











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkBackground
Brain abscesses are infrequent, intracranial infections that are associated to important morbidity and mortality. These infections occur due to contiguous or hematogenous spread of pathogens to the brain parenchyma. In immunocompetent patients, these are mainly caused by bacteria. Brain abscesses most frequently involve gram positive cocci as the main pathogen, but up to 50% are polymicrobial.
Nocardia sp. are aerobic, gram positive bacteria, partially acidfast, filamentous bacteria and are infrequently found as pathogens in humans. Most commonly, Nocardia sp. causes pulmonary infection, due to inhalation being the main route of exposure. Nocardia sp. also represents a rare cause of brain abscess (1-2% of all intracranial abscesses).1 Nocardiosis normally occurs in immunocompromised patients (organ transplant recipients, leukemia, chronic steroid use, and HIV), but up to a third of cases occur in immunocompetent hosts. There are other risk factors can predispose a patient for nocardiosis, like diabetes, alcohol use disorder, and chronic obstructive pulmonary disease.1,2 Of important note, Nocardia sp. can be isolated in patients with underlying pulmonary structural disease, like cystic fibrosis or bronchiectasis.2 Here we present a case of a brain abscess due to Nocardia sp. from Nocardia abscesus complex in a patient with bronchiectasis.
Case presentation
A 56 year-old woman arrived at the emergency room after presenting a brief (minutes) episode of loss of consciousness at home. She had a history of bronchiectasis with normal alpha-1 antitrypsin levels and hepatitis C on sustained virologic response. Otherwise, she was in good health. She did not report any history of other foci of infection, sinusitis, or head trauma. On arrival, the patient was sleepy and inattentive. During the initial evaluation she presented a focal seizure with secondary generalization, with forced eye deviation towards the right, then tonic extension of the right arm followed by bilateral extension of the four extremities. She denied history of headache, fever, nausea or blurred vision during the past week. On examination, deep tendon reflexes were heightened on the right extremities, and a right extensor plantar response was present. Meningeal signs were absent, and the rest of the neurologic examination was normal. Cardiopulmonary examination was normal.
Imaging and laboratory results
She had leukocytosis (12.3x109 cells/L), lymphopenia (370 cells/mL) and a D-dimer value above the detection limit (>10,000 ng/dL). Inflammatory markers (sedimentation rate and procalcitonin) and serum complement levels were normal. A head CT scan was carried out and showed a cystic lesion in the left frontal lobe with associated edema (Figure 1A). A brain MRI was performed. The T1-weighted, T2-weighted and FLAIR sequences showed a sharply defined lesion (16.8 x 16 x 15.1 mm) in the left frontal lobe, with a large area of perilesional edema (Figure 1D). Diffusion weighted imaging showed elevated molecular restriction of the content with reduced apparent diffusion coefficient (Figure 1B,C). The lesion showed an enhancing rim after applying IV contrast (Figure 1E). There were no hemorrhage or calcium components in the susceptibility weighted imaging sequence (Figure 1F). Magnetic resonance spectroscopy demonstrated normal creatinine, choline and N-acetyl aspartate levels with a markedly elevated lactic acid and lipids peak (Figure 1G).
Panel A shows the head CT scan, which reveals a cystic lesion with associated edema in the left frontal lobe found. Panels B-F: Findings on brain MRI. Panel B and C: diffusion weighted imaging, which demonstrates an elevated molecular restriction of the content of the lesion with reduced apparent diffusion coefficient. Panel D: FLAIR sequence, which shows a sharply defined lesion in the left frontal lobe and corroborates the presences of a large area of perilesional edema. Panel E shows the lesion’s enhancing rim after applying IV contrast in T1Weighted imaging. Panel F shows the susceptibility weighted imaging sequence, which reveals no sings of hemorrhage or calcium components. Panel G shows the magnetic resonance spectroscopy. The study reveals normal creatinine, choline and N-acetyl aspartate levels with a markedly elevated lactic acid and lipids peak.
Figure 1 Head CT scan and brain magnetic resonance imaging and magnetic resonance spectroscopy
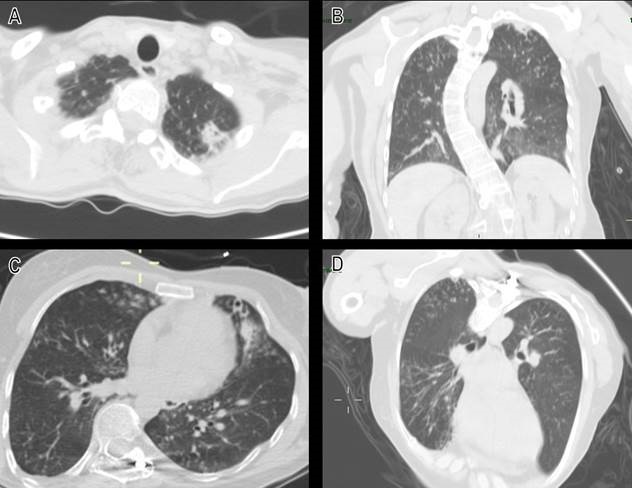
A chest CT scan showed the presence of cavitating lesions on the apical lobes associated to centrilobular nodules, reticulonodular infiltrates (Figure 2A,B) and the previously known cylindrical bronchiectasis (Figure 2C,D). HIV, VDRL, 3 blood cultures set, urinary Histoplasma antigen, serum galactomanan, and interferon-gamma release assay were all negative. Transesophageal echocardiogram ruled out infective endocarditis. The patient underwent a surgical excision of the lesion, and tissue was sent for Tb PCR (GeneXpert®), 16S RNAr sequencing, histopathology, as well as for bacterial, mycobacterial, and fungal cultures.
Discussion
Within the clinical differential in these case were stroke, subdural hematoma, venous thrombosis, malignancy, cysticercosis, and brain abscess. Imaging ruled out most mentioned causes and suggested the diagnosis of a brain abscess, which the craniotomy and surgical resection confirmed. Indolent course suggested a noncommon bacterial etiology. Due to the endemicity of Mycobacterium tuberculosis in Mexico, tuberculous brain abscess was our main differential diagnosis. The negative interferon-gamma release assay, GeneXpert PCR, and cultures discarded this diagnosis. Other important etiologies like toxoplasmosis, histoplasmosis, and neurosyphilis were ruled out.
Etiologic diagnosis
Nocardia sp. was isolated in Lowenstein-Jensen culture and confirmed as a member of Nocardia abscessus complex with 16S ribosomal RNA sequencing, stablishing the diagnosis of nocardial brain abscess. The antibiotic regime was modified to trimethoprim/sulfamethoxazole plus linezolid.
Clinical-pathological correlation
Nocardial brain abscess are the most common presentation of extrapulmonary nocardiosis (up to 44% of cases). Nocardia farcinica is the most commonly isolated pathogen, while Nocardia abscesus is infrequently reported as a cause. Neurological symptoms in Nocardial brain abscess develop gradually (over months or even years) and tend to be more indolent than other etiologies of bacterial brain abscess, with infrequent signs of systemic infection.1 The most common clinical manifestations observed in these cases are seizures and focal neurological deficits.1 This is congruent with our patient’s clinical picture, as it as well did not show any symptoms of systemic infection and had seizures as the initial manifestation of the disease.
As stated earlier, there is a well described association between Nocardia and bronchiectasis. In the context of pulmonary nocardiosis, bronchiectasis is the second most commonly reported predisposing respiratory condition (29-38%).3 This association seems to be strong enough to have epidemiological implications. For example, a study from Duke University Hospital reported a significantly increase in Nocardia incidence over time, which appears to be driven by an increased incidence in patients with bronchiectasis rather than increases in immunocompromised populations.3 Due to this important association and the ruling-out of endocarditis, direct inoculation and contiguous infection as possible causes, the bronchiectasis that our patient presented were deemed to be most likely source of infection. Pulmonary nocardiosis could not be confirmed due to the fact that the patient did not produce a suitable sputum specimen.
Nowadays, MRI and CT scans are important tools for the diagnosis of brain abscess and for ruling out alternate diagnosis, with Nocardial brain abscesses normally presenting as hyperenhanced multiloculated ring lesions with the variable presence of perilesional edema.4 The more indolent clinical picture presented in Nocardial cerebral abscesses in immunocompetent patients make the full utilization of these studies even more vital in the differential diagnosis, as immunocompetent patients the lesions may resemble infarcts or tumors.4 Magnetic resonance spectrum is an useful resource for distinguishing brain abscess from other lesions (gliomas, and cystic or necrotic foci).4 This is due to the fact that brain abscess have scarce amounts the metabolites normally found in healthy brain tissue (N-acetyl aspartate, creatine, and choline) and have elevated levels of lactic acid. Other helpful MRI modality is diffusion weighted imaging, which shows an hyperintense signal inside the abscess cavity with a low apparent diffusion coefficient (ADC).4 Both MRI findings were present in our patient and helped to define the diagnosis within the first 24 hours and thus provide prompt treatment.
The treatment of Nocardial brain abscess remains a multidisciplinary endeavor. Surgical treatment with craniotomy excision or puncture aspiration are fundamental in the early management of the abscess and for the identification of the causative pathogen.1,2 Due to the size and to prevent recurrent infection, craniotomy excision was chosen for our patient. Antibiotic therapy constitutes the other pillar of Nocardial abscess treatment. Due to the risk of recurrence, patients with SNC involvement should receive at least 12 months of antibiotic treatment.1 Trimethoprim/sulfamethoxazole is the agent of choice for the treatment of Nocardiosis with most species of Nocardia sp. being highly susceptible to this therapy.2 Of important note, some species like Nocardia otitidiscaviarum are naturally resistant to trimethoprim/sulfamethoxazole.2 This factors makes the adequate identification of the causative species of Nocardia paramount for the selection of antimicrobial therapy, for which molecular methods like MALDI-TOF or 16S ribosomal RNA sequencing have become standard practice.5 In this case, using 16S ribosomal RNA sequencing we identified a specimen from Nocardia abscesus complex, which allowed us to safely prescribe trimethoprim/sulfamethoxazole monotherapy for our patient.
Finally, Nocardial brain abscesses have a higher mortality Conflicts of interest rate than other causes of brain abscess (up to three times higher), but this is probably directly related to the patient's immune status and not to the Nocardial infection.1 Authors report no conflicts of interest relating to the material This in turn implies a good prognosis to our patient. or methods used nor the results presented in this article.

