











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkA 22-year-old woman with history of heart murmur diagnosed in childhood was referred from a general hospital with dizziness, palpitation, and worsening of dyspnea (NYHA III).
Transthoracic echocardiography (TTE) revealed large atria with supramitral, non-restrictive membrane that extends from the mitral annulus to the lower portion of the left atrial appendage (Fig.1 A-B, red.arrow. Video S1). Mitral valve showed thickened leaflets, both leaflets inserted into anterolateral papillary muscle, and hypoplastic posteromedial papillary muscle was present, so a parachute mitral valve was described. The Doppler demonstrated significant mitral stenosis (mean gradient 17 mmHg, and valve area 0.5 cm2) (Fig.1 C). Type I bicuspid aortic valve without raphe (Fig.1 E), non-restricted subaortic membrane (Fig.1 D, yellow. arrow. Video S2), aortic coarctation with gradient 28 mmHg and non-diastolic prolongation, preserved left ventricular systolic function, and tricuspid regurgitation gradient 52 mmHg were additional findings. Transesophageal echocardiography confirmed TTE diagnosis.
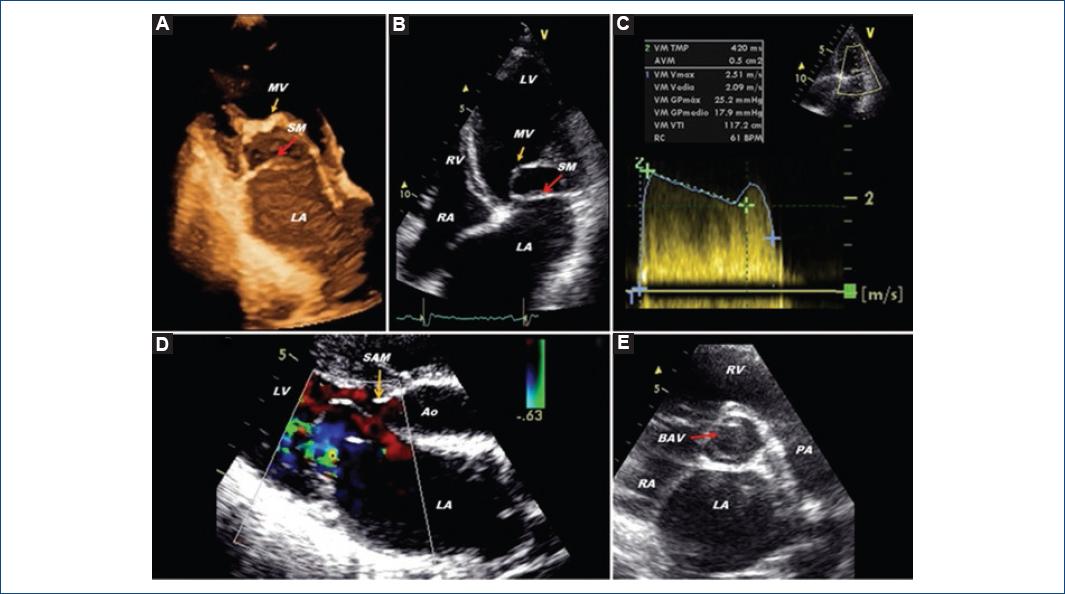
Figure 1 Transthoracic echocardiography. A: apical three-chamber view; B: apical four-chamber view; C: continuous Doppler, mitral valve gradient; D: parasternal long-axis color Doppler; E: parasternal short-axis view of aortic valve.BAV: bicuspid aortic valve; SM: supramitral membrane; MV: mitral valve; SAM: subaortic membrane; Ao: aorta; RA: right atrium; LA: left atrium; RV: right ventricle; LV: left ventricle; PA: pulmonary artery.
Cardiac catheterization showed pulmonary capillary wedge pressure 35 mmHg, transmitral gradient 10 mmHg, mean pulmonary pressure 47 mmHg, and non-significant aortic coarctation gradient (13 mmHg).
Surgery revealed supramitral membrane, anterior commissure fusion, and posterior mitral leaflet traction to anterolateral papillary muscle due to chordae tendineae. For those reasons, mitral commissurotomy was performed, supravalvular mitral membrane resection and mitral annuloplasty. Three months after the surgery, TTE showed a mean mitral gradient of 10 mmHg, and the treadmill exercise test demonstrated an improvement in the functional class (> 8 metabolic equivalents [METS]).
Shone’s syndrome is a rare congenital anomaly of the mitral valve, and the survival is hardly ever until adulthood. There are different treatment techniques; one of them is the mitral plasty. Echocardiography is an excellent non-invasive method to establish the correct diagnosis.1-4
Supplementary data
Supplementary data are available at Revista Archivos de Cardiología de México online (http://www.archivoscardiologia.com/frame_esp.php?id=9). These data are provided by the corresponding author and published online for the benefit of the reader. The contents of supplementary data are the sole responsibility of the authors.

