










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
 Cited by SciELO
Cited by SciELO Related links
 Similars in
SciELO
Similars in
SciELO Share

 Permalink
PermalinkFrontera norte
On-line version ISSN 2594-0260Print version ISSN 0187-7372
Frontera norte vol.19 n.37 México Jan./Jun. 2007
Artículos
Compromised Birth Outcomes among Mexican-Origin Population at the U. S.-Mexico Border
Raúl S. González R.*
* Professor-researcher, El Colegio de la Frontera Norte. E-mail: raul@colef.mx.
Date of receipt: October 7, 2005.
Data of acceptance: June 5, 2006.
Abstract
This research on ethnicity, risk factors, and birth outcomes among women of Mexican origin along the U. S.-Mexico border in the state of Texas includes a review of the Hispanic epidemiologic paradox. The study uses a framework that delineates the sociodemographic and biomedical factors that help to explain birth-outcome characteristics for Mexican-origin mothers. Data from a large hospital in El Paso, Texas, is analyzed to determine the frequency of, and the reasons for, birth-outcome disparities in Mexican-origin women from different backgrounds who are residing in the United States.
Keywords: Hispanic epidemiologic paradox, birth outcomes, Mexican-origin population, U. S.-Mexico border; El Paso, Texas.
Resumen
Esta investigación sobre etnicidad, factores de riesgo y natalicios entre mujeres de origen mexicano en la frontera México-Estados Unidos en el estado de Texas, incluye una revisión de la paradoja epidemiológica hispana. Se utiliza un marco de referencia que delimita los factores sociodemográficos y biomédicos que son de utilidad para explicar las características de natalidad en madres de origen mexicano. se analizan datos de un hospital general en El Paso con el fin de determinar las razones y la frecuencia de disparidades natales entre madres de origen mexicano que tienen diversos antecedentes y viven en Estados Unidos.
Palabras clave: paradoja epidemiológica hispana, características de los nacimientos, población de origen mexicano, frontera México-Estados Unidos, El Paso Texas.
INTRODUCTION
This article reports on research on the relationship between birth outcomes and nationality/language at a site along the U. S.-Mexico border. A diverse set of women's socioeconomic and demographic characteristics, as well as behavioral and health factors are analyzed in terms of their impacts on birth outcomes, using data from a hospital in El Paso, Texas.
Birth outcomes are an excellent marker for infant health and survival probabilities as well as subsequent child health. The health of newborn infants is the subject of numerous empirical studies due to its strong association with infant mortality (neonatal and post-neonatal), congenital anomalies, and later childhood outcomes, such as developmental delays, disabilities, attention-deficit hyperactivity disorder (ADHD), and poor educational achievement (Albrecht et al., 1996; Thompson et al., 2003; Bhutta et al., 2002). An infant's birth weight is one variable that determines a child's health.
In 1950, the World Health Organization (WHO) designated births of <2 500 g as a standard for prematurity. Since that time, this limit has been established as a critical value for a newborn's probability of survival. An upper limit for compromised birth weight has not been established, although it is known that infants born to women with diabetes usually present birth-weight-related problems.
Many U. S. studies have used sociodemographic and socioeconomic variables to address disparities in the health of specific populations. An important one is race/ethnicity, a socially constructed variable based mainly on infant's country of birth, maternal country of birth, skin color, and even surname (Forbes and Frisbie, 1991; Fuentes-Afflick et al., 1997; Palloni and Morenoff, 2001; Hummer, 1993; Hummer et al., 1999; Singh and Yu, 1996; Scribner, 1996; Palloni and Arias, 2004). The literature on birth outcomes usually differentiates White (also called non-Hispanic White), African-American, Hispanic, Asian-American, and Native-American populations. Most frequently, studies compare these groups across one or more health-status aspects, employing sociodemographic and socioeconomic variables as explanatory factors.
Over the last three decades, literature on the so-called Hispanic epidemiologic paradox has been an important subset of this body of work. This paradox arises because the Hispanic population, despite having an overall low socioeconomic profile and less access to healthcare than the majority population, exhibits a lower infant mortality rate than does the population of non-Hispanic Whites (Forbes and Frisbie, 1991; Frisbie et al., 1996; Palloni and Morenoff, 2001). Some studies have shown that this pattern is also valid for adult mortality (Hummer et al., 2000; Sorlie et al., 1993). Moreover, certain studies have shown that within ethnic groups, foreign-born women have better birth outcomes than do U. S.-born women (Kelaher and Jessop, 2002; Singh and Yu, 1996). That aspect of the epidemiologic paradox—more favorable outcomes among the foreign-born—is one of the key health patterns examined in this article.
NATIVITY AND LENGUAGUE
Maternal birthplace and language appear to be associated with birth outcomes. Infants whose mothers were born in Mexico present lower rates of low birth weight than do infants born to Mexican-American women. English et al. (1997) concluded that Mexican nativity of the mother constitutes a significant protective factor against low birth weight in the child. Singh and Yu (1996) established that a mother's Mexican nativity may serve as an important differentiation axis for birth outcomes. Crump et al. (1999), in a study of birth outcomes in the state of Washington, found that U. S.-born Mexican-American mothers had a higher risk for preterm birth than did Mexican-born mothers. Scribner and Dwyer (1989) and Weeks et al. (1999) found similar outcomes. Thus, in studying birth outcomes, it is important to classify mothers according to birthplace. This study respects that distinction by differentiating between mothers born in the United States and mothers born in Mexico.
Similarly, among the Mexican-born women, those who are less acculturated Mexican-origin women who live in the U. S. present fewer compromised birth outcomes, with language an important component of acculturation (Cobas et al., 1996; Scribner and Dwyer, 1989). English et al. (1997) found that Mexican-born English-speaking mothers had lower rates of low birth-weight outcomes than do Spanish-speaking mothers. These studies highlight the importance of utilizing language among foreign-born mothers as a key variable for acculturation in studying birth outcomes and infant mortality. Therefore, analysis of the epidemiologic paradox is better served by dividing Mexican-born women into two groups: those who speak only Spanish, and those who speak at least some English. Thus, this article studies three groups: a) Mexican-born women who do not speak English (MNE); b) Mexican-born mothers who stated that they usually or always speak English in the home (MSE), and c) U. S.-born Mexican-American women, regardless of their language (MA). Although language may be a significant variable for the MA group, I do not disaggregate it by language because of the small number of sample cases that would result by doing so.
DATA
Data for this study came from the Border Women's Maternal Health Survey carried out at Thomason Hospital in El Paso, Texas. The survey contains information on 5 076 postpartum women who delivered a live birth at the hospital between April 1995 and March 1997. It gathered data on birth outcomes, risk factors, and conditions for the mother during the pregnancy (social surroundings, behavior, problems experienced, etcetera). Hospital records provided information on infant weight and gestation.
As in any survey, information has its limitations. It includes only women who agreed to participate. No information was collected from non-respondents. Additionally, the survey was self-declared, and the responses to some questions were retrospective, thus limiting their accuracy.
MEASUREMENTS
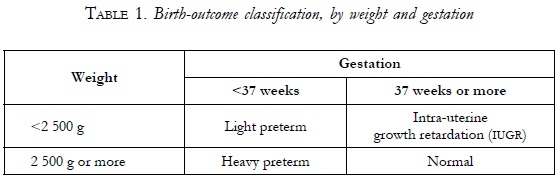
Several factors' effects on birth outcome, including socioeconomic and demographic variables (maternal age, education, and marital status), income, and biomedical characteristics (baby's sex, prenatal care, maternal weight gain, parity, inter-pregnancy interval, and past history) will be measured. The dependent variable is birth outcome, divided into four categories by birth weight (in grams) and gestation (in weeks): normal; low birth-weight preterm (light preterm); intrauterine growth retardation (IUGR), and high birth-weight preterm (heavy preterm). It is noteworthy that with a few exceptions, this information comes from hospital records rather than interviews with the new mothers. For the purpose of this research, normal outcome refers to newborns weighing at least 2 500 g and pregnancies lasting at least 37 weeks. Low birth weight (<2 500 g) is separated into two categories: light preterm, for births in <37 weeks and IUGR, for births in the 37th week or later. Heavy- preterm refers to outcomes with a normal birth weight but born prior to the 37th week of pregnancy. (See Table 1 for a summary of these classifications.)
The majority in the study (61%) were MNE; MSE constituted 13.5% of the sample; and ma constituted the remaining 25.5%.
RESULTS
Because birth outcomes are the main subject in this research, I will begin by examining that variable's principal differences by nationality/language. Among the mothers surveyed mothers in the study, 88.9% had normal birth outcomes; about 5% had heavy-weight preterm births, the most prevalent type of compromised outcome; and 6.1% had low birth-weight outcomes, divided into IUGR (2.4%) and light preterm (3.7%) (Table 2).
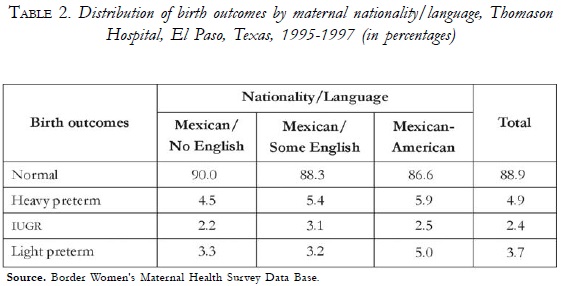
MNE mothers had the highest percentage of normal outcomes (90%) compared to MSE mothers (88.3%) and MA mothers (86.6%). Regarding compromised outcomes, women in all three groups had mainly heavy preterm infants, with MA mothers presenting the highest level (5.9%) and MNE the lowest (4.5%). IUGR outcomes are slightly more common in the MSE group than the other two groups. Nonetheless, the totally compromised outcome category, light preterm, includes 5% of all infants born to Mexican-American women compared to approximately 3.2% for Mexican-born mothers. In general terms, infants born to Mexican women have an advantage over infants of MA mothers. This finding coincides with other studies on nationality/language differences in birth outcomes that determined that Mexican-born women have better birth outcomes than U. S.-born women (Palloni and Morenoff, 2001; Cervantes et al., 1999; Weeks et al, 1999; Crump et al, 1999; English et al, 1997; Singh and Yu, 1996). The association between birth outcomes and different sets of risk factors was analyzed using multinomial logistic regression. First, I examine the odds ratios (ORS) for having light preterm, heavy preterm, or an infant with IUGR outcome based solely on nationality/language (Table 3).
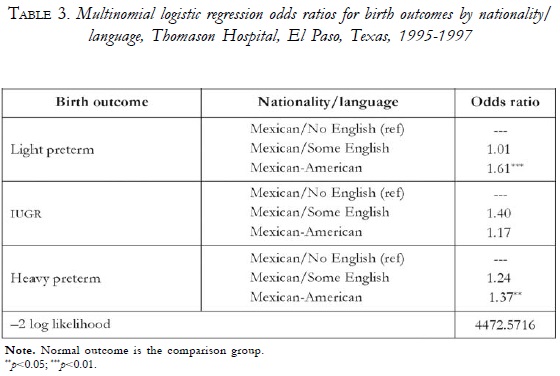
According to this model, Mexican-American women are 61% more likely to have a light preterm infant and 37% more likely to deliver a heavy preterm baby than are MNE mothers. Although not statistically significant, the or for ma women having an infant with IUGR is 17% higher than for MNE. Compared to MNE, MSE show no significant differences for the likelihood of having a compromised birth outcome. Nonetheless, the tendency is more favorable to women who do not speak English; MA are at higher risk of having a light preterm or a heavy preterm infant compared with MNE. This is consistent with most of the literature on the epidemiologic paradox (Cervantes et al., 1999; Collins and Shay, 1994; Cohen et al., 1993; Crump et al., 1999; de la Rosa, 2002; English et al., 1997). In this case, Mexican women who do not speak English, and are thus less embedded in U. S. culture, have a smaller risk of delivering a light preterm infant.
Is this disadvantage for MA women sustained when different risk factors are considered? The following is an analysis of compromised birth outcomes and their associated risk factors. Three multinomial logistic regression models were estimated, with a group of variables added to each model; normal birth outcome is the reference category. Due to space constraints, the models are divided into three separate tables, one for each compromised birth outcome. However, all form part of a single, multinomial regression model.
LIGHT PRETERM RISKS FACTORS
Table 4 demonstrates the relationship among nationality/language, sociodemographic factors, income support factors, biomedical factors, and light preterm birth outcomes. The reference category is normal birth outcome, and the remaining two competing outcomes (IUGR and heavy preterm) are shown in Tables 5 and 6, respectively.
Table 4, Model 1 reveals that Mexican-American women are 1.37 times more likely to have a premature delivery than are Mexican women who speak no English, net of sociodemographic factors. In contrast, regarding this outcome, Mexican women who speak some English do not vary significantly from non-English-speaking Mexican women.
For models 2 and 3 (table 4), it is clear that the prematurity disadvantage for Mexican-American women remains moderately strong and statistically significant, even after inclusion of the complete set of variables. Such a disadvantage for Mexican-American women, in comparison with women born in Mexico, is consistent with previous research showing that nativity is a key distinguishing characteristic for birth outcomes in the United States (Hummer et al., 1999; Landale et al., 2000; Singh and Yu, 1996; Cervantes et al, 1999), with most studies finding that foreign-born women have a clear advantage.
In turn, lack of a statistically significant difference between the two groups of Mexican-born women across the three models suggests that acculturation is not an important distinguishing characteristic, at least for predicting the likelihood of a premature birth in those groups. Thus, at this point, the evidence suggests that nativity differences among women are critical and perhaps reflect the importance of positive health selectivity among Mexican-origin women. At the same time, language differences among Mexican-origin women are not important. This finding contrasts with previous studies that found that the acculturation process heightens the risk for adverse pregnancy outcomes (Coonrod et al., 2004). It is possible that a substantial number of the Mexican women who were admitted to Thomason Hospital for delivery of their infants are not totally immersed in the U. S. acculturation process, either because they continue to live in Mexico or because their interactions are concentrated within a close circle of Mexican-origin friends and relatives.
On observing the remainder of Table 4, there are several important findings to report. Teenage women's odds of having a light preterm birth are roughly 60% higher when compared to women in the 20-34 years of age bracket. This finding is consistent with other studies that have examined maternal age and birth outcomes among Mexican-origin women (Cervantes et al., 1999; Gould et al., 2003; Singh and Yu, 1996). Interestingly, socioeconomic factors exhibit no significant relationship to the likelihood of a light preterm birth outcome, that is, maternal education, marital status, household type, employment status, and receipt of government aid do not display any significant relationship to prematurity. Although the non-significance of these factors might come as a surprise, especially when these variables have been abundantly shown to display birth outcome-associated relationships in the general U. S. population (Cohen et all, 1993; Fuentes-Afflick et all, 1999; Kallan, 1993; Singh and Yu, 1996), their non-significant effects among this Mexican-origin population in the U. S. Southwest is a paradox. Indeed, this is partly because of the lack of a relationship among well-known risk factors and health outcomes. Moreover, Weeks et al. (1999) found no significant effects for certain key socioeconomic variables at the Mexico-U. S. border. Thus, this set of nonsignificant findings further supports the existence of a paradox within this border population. In short, outcomes are generally good, although a heightened risk exists for Mexican-American women, and socioeconomic factors are not important predictors for light preterm birth outcomes.
Table 4, model 3 also demonstrates that a number of biomedical variables are important predictors of light preterm outcomes. Indeed, inadequate and intermediate prenatal care are both associated with higher prematurity levels. In addition, adequate-plus care—that is indicative of a problematic pregnancy (Kotelchuk, 1994a; 1994b)—is also strongly associated with prematurity. A previous failed pregnancy is also heavily associated with prematurity. Together, the effects of adequate-plus care and previous pregnancy loss strongly suggest that a woman's health is a very strong risk factor for prematurity. This is consistent with previous research that firmly suggests the importance of prenatal care for reducing light preterm births (Balcazar et al., 1991; Hessol and Fuentes-Afflick, 2000). Also, first births are also at higher risk, consistent with previous research (Gould et al., 2003; English et al., 1997; Crump et al., 1999). Finally, low weight gain in the mother during pregnancy is strongly associated with prematurity, perhaps in part due to reverse causation—prematurity is, by definition, a shorter pregnancy and does not allow for weight gain that might otherwise occur throughout a full-term pregnancy. It will be even more interesting to observe the manner in which weight gain is related with the odds of IUGR (table 5). Despite the effects of these biomedical variables in the expected direction, their inclusion has little effect on the relationship between nativity and prematurity because Mexican- American women continue to show higher odds of experiencing a preterm pregnancy even in the most complete model. Thus, these biomedical variables do not explain the higher odds of prematurity among Mexican-American women.
In sum, being a Mexican-American mother, being less than 20 years of age at time of delivery, receiving prenatal care that is not adequate, having experienced a failed pregnancy, and having gained 25 lbs or less during the pregnancy are risk factors for a light preterm birth.
INTRAUTERINE GROWTH RETARDATION RISK FACTORS
Table 5 shows the relationships among nationality/language, sociodemographic factors, income factors, biomedical factors, and IUGR birth outcomes; again, the reference category is normal birth outcome. Table 5, model 1 shows that, although Mexican women who speak some English have higher odds for an IUGR birth outcome, there is no significant difference among these women, non-English-speaking Mexican women, and Mexican-American women regarding the likelihood of having an IUGR outcome.
Nonetheless, it is noteworthy that MSE women have the highest odds ratio (36% higher), which could indicate that the IUGR birth-outcome type tends to prevail to a greater degree among these women than among non-English-speaking Mexican women.
Maternal age is an important predictor for IUGR. Mothers of 35 years of age or older are nearly three times as likely to experience IUGR birth outcomes than are mothers in the 20-34 age bracket. This is consistent with previous studies regarding this variable (English et al., 1997; Singh and Yu, 1996; Kallan, 1993).
Odds ratios for education behave in an unexpected way. Groups with less education tend to have a reduced risk of an IUGR outcome, although the risk for these groups is not statistically significant when compared to the reference group. Nevertheless, this is not entirely surprising, because the majority of the women in this study are Mexican and have fewer years of education; thus, the paradox persists.
Moreover, marital status, household type, and labor-force participation have no significant influence on the likelihood of an IUGR outcome because the ORs are not statistically different from 1. Nonetheless, it is noteworthy that a woman living alone or alone with her children tends to have a reduced risk of an IUGR outcome.
Model 2 also includes U. S. government social assistance, such as the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and the Food and Nutrition Services Food Stamp Program, with the direction of ORS as expected; however, these are not statistically significant. As mentioned previously, Mexican-born women use this type of income support less than do U. S.-born Mexican-American mothers, which is consistent with previous findings in previous studies (Echevarría and Frisbie, 2001). Thus, they would be expected to present higher ORS, but that is not the case. This phenomenon is also consistent with the epidemiological paradox because it has been documented that women who receive WIC aid have reduced risks of IUGR outcomes (Frisbie et. al., 1997).
Table 5, model 3 includes the set of biomedical variables as predictors for IUGR outcomes. Age <20 years was not statistically significant, although it shows an OR of >1. Inadequate and adequate plus prenatal care are both highly associated with IUGR, increasing the risk to >200% for the latter. Moreover, women who gained <25 lbs during their pregnancies are also at higher risk of delivering an infant with IUGR than mothers who gained at least 25 lbs, with ORS representing more than double and triple, respectively, the risk of having such an outcome. These findings are consistent with previous studies that determined that the likelihood of a woman giving birth to an infant with IUGR was greatly increased when prenatal care was not adequate, or when weight gain was 15 lbs or less (Frisbie et. al., 1997; Collins and Shay, 1994; Kallan, 1993). Parity and pregnancy interval showed no significant effects on IUGR outcomes with respect to first pregnancy, which contrasts with the study by Lang et al., (1996), who found that first births have higher rates of preterm and small-for-gestational-age birth outcomes.
In sum, women who were 35 years of age or older at time of delivery, who received inadequate or adequate plus prenatal care, and who did not gain at least 25 lbs during the pregnancy are at higher risk of having an infant with IUGR. In this case, nationality/language exerts no significant influence on this birth-outcome type.
HEAVY PRETERM RISK FACTORS
Table 6 presents the relationship between nationality/language, sociodemographic factors, income support factors, biomedical factors, and heavy preterm birth outcomes; the reference category is normal birth outcome. Model 1 in Table 6 demonstrates that being a Mexican-American mother increases the likelihood of a heavy preterm outcome by 40% in comparison with non-English-speaking Mexican women. Frisbie et al. (1997) found that heavy preterm was more likely in Mexican-Americans than in Anglo population. There is no significant difference between the two categories of Mexican-born women.
Age is also an important factor in predicting heavy preterm outcomes; teenage mothers present ca 50% higher odds of delivering a heavy preterm infant, while infants born to mothers aged 35 years of older are not statistically different from infants whose mothers who were 20-34 years of age. As with the remaining compromised outcomes, being married or living with a partner has no significant effect on the heavy preterm birth outcome.
Likewise, household type is not associated with heavy preterm outcomes because no category exhibited a significant difference with the nuclear-household reference category. The same can be affirmed regarding working conditions, because the results for those mothers who participate in the labor force is not statistically different from the results for those who were not working.
Table 6, model 2 adds the variables for income support. Participation in the WIC Program demonstrates a protective effect against the heavy preterm outcome because it reduces the odds for that happening by 25%. This is consistent with previous research findings that show that the WIC Program is beneficial for infant health (Frisbie et al., 1997) because it reduces the risk of all adverse birth outcomes. The Food Stamps Program has an odds ratio of >1, as expected (since participants are in financial need), although the effects of this program are not significant. The Medicare Program also shows an effect in the expected direction, but it also is not statistically significant.
Including biomedical variables shows that female infants are at a lesser risk of being heavy preterm (Table 6, model 3). This is consistent with some previous studies showing that female infants are less likely to born preterm (Frisbie and Song, 2003; Frisbie et al, 1998).
Adequate prenatal care is also very important in preventing heavy preterm births. Women who received inadequate or more than adequate prenatal care are at a very high risk of having this compromised outcome, more than five times the odds in comparison with women who had adequate prenatal care. Again, this is consistent with the majority of studies, which indicate the importance of prenatal care to avert this, or any, type of compromised outcome, or the adequate-plus prenatal care category suggests that these women are at very high risk and receive extra prenatal care. In this case, intermediate prenatal care is not statistically different from adequate care.
Pregnancy-loss history has no statistically significant effect on heavy-weight preterm, but the direction of the ORs was as expected. The weight gain variable, on the other hand, indicates that mothers who fail to gain at least 15 lbs or more are more than tWICe as likely to have a preterm outcome in comparison with mothers who gain 25 lbs or more. This finding contrasts with the result obtained by Frisbie et al. (1997), who found no significant differences between women who gained 15 lbs or less and those who gained 15-40 lbs during their pregnancies.
The parity variable, that is, how many births the mother has previously experienced, did not exhibit a statistically important effect, although the high-parity category has an OR of >2. Other studies also have failed to find an association between parity and compromised birth outcomes (Fuentes-Afflick et al., 1999).
In sum, data from this survey can support only some of the hypotheses stated previously. Infants born to Mexican-American women are significantly more likely to be light preterm, either with or without sufficient gestation at delivery. Mother's age is associated with all three compromised birth outcomes. Being less than 20 years or being 35 or more years of age represents a risk factor for low birth weight and a pregnancy of <37 weeks gestation. Singh and Yu (1996) found similar results when comparing pregnancy outcomes of foreign-born with U. S.-born mothers, concluding that births to mothers 19 years of age or younger and 35 years of age or older are associated with increased risks of low birth weight and preterm birth.
Among variables not demonstrating a significant effect is the existence of a husband/partner in the household. It is possible that the social background of these women influence this non-effect: Perhaps society has placed too much importance on living with a male spouse. Perhaps many women know what to do during their pregnancies, and they do this with or without requiring help from their partners. If a woman does not know what to do or how to react to a specific situation during pregnancy, chances are that her partner does not know either.
Similar reasoning can be applied with regard to education: living in an urban area such as El Paso (Texas, United States)-Ciudad Juarez (Chihuahua, Mexico) can imply that formal knowledge (acquired in school classrooms) can be received from other women, either at home or within another social sphere. In fact, this is consistent with the conclusion drawn by Weeks et al. (1999) that education is not in itself a relevant factor for explaining the differences.
Working conditions are a factor that should be interpreted very carefully. This factor can play a role that can have both negative and positive effects on birth outcomes. For this group of working expectant mothers, only standing up on the job presents a difference that is statistically significant from not working, by lowering the risk of an IUGR outcome. Data did not show additional risks for women who work during their pregnancies, although the women exhibited a rather low economic participation rate.
Of all government social assistance programs included in the questionnaire, only the WIC Program, which was designed specifically to promote mother and infant health, demonstrated fulfillment of its goals with regard to women receiving healthcare at Thomason Hospital, at least with reference to heavy preterm. Frisbie et al. (1997) also found that participation in the WIC Program was important to prevent infants with IUGR and heavy preterm, but the findings were not conclusive with respect to preterm outcomes. Indeed, the authors concluded that the odds of prematurity were higher if medical costs for delivery were paid by a government source. Because the other three government programs are not necessarily focused on pregnancy-related issues, their effects on prevention of compromised outcomes were less.
Perhaps the most direct factors that could affect the birth outcomes included in this research were associated with the maternal biomedical history. It appears natural and logical that an infant's birth weight and gestation are determined more directly by the mother's pregnancy history, or even more directly by prenatal care received and/or proper maternal weight gain during pregnancy.
In sum, certain hypotheses for biomedical factors were supported. Perhaps the most important is that adequate prenatal care plays a very important role in giving birth to an infant weighing >2 500 g and >37 weeks gestation. This was significant in relation to all three compromised-outcome types. For mothers who received adequate-plus prenatal care, physicians should be prepared, and should prepare the woman, to face a compromised outcome, particularly a light preterm or a heavy preterm outcome. This is not surprising because the literature agrees with respect to the importance of adequate prenatal care and its protective effects on birth outcomes (Frisbie et al., 1997; Hessol and Fuentes-Afflick, 2000; Kotelchuck, 1994b).
A previous pregnancy loss indicates a higher risk for the light-preterm outcome. Weight gain during pregnancy proved to be one of the most important variables, because low weight gain (<14 lbs) increases the risk of compromised outcomes. Low parity is a protection against compromised outcomes, compared with first births. Finally, birth intervals of 4 years or more are significant for preventing heavy preterm outcomes.
DISCUSSION
It has long been observed that Mexican-born women use Thomason Hospital in El Paso, Texas, to deliver their babies. Many of these mothers are legal U. S. residents, others are not, and still others cross the U. S.-Mexico border solely to obtain U. S. citizenship for their infant (Ojeda and Lopez, 1994; Guendel-man and Jasis, 1992). However, this situation made it feasible to study another aspect of the epidemiologic paradox, because it was possible to observe women not embedded in American culture in any way, but who nevertheless share many factors with women living in the United States.
Regression analysis showed that only a few variables were statistically significant as birth-outcome predictors. Age was predictive for compromised outcomes because risk increased significantly for women outside the 20-34 years-of-age group. In particular, teenage mothers had a higher probability of compromised outcomes. The group of Mexican-American mothers, on average, had a higher proportion of adolescents than did the group of Mexican-born mothers.
On the other hand, marital status did not predict compromised outcomes. Moreover, the level of education also failed to have an effect on compromised birth outcomes. As mentioned previously, many women offset a lack of formal education with information from other sources, such as relatives, friends, or other social groups. Labor force participation had a positive effect on preventing IUGR births only when the job involved standing up; this had no effect on the other birth outcomes. This could be a case of reverse causation— healthy women may continue to work during pregnancy.
Regarding governmental social-assistance programs, among the surveyed population, those participating in the food stamp program (designed to reduce poverty), and Medicaid (whose mission is not directly related to maternal or child health) did not appear to reduce compromised births. The WIC Program, designed specifically for pregnant women and young children, demonstrated its importance in reducing the risk of heavy preterm outcomes. However, its importance may not have been accurately reflected because, in the survey, the number of individuals participating in WIC was small. If we were to analyze all individuals who receive this support and compare them with those not receiving it, while controlling for other factors, we might be able to ascertain further important differences in terms of birth outcomes for women who participate and women who do not participate in WIC.
Variables included among the biomedical factors essentially were consistent with expectations, because the majority of these helped determine relative risk for light preterm infants. These show strong significance for the majority of the categories. The Adequate Prenatal Care Index developed by Kotelchuck is an excellent predictor of compromised-outcome risk. In each variable present in the woman's pregnancy history (a history of pregnancy loss, parity, and birth interval), Mexican-American women are at a disadvantage compared with Mexican-born women in that the former have higher previous pregnancy loss, comparatively high parity, and are more likely to be having their first child. When compared to the Mexican-American group, a larger percentage of Mexican-born mothers in the survey gained >15 lbs, which would indicate that they were at less risk for compromised birth outcomes.
In conclusion, a number of actions could be implemented to reduce the number of compromised birth outcomes. All involve the information that women ought to receive before becoming pregnant and should be developed around the factors that increase the likelihood of a normal outcome, factors that exist in the Mexican-born population studied here.
First, the adolescent population should be targeted, since being a teenager heightens the risk for all compromised outcomes. The risk among teenagers is compounded because the pregnancy is usually a first birth and, as shown in the survey, approximately 30% of the teenage mothers live with their parents, from whom they may have attempted to hide the pregnancy, thus delaying prenatal and other medical care.
An important step would be more assertive sexual education, particularly concerning contraceptive use for both male and female teenagers, aimed at reducing teen pregnancies. Currently, campaigns focus more on preventing sexually transmitted diseases than on preventing unwanted pregnancies. By reducing pregnancy in teenagers, the average age of the mothers would increase, and proportionally more infants would be born to mothers between 20 and 34 years of age, the ideal age cohort for reducing the risk of compromised birth outcome. Proportionally fewer mothers would hide the pregnancy, and proportionally more mothers would seek professional prenatal care.
Second, steps should be taken to inform women 35 years of age or older that they are at higher risk for certain compromised outcomes. Special medical attention should be given to these women during pregnancy. To the extent that Mexican-Americans are inserted into these dynamics, the gap with Mexican-born mothers may close.
Third, government social-assistance programs ought to continue. The WIC Program is an excellent means for providing women with information regarding contraceptive use and birth spacing.
Fourth, education concerning the risk factors affecting an infant's condition at birth is key. Women should know that a previous pregnancy loss, for example, implies the risk of delivering a preterm baby, but that waiting at least two years to have another child increases the likelihood of a normal outcome. Women should also know that even if they did not receive prenatal care from the beginning of the pregnancy, it is better to have intermediate prenatal care than inadequate care or no care.
Finally, analysis of the Mexican culture and its influence on birth outcomes should continue using a different methodology, perhaps with focus groups and/or in-depth interviews with the Mexican-origin population and with women representing all of the main ethnic groups. The Mexican-born population could learn to use the health-services infrastructure to reduce their chances of compromised birth outcomes, and Mexican-Americans (and the remainder of the U. S. population) could be made aware of the disadvantages of certain behaviors, particularly teen pregnancy, and the advantage of other factors, including strong family ties.
REFERENCES
Albrecht, Stan L., Leslie L. Clarke, Michael K. Miller, and Frank L. Farmer, "Predictors of Differential Birth Outcomes among Hispanic Subgroups in the United States: The Role of Maternal Risk Characteristics and Medical Care," Social Science Quarterly, 77(2), 1996, pp. 407-433. [ Links ]
Balcázar, Héctor, Carolyn Aoyama, and Xi Cai, "Interpretative Views on Hispanics' Perinatal Problems of Low Birth Weight and Prenatal Care," Public Health Reports, vol. 106(4), 1991, pp. 420-426. [ Links ]
Bhutta, Adnan T., Mario A. Cleves, Patrick H. Casey, Mary M. Cradcock, and K. J. S. Anand, "Cognitive and Behavioral Outcomes of School-aged Children who were Born Preterm: A Meta-analysis," Journal of the American Medical Association, 288(6), 2002, pp. 728-737. [ Links ]
Cervantes, Arturo, Louis Keith, and Grace Wyshak, "Adverse Birth Outcomes among Native-Born and Immigrant Women: Replicant National Evidence Regarding Mexicans at the Local Level," Maternal and Child Health Journal, 3(2), 1999, pp. 99-109. [ Links ]
Cobas, José A., Héctor Balcázar, Mary B. Benin, Verna M. Keith, and Yi-nong Chong, "Acculturation and Low-birthweight Infants among Latino Women: A Reanalysis of hhanes Data with Structural Equation Models," American Journal of Public Health, March 1996, vol. 86(3), 1996, pp. 394-396. [ Links ]
Cohen, Bruce B., Daniel J. Friedman, Clare M. Mahan, and Doralba Muñoz, "Ethnicity, Maternal Risk, and Birth Weight among Hispanics in Massachusetts, 1987-89," Public Health Reports, 108(3), 1993, pp. 363-371. [ Links ]
Collins, James W. Jr., and David K. Shay, "Prevalence of Low Birth Weight among Hispanic Infants with United States-Born and Foreign-Born Mothers: The Effect of Urban Poverty," American Journal of Epidemiology, 139(2), 1994, pp. 184-192. [ Links ]
Coonrod, Dean V., R. Curtis Bay, and Héctor Balcázar, "Ethnicity, Acculturation and Obstetric Outcomes: Different Risk Factor Profiles in Low-And High-acculturation Hispanics and in White Non-Hispanics," The Journal of Reproductive Medicine, 49(1), 2004, pp. 17-22. [ Links ]
Crump, Casey, Sherry Lipsky, and Beth A. Mueller, "Adverse Birth Outcomes among Mexican-Americans: Are U. S.-born Women at Greater Risk than Mexico-born Women?," Ethnicity Health, 4(1-2), 1999, pp. 29-34. [ Links ]
De la Rosa, Iván, "Perinatal Outcomes Among Mexican Americans: A Review of an Epidemilogical Paradox," Ethnicity and Disease, vol. 12, Autumn 2002, pp. 480-487. [ Links ]
Echevarría, Samuel, and W Parker Frisbie, "Race/Ethnicity-specific Variation in Adequacy of Prenatal Care Utilization," Social Forces, 80(1), 2001, pp. 633-655. [ Links ]
English, Paul B., Martin Kharrazi, and Sylvia Guendelman, "Pregnancy Outcomes and Risk Factors in Mexican Americans: The Effect of Language Use and Mother's Birthplace," Ethnicity and Disease, 7 (Autumn), 1997, pp. 229-240. [ Links ]
Forbes, D. and P. Frisbie, "Spanish Surname and Anglo Infant Mortality: Differential over a Half-century," Demography, 28(4), 1991, pp. 639-660. [ Links ]
Frisbie, w. Parker, Douglas Forbes, and Robert A. Hummer, "Hispanic Pregnancy Outcomes: Additional Evidence," Social Science Quartery, 79(1), 1998, pp. 149-169. [ Links ]
----------, Douglas Forbes, and Starling Pullum, "Compromised Birth Outcomes and Infant Mortality among Racial and Ethnic Groups," Demography, 33(4), 1996, pp. 469-481. [ Links ]
----------, Monique Biegler, Peter de Turk, Douglas Forbes, and Starling G. Pullum, "Racial and Ethnic Differences in Determinants of Intrauterine Growth Retardation and Other Compromised Birth Outcomes," American Journal of Public Health 87(12), 1997, pp. 1977-1983. [ Links ]
----------, and Seung-eun Song, "Hispanic Pregnancy Outcomes: Differentials over Time and Current Risk Factor Effects," The Policy Studies Journal, 31(2), 2003, pp. 237-252. [ Links ]
Fuentes-Afflick, Elena, and Peter Lurie, "Low Birth weight and Latino Ethnicity: Examining the Epidemiologic Paradox," Archives of Pediatrics and Adolescent Medicine, 151(7), 1997, pp. 665-674. [ Links ]
----------, Nancy A. Hessol, and Eliseo J. Perez-Stable, "Testing the Epidemiologic Paradox of Low Birth weight in Latinos," Archives of Pediatrics and Adolescent Medicine, 153(2), 1999, pp. 147-153. [ Links ]
Gould, Jeffrey B., Ashima Madan, Cheng Qin, and Gilberto Chavez, "Perinatal Outcomes in Two Dissimilar Immigrant Populations in the United States: A Dual Epidemiologic Paradox," Pediatrics 111(6), 2003, e676-e682. [ Links ]
Guendelman, Sylvia, and Monica Jasis, "Giving Birth Across the Border: The San Diego-Tijuana Connection," Social Science & Medicine, 34(4), 1992, pp. 419-425. [ Links ]
Hessol, Nancy A., and Elena Fuentes-Afflick, "The Perinatal Advantage of Mexican-origin Latina women," Annals of Epidemiology, vol. 10(8), 2000, pp. 516-523. [ Links ]
Hummer, Robert A., "Racial Differentials in Infant Mortality in the U. S.: An Examination of Social and Health Determinants," Social Forces, 72(2), 1993, pp. 529-554. [ Links ]
----------, Monique Biegler, Peter B. de Turk, Douglas Forbes, W Parker Frisbie, Ying Hong, and Starling G. Pullum, "Race/Ethnicity, Nativity, and Infant Mortality in the United States," Social Forces, 77(3), 1999, pp. 1083-1118. [ Links ]
----------, Richard G. Rogers, Sarit H. Amir, Douglas Forbes, and W. Parker Frisbie, "Adult Mortality Differentials among Hispanic Subgroups and Non-Hispanic Whites," Social Science Quarterly, 81(1), 2000, pp. 459-477. [ Links ]
Kallan, Jeffrey E., "Race, Intervening Variables, and Two Components of Low Birth Weight," Demography, 30(3), 1993, pp. 489-506. [ Links ]
Kelaher, Margaret, and Dorothy Jones Jessop, "Differences in Low-birthweight among Documented and Undocumented Foreign-born and US-born Latinas," Social Science & Medicine, 55(12), 2002, pp. 2171-2175. [ Links ]
Kotelchuck, M., "The Adequacy of Prenatal Care Utilization Index: its US distribution and Association with Low Birthweight," American Journal of Pubic Health 84(9), 1994a, pp. 1486-1489. [ Links ]
----------, "An Evaluation of the Kessner Adequacy of Prenatal Care Index: And a Proposed Adequacy of Prenatal Care Utilization Index," American Journal of Public Health, 84(9), 1994b, pp. 1414-1420. [ Links ]
Landale, Nancy S., R. S. Oropeza, and Bridget K. Gorman, "Migration and Infant Death: Assimilation or Selective Migration among Puerto Ricans?," American Sociological Review, 65(6), 2000, pp. 888-909. [ Links ]
Lang, Janet M., Ellice Lieberman, and Amy Cohen, "A Comparison of Risk Factors for Preterm Labor and Term Small-for-gestational-age Birth," Epidemiology, 7(4), 1996, pp. 369-376. [ Links ]
Ojeda, Norma, and Silvia López, Familias transfronterizas en Tijuana: Dos estudios complementarios, Tijuana, B. C., El Colegio de la Frontera Norte, Departamento de Estudios de Población, El Colegio de la Frontera Norte, 1994 (Cuadernos, 6). [ Links ]
Palloni, Alberto and Elizabeth Arias, "Explaining the Hispanic adult Mortality Advantage," Demography, 41(3), 2004, pp. 385-415. [ Links ]
----------, and Jeffrey D. Morenoff, "Interpreting the Paradoxical in the Hispanic Paradox: Demographic and Epidemiologic Approaches," Annals of the New York Academy of Sciences, 954, 2001, pp. 140-174. [ Links ]
Rosenberg, T. J., S. Garbers, H. Lipkind, and M. A. Chiasson, "Maternal Obesity and Diabetes as Risk Factors for Adverse Pregnancy Outcomes: Differences among 4 Racial/Ethnic Groups," American Journal of Public Health, 95(9), 2005, pp. 1545-1551. [ Links ]
Scribner, Richard, "Editorial: Paradox as Paradigm—the Health Outcomes of Mexican Americans," American Journal of Public Health, 86(3), 1996, pp. 303-305. [ Links ]
----------, and J. Dwyer, "Acculturation and Low Birth Weight among Latinos in the Hispanic hanes," American Journal of Public Health, 79(9), 1989, pp. 1263-1267. [ Links ]
Singh, Gopal K., and Stella M. Yu, "Adverse Pregnancy Outcomes: Differences between U. S.-and Foreign-Born Women in Major U. S. Racial and Ethnic Groups," American Journal of Public Health, 86(6), 1996, pp. 837-843. [ Links ]
Sorlie, P. D., E. Backlund, N. J. Johnson, and E. Rogot, "Mortality by Hispanic Status in the United States," Journal of the American Medical Association, 270(20), 1993, pp. 2464-2468. [ Links ]
Thompson, J. R., R. L. Carter, A. R. Edwards, J. Roth, M. Ariet, N. L. Ross, and M. B. Resnick, "A Population Based Study of Effects of Birth Weight on Early Developmental Delay or Disability in Children," American Journal of Perinatology, 20(6), 2003, pp. 321-332. [ Links ]
Weeks, John R., Rubén G. Rumbaut, and Norma Ojeda, "Reproductive Outcomes among Mexico-born Women in San Diego and Tijuana: Testing the Migration Selectivity Hypothesis," Journal of Immigrant Health, 1(2), 1999, pp. 77-90. [ Links ]

