











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Saphenous vein grafts (SVGs) are frequently used in coronary artery bypass graft (CABG) surgeries to bypass occluded coronary arteries. In CABG surgery SVGs are frequently used but these grafts are prone to degeneration, atherosclerotic process, and thrombus formation often treated with coronary percutaneous intervention with balloon angioplasty and stenting leading to complications such as in-stent restenosis (ISR) and SVG failure. Management of ISR in SVGs, especially when complicated by chronic total occlusion (CTO) of native coronary arteries, presents unique challenges. This case illustrates a rare complication during the attempt to occlude an SVG with coil embolization during retrograde CTO percutaneous coronary intervention (PCI).
Case presentation
The patient was a 78 years old male with a history of CABG and PCI. His medical history included hypertension, hyperlipidemia and a previous PCI on the SVG to the obtuse marginal (OM) artery (Figure 1).
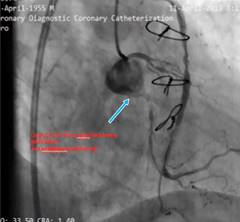
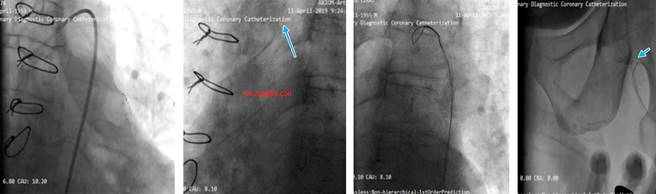
Figure 1: Thrombotic SVG with in-stent restenosis LCx CTO from ostial with no antegrade guide support. (J CTO Score; 4 Long, Calcified, Ambiguous proximal CAP and retry).
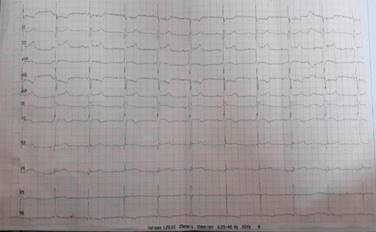
The patient presented with symptoms of acute coronary syndrome, including chest pain and shortness of breath. The ECG was in sinus rhythm and q wave was seen in D2, D3 and AVF leads. (Figure 2) His blood tests showed no significant values. He was referred to our center for tertiary care after coronary angiography performed at another hospital revealed a thrombotic SVG with in stent restenosis and CTO of the left circumflex artery (LCx) (Figure 3).
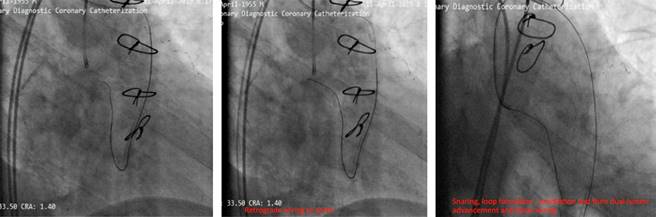
Our aim was to use the SVG as retrograde conduit for CTO PCI. During the procedure stenting was done but the stents balloon ruptured and made a huge dissection which caused a hematoma (Figure 4). As a bailout solution we decided to stent from the ostial LCx (Figure 5). To maintain a sufficient coronary perfusion, we decided to coil occlude due to Thrombolysis in Myocardial Infarction Score (TIMI) flow over 2 in this stenotic and thrombotic SVG so the competitive flow won’t affect the newly opened CTO’s long-term results. While coiling the donor SVG the coil dislodged. During the attempt to snare the dislodged coil with single loop snare, force by this device resulted in fracture in the dislodge coil and made two separated particles. One particle stayed in the descending aorta and the other went to the femoral artery. Both then were snared eventually (Figure 6).
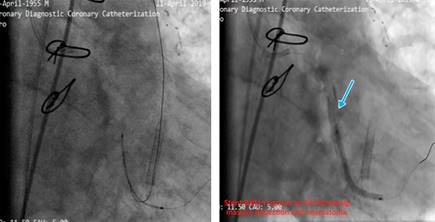
Figure 4: Stenting was done, stent’s balloon ruptured the LCx and created a huge dissection and hematoma.

Figure 5: Free wire in aorta to place the stent ostially and avoid injection. Result after stenting and post dilation.
Discussion
This case highlights several key challenges in the management of post-CABG patients with PCI to SVGs. First, the management of in-stent restenosis in thrombotic SVGs poses significant risks, particularly when CTO is involved in the native coronary arteries. The decision to use the SVG as a retrograde conduit was justified based on the anatomy;1 but complications such as balloon rupture and SVG dissection underscore the importance of selecting appropriate devices and anticipating potential hazards.2,3
Coil occlusion of SVGs is commonly employed to reduce competitive flow; however, in this case, coil dislodgement led to additional complications. The retrieval of coil fragments from both the descending aorta and femoral artery demonstrates the importance of having a bailout plan in such high-risk interventions.4
Moreover, the fracture of the coil during snaring highlights the need for careful handling of retrieval devices to avoid exacerbating complications.
Prompt and efficient operation is necessary after loop formation; as hemodynamic instability can occur quickly due to the compressive forces of looped wires on the heart.
Balloon rupture leading to dissection and hematoma is a severe complication that necessitates immediate bailout strategies, such as ostial stenting, where techniques like the Szabo technique can be helpful.5
When competitive flow from an SVG is present (TIMI flow ≥ 2), coil occlusion should be considered to ensure long-term patency of the newly opened CTO.6
Conclusions
This case underscores several important technical and procedural considerations for managing complex PCI in post-CABG patients with SVG involvement.
Stenotic or occluded SVGs should be considered the primary retrograde route for CTO PCI when available, as they often lead to fewer complications and greater procedural success compared to other collateral routes. Coil retrieval, when necessary, is best managed with three-looped snares, which are superior to single-loop snares for preventing coil fracture and subsequent embolization. This case highlights the importance of careful procedural planning and the ability to handle unexpected complications during complex coronary interventions.

