and part of their adult life. This situation might generate oral problems as well as psychosocial issues such as rejection.9,10 Treatment alternatives can be surgical excision, cryosurgery, 5% imiquimod and laser ablation. Nevertheless, all the aforementioned are trauma-inducing techniques, some are immunemodulating techniques, and might cause anguish, anxiety and fear in the patient.11,12
Trichloroacetic acid (TAA) is a favorable therapeutic option, it elicits little trauma or negative emotional reactions, nevertheless its use requires further study.13 TAA is chemically composed of carbon, chloride, oxygen and hydrogen. It causes denaturalization, precipitation and destruction of lesions by means of chemical coagulation of affected tissue. Clinically, certain flattening of the lesions can be observed.14 It is used for the treatment of vaginal infections caused by human papilloma virus in conditions such as papilloma, condyloma and common warts (verruca vulgaris). Suitable results are obtained when this acid is used at concentrations higher than 80%.15,16 Harris et al applied TAA in oral lesions of two pediatric patients; they observed lesion resolution with two topical applications.17 Leon et al reported two cases of patients affl icted with FEH (focal epithelial hyperplasia), who showed satisfactory results after being treated with TAA.18
The aim of the present study was to assess effectiveness of trichloroacetic acid therapy in treatment of focal epithelial hyperplasia.
MATERIAL AND METHODS
A prospective analytical study was conducted with an intervention component. Eleven patients were included in the study, according to population. Patients exhibited clinical and histopathological characteristics of focal epithelial hyperplasia and had previously signed informed consent forms. Convenience sampling was applied to patients attending dental services at the clinics of the Rafael Nuñez University Corporation and the University of Cartagena. Initially, an intraoral examination was conducted in subjects showing clinical impression of focal epithelial hyperplasia (Figure 1). Patients were subjected to incision biopsy in one of the lesions so as to establish anatomical and pathological diagnosis. At a later point, and following Beutner et al protocolol,19 80% trichloroacetic acid was applied.

To begin with, the area was cleansed with abundant water supply and the lesion surface was dried. After this, TAA was applied over the lesions with a hyssop; after 90 seconds the lesion acquired an intense white coloration due to the chemical burn caused by the acid (Figure 2). After this, a buffering substance was applied in the mouth, this substance was composed of water and sodium bicarbonate powder (soda) so as to neutralize the acid´s ph and to eliminate residues which might affect adjacent tissues. The process was repeated in all lesions every two weeks, until lesion disappearance (Figure 3).


The present work was adapted to the World Medical Association Helsinki recommendations for biomedical research, (Number 008430 (1993) resolution of technical, scientific and administrative norms) and was approved by the ethics research committee of the Rafael Nuñez University Corporation and the University of Cartagena.
Data statistical analysis was conducted using StrataTM version 12 for Windows statistical package. Description was made of treated patients’ data, central tendency and dispersion measures were used for quantitative variables and frequency distribution and qualitative variables proportions. Lesion resolution time was defined as main outcome (dependent variable).
RESULTS
Out of a total of 11 patients, 63.64% were female. Average age was 9.0 ± (SD:3.41). Most affected sites in the mouth were upper and lower labial mucosa in 100% cases, right and left oral mucosa in 63.64% cases, dorsal side of the tongue in 45.45% cases and lateral border of the tongue in 27.27% cases (Table I). Anatomical and pathological study revealed presence of epithelial acanthosis, papillomatosis and koilocytosis in 100% of cases.
Table I Case distribution according to gender, age, lesion location and evolution time.
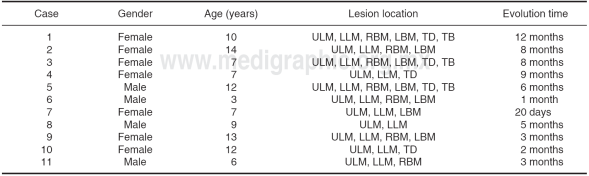
ULM = Upper labial mucosa, LLM = Lower labial mucosa, RBM = Right buccal mucosa, LBM = Left buccal mucosa, TD = Tongue dorsum, TB = Tongue border.
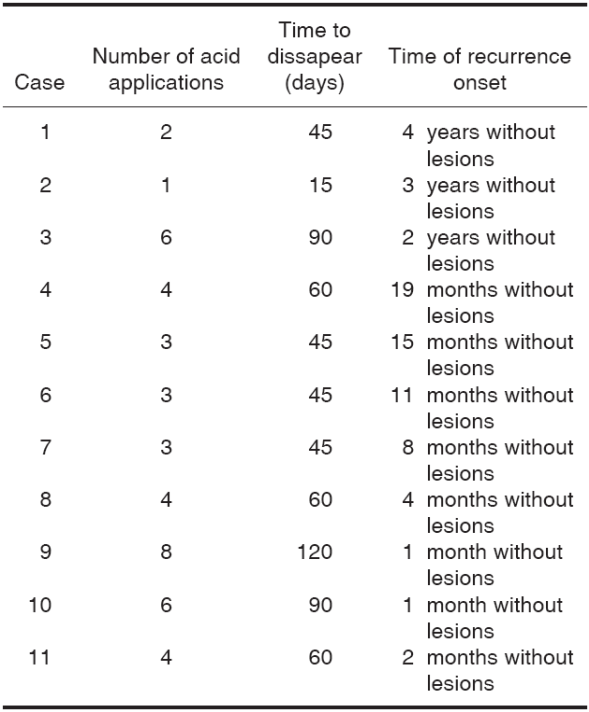
The greatest number of acid application was three and four times per case, representing 27%, with average of 4.0 ± (SD:2.0), lesion disappearance average was 61.3 days ± (SD:28.8) and relapse was not present in 100% of all cases (Table II).
Table II Lesion behavior with respect to number of applications, time of disappearance and recurrence.
With respect to symptoms, two patients manifested burning sensation after acid application during the first session, no complications such as ulcerative lesions, blisters or burns were observed.
DISCUSSION
Gonzalez et al and Hall et al described in their studies that FEH is characterized by the presence of multiple papules, which are commonly located in the labial and oral mucosa; they describe these lesions as asymptomatic, of variable size and matching the color of adjacent mucosa.19,20,21 Villanueva et al state that FEH frequently affects child population, and exhibits preference for the female gender;22 this concurs with the clinical characteristics exhibited in 100% of cases examined in the present study: 63.64% of total population was female, and age average was 9.0 years. Lopez et al and Gonzalez et al stated that in the histological study, the condition was characterized by presence of acanthosis, epithelial projections, papillomatosis, ovoid-shaped cells with increased cytoplasm and displaced nuclei also called koliocytes;23,24 all the aforementioned fully concurs with 100% of cases studied in the present report.
Leon et al reported two cases of patients affl icted with FEH in the upper and lower labial mucosa as well as the oral mucosa. Lesions were treated with 70% TAA in several sessions, favorable results were obtained.18 Little et al reported that FAA application in FEH cases was a therapeutic alternative offering suitable results; they recommend concentrations of 80 and 90%.25 The present study concurred with these appreciations since topical applications were performed with 80% TAA and favorable results were obtained. Average time for lesion disappearance was 61.3 days; only two patients experimented burning sensation after acid application in the first visit. No relapse was observed in 100% of all cases.
Mata et al applied TAA and cryotherapy to patients affl icted with FEH. They reported full lesion resolution after a two year follow-up,26 differing from the present study where average time for lesion resolution was 61.3 days with only 80% TAA topical applications.
CONCLUSIONS
Application of trichloroacetic acid as therapeutic method in focal epithelial hyperplasia was an effective technique, lesions were resolved in a rapid and atraumatic manner, without generating anxiety or fear. Lesions exhibiting greater diameter and height required more applications than those of smaller size.
REFERENCES
1. Ozden B, Gunduz K, Gunhan O, Ozden FO. A case report of focal epithelial hyperplasia (Heck's disease) with PCR detection of human papillomavirus. J Maxillofac Oral Surg. 2011; 10 (4): 357-360. [ Links ]
2. Oaunders NR, Scolnik D, Rebbapragada A, Koelink E, Craw L, Roth S et al. Focal epithelial hyperplasia caused by human papillomavirus 13. Pediatr Infect Dis J. 2010; 29 (6): 550-552. [ Links ]
3. Navarro L, Ordaz K, Lacruz B, More Y. Prevalencia de la hiperplasia epitelial focal en pacientes de las étnias Sanema y Yekuana. Estado Bolívar. Venezuela. Acta Odont Venez. 2006; 45 (3): 426-428. [ Links ]
4. Rodríguez GM, Guzmán YR, Tejada PA, Sánchez R, Rodríguez C. Percepción y experiencias frente a la hiperplasia epitelial focal en una comunidad indígena huitoto/ticuna del amazonas colombiano. Rev Fac Med. 2008; 56 (2): 101-108. [ Links ]
5. Borborema-Santos CM, Castro MM, Santos PJ, Talhari S, Astol? -Filho S. Oral focal epithelialhyperplasia: reportof?ve cases. Braz Dent J. 2006; 17 (1): 79-82. [ Links ]
6. Hashemipour MA, Shoryabi A, Adhami S, Mehrabizadeh Honarmand H. Extensive focal epithelial hyperplasia. Arch Iran Med. 2010; 13 (1): 48-52. [ Links ]
7. Gültekin SE, Tokman Yildirim B, Sarisoy S. Oral focal epithelial hyperplasia: report of 3 cases with human papillomavirus DNA sequencing analysis. Pediatr Dent. 2011; 33 (7): 522-524. [ Links ]
8. Puriene A, Rimkevicius A, Gaigalas M. Focal epithelial hyperplasia: Case report. Stomatologija. 2011; 13 (3): 102-104. [ Links ]
9. Regura R, Toro M, Ceballos A, Aparicio J, Fuentes H. Focal epithelialhyperplasia. a raredisease in ourarea. Med Oral Patol Oral Cir Bucal. 2005; 10 (2): 128-131. [ Links ]
10. Vera-Iglesias E, García-Arpa M, Sánchez-Caminero P, RomeroAguilera G, Cortina de la Calle P. Focal epitelial hyperplasia. Actas Dermosi?liogr. 2007; 98 (9): 621-623. [ Links ]
11. Said AK, Leao JC, Fedele S, Porter SR. Focal epithelial hyperplasia - an update. J Oral Pathol Med. 2013; 42 (6): 435-442. [ Links ]
12. Van der Voort EA, Arani SF, Hegt VN, van Praag MC. Focal epithelial hyperplasia of the oral mucosa. A unique manifestation of human papillomavirus. Ned Tijdschr Tandheelkd. 2009; 116 (3): 149-151. [ Links ]
13. Yanofsky VR, Patel RV, Goldenberg G. Genital warts: a comprehensive review. J Clin Aesthet Dermatol. 2012; 5 (6): 25-36. [ Links ]
14. Ficha de Datos de Seguridad Según Reglamento (CE) 1907. Citado 2006. www.panreac.com/new/esp/fds/esp/X151067.htm [ Links ]
15. Taner ZM, Taskira C, Onan AM, Gursoy R, Himmetoglu O. Therapeutic value of trichloroacetic acid in the treatment of isolated genital warts on the external female genitalia. J Reprod Med. 2007; 52 (6): 521-525. [ Links ]
16. Pezeshkpoor F, Banihashemi M, Yazdanpanah MJ, Yousefzadeh H, Sharghi M, Hoseinzadeh H. Comparative study of topical 80% trichloroacetic acid with 35% trichloroacetic acid in the treatment of the common wart. J Drugs Dermatol. 2012; 11 (11): 66-69. [ Links ]
17. Harris Ricardo J, Rebolledo Cobos M, Carmona Lorduy M. Ácido tricloroacético como terapéutica en dos casos de hiperplasia epitelial focal. Acta Odont Venez. 2011; 49 (3): 1-11. [ Links ]
18. León L, Cubilla E, Guzmán A, Mendoza G, Celias L, Arenas R y cols. Hiperplasia epitelial multifocal. Reporte de dos casos relacionados con VPH-13. DCMQ. 2012; 10 (4): 256-259. [ Links ]
19. Beutner KR, Wiley DJ, Douglas JM, Tyring SK, Fife K, Trofatter K. Genital warts and their treatment. Clin Infect Dis. 1999; 28 (1): 37-56. [ Links ]
20. González-Losa MR, Suarez-Allén RE, Canul-Canche J, CondeFerráez L, Eljure-Lopez N. Multifocal epithelial hyperplasia in a community in the Mayan area of Mexico. Int J Dermatol. 2011; 50 (3): 304-309. [ Links ]
21. Hall C, McCullough M, Angel C, Manton D. Multifocal epithelial hyperplasia: a case report of a family of Somalian descent living in Australia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010; 109 (1): 20-24. [ Links ]
22. Villanueva Álvarez-Santullano CA, Hernández-Núñez A, Castaño A, Miñano Medrano R, Córdoba Guijarro S, BorbujoMartínez J. Multifocal epithelial hyperplasia: a familial case. An Pediatr (Barc). 2010; 73 (6): 357-360. [ Links ]
23. López-Jornet P, Camacho-Alonso F, Berdugo L. Oral focal epitelial hyperplasia. N Y State Dent J. 2010; 76 (4): 54-55. [ Links ]
24. González LV, Gaviria AM, Sanclemente G, Rady P, Tyring SK, Carlos R et al. Clinical, histopathological and virological ?ndings in patients with focal epithelial hyperplasia from Colombia. Int J Dermatol. 2005; 44 (4): 274-279. [ Links ]
25. Little J, Falace D, Miller C, Rhodus N. Dental management of the medically compromised patient. 5th Ed. mosby. 1998. pp. 319, 320. [ Links ]
26. Mata M, Fermín Y, Oliver M, Rondón A. Focal epithelial hyperplasia: report of four cases. Dermatol Venez. 1996; 34 (1): 29-32. [ Links ]
***This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam
Received: May 01, 2015; Accepted: January 01, 2016
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
