











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Cardiovascular disease is the leading cause of morbidity and mortality in individuals with type 2 diabetes mellitus (DM2), especially in adults aged 20 to 79 years.1 This disease has gained increasing relevance as a health concern due to its high prevalence and the severe complications it causes.
In Mexico, the prevalence of type 2 diabetes is also alarming. According to the 2021 World Diabetes Day Statistics report from the Instituto Nacional de Estadística y Geografía (INEGI), 10.3% of the population aged 20 years or older (equivalent to 8,542,718 individuals) has been diagnosed with diabetes mellitus. By 2001, 16.1% of the population aged 53 years or older had been diagnosed with diabetes (14.1% in men and 17.8% in women). By 2021, this percentage had risen to 25.6% (22.5% in men and 28.1% in women).2 However, it is estimated that around 60% of individuals with type 2 diabetes are unaware they have the disease, which significantly increases the risk of severe complications, including cardiovascular diseases, renal failure, and other related issues.3
The complications associated with type 2 diabetes have a devastating impact on global health. According to the Diabetes Atlas of the International Diabetes Federation (IDF), complications of DM2 caused approximately 4.2 million deaths worldwide in 2019.1 These complications include cardiovascular diseases, renal failure, blindness, and amputations, which severely affect patients’ quality of life and represent a significant portion of hospital admissions. Diabetes complications often require urgent intervention and early diagnosis, which includes proper treatment.4
Globally, it is estimated that a heart attack occurs every four seconds. In the United States, this event happens every 26 seconds, while in Mexico, it is estimated to occur every three minutes.5,6 INEGI reports that although mortality rates from type 2 diabetes have decreased in recent years, from 119.5 per 100,000 inhabitants in 2020 to 89.4 in 2022, diabetes remains one of the leading causes of death, especially among adults aged 65 years and older. By 2023, mortality rates continued to decrease compared to those reported in 2022.7
Atherogenic risk factors in type 2 diabetes
DM2 often develops years before clinical diagnosis and is strongly associated with various atherosclerotic risk factors (ARFs). These ARFs directly contribute to the progression and severity of DM2, including dyslipidemia, hypertension (HTN), and obesity, all of which significantly elevate cardiovascular risk in these patients.8,9 Therefore, identifying and managing these risk factors is essential to reducing the incidence and severity of cardiovascular diseases (CVD) in individuals with DM2.10
Cardiovascular risk in type 2 diabetes mellitus
Cardiovascular risk (CVR) refers to the probability of developing CVD, such as coronary artery disease, stroke, or peripheral arterial disease. Alarmingly, around 80% of deaths in individuals with DM2 result from vascular complications, with ischemic heart disease accounting for 40% and cerebral ischemia for 10%.
Patients with DM2 often face a combination of risk factors that exacerbate their CVR, including tobacco use, physical inactivity, nonadherence to treatment regimens, prolonged disease duration, and the presence of complications.11,12 Notably, the duration of diabetes is a key determinant, as extended progression increases the risk of conditions affecting multiple organ systems.13
Cardiovascular risk and hospitalization of patients
Hospitalized patients with DM2 are at heightened risk of developing severe vascular complications due to multiple predisposing factors. Scientific evidence highlights that cardio-atherogenic factors often influenced by lifestyle can disrupt blood flow and lead to critical cardiac events.14-16
In Mexico, during the first quarter of 2024, the Epidemiological Surveillance System for DM2 recorded 11,083 hospitalizations of patients diagnosed with DM2, with Tabasco reporting the highest number of cases. Among these, the most common comorbidities included hypertension (affecting 6,705 individuals, 60.50%), obesity (1,488 cases, 13.43%), and chronic kidney disease (CKD) (1,433 cases, 12.93%). Hypertension is a major trigger for life-threatening events like acute myocardial infarction and cerebrovascular accidents, as evidenced by SINAVE data.17
Early intervention in glucose control
Timely intervention in glucose control to achieve the recommended HbA1c targets (≤ 7%) significantly reduces the onset and progression of DM2-related complications. However, the benefits of intensive glycemic control take time to manifest, making early intervention particularly advantageous for younger patients. Weight loss of 10 to 15% also contributes to substantial metabolic improvements.18
For example, studies demonstrate that early glycemic control is associated with a lower incidence of microvascular complications, such as retinopathy and nephropathy, as well as a delay in the progression of macrovascular complications like myocardial infarction. These findings highlight the importance of early and sustained glycemic management to improve long-term outcomes in DM2 patients.
Adapted Framingham risk score for hospitalized DM2 patients
The Framingham Risk Score has been adapted to address limitations in assessing CVR among hospitalized DM2 patients. The original version does not adequately account for factors such as treatment regimens, body mass index (BMI), duration of disease, or gender differences, which are elements critical for accurate risk estimation in this population.19-22
This modified score incorporates these variables, providing a more tailored and reliable assessment of CVR in hospitalized DM2 patients. By offering a contextualized risk evaluation, the adapted score enhances clinical decision-making and supports the prioritization of interventions aimed at reducing cardiovascular morbidity and mortality.
The objective of this study is to establish a correlation between the time of being diabetic and the presence of atherogenic risk factors to understand better and define the cardiovascular risk profile of patients hospitalized with type 2 diabetes mellitus (DM2).
Material and methods
An observational, correlational, and cross-sectional study was conducted. The study population consisted of patients diagnosed with DM2 who were hospitalized at the Medical Specialty Center of the Instituto de Seguridad Social del Estado de Tabasco (ISSET), Mexico, between January and June 2024.
The sample size was calculated by a random test from a population of 3,193 patients, with a confidence level of 95% and a margin of error of five percent, resulting in a sample of 343 patients.
Following the corresponding authorization from the Teaching Committee of the ISSET and obtaining the JI-LCT-179 registry from the Research Center of the Universidad Juárez Autónoma de Tabasco, patients aged 40 to 79 years with clinical records and social security numbers were identified.
Rationale for adjusting the risk score
Diabetes mellitus is a well-established risk factor for microvascular (e.g., retinopathy, nephropathy) and macrovascular (e.g., coronary artery disease, stroke) complications. However, appropriate treatment can significantly delay or even prevent these serious outcomes, emphasizing the importance of personalized cardiovascular risk assessments.
Patients hospitalized with DM2 are often exposed to additional risk factors, such as acute metabolic dysregulation, immobility, and stress, which can accelerate the progression of vascular complications and increase the likelihood of fatal outcomes.
To conduct a comprehensive cardiovascular risk assessment, the Framingham Risk Score was adjusted to include additional variables that are particularly relevant for hospitalized patients with type 2 diabetes mellitus (DM2). While the Framingham Risk Score is widely validated for predicting cardiovascular risk in the general population, it may not fully account for the unique risk factors seen in hospitalized DM2 patients.
To address these limitations, the score was adapted to include the following: Time since diabetes diagnosis, Documented complications in the past five years, and Adherence to diabetes treatment. These adjustments are intended to provide a more nuanced and accurate risk stratification for this specific group (Figures 1 and 2).
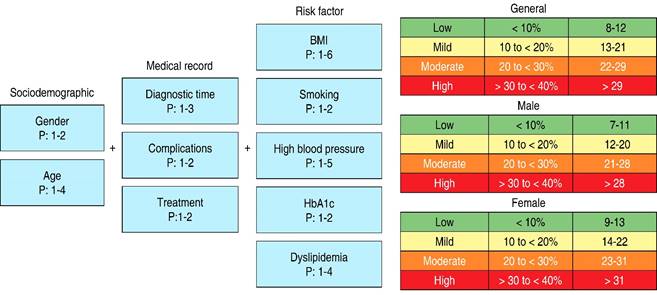
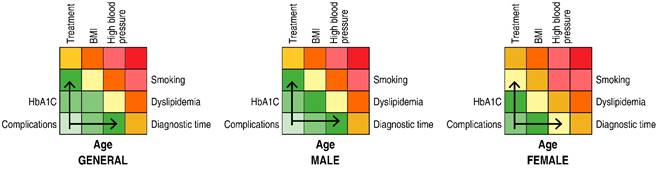
Figure 2: Colorimetry between variables and cardiovascular risk factors in patients with type 2 diabetes mellitus. Differences are observed based on gender, with emphasis on the influence of treatment, body mass index (BMI ), and time of diagnosis.
The data were collected from clinical records in accordance with the ethical guidelines established in NOM-004-SSA3-2012, the General Health Law, and the Federal Law on the Protection of Personal Data Held by Private Parties. The information collected included age, sex, body mass index, blood pressure, lipid profile, HbA1c levels, and any documented complications related to diabetes.
The study adhered to the principles of the Declaration of Helsinki, ensuring the protection of the health, rights, and dignity of the participants. This included obtaining informed consent, safeguarding personal information, and assessing the risks and benefits associated with the research.
Results
Upon examination of the sociodemographic data, the mean age with a standard deviation (SD) was 59.66 ± 9.57 years, with a predominance of females, representing 180 (52.5%) of the records. Marital status was also examined, with 249 (72.6%) patients being married (Table 1), which could potentially influence adherence to treatment and emotional support.
Table 1: Sociodemographic variables (N = 343).
| n (%) | |
|---|---|
| General age* | 59.66 ± 9.57 |
| Male* | 60.06 ± 9.36 |
| Female* | 59.30 ± 9.70 |
| Gender | |
| Male | 163 (47.5) |
| Female | 180 (52.5) |
| Marital status | |
| Single | 80 (23.3) |
| Married | 249 (72.6) |
| Divorced | 8 (2.3) |
| Common-law | 6 (1.7) |
* Data presented as mean ± standard deviation.
A review of the clinical records revealed that 337 patients (98.3%) had complete records. Of this subset, 243 patients (78%) had more than 10 years with the diagnosis of diabetes. Furthermore, 320 (93.5%) patients had been hospitalized in the last five years due to mild complications, and 305 (89.5%) patients had an active treatment plan (Table 2).
Table 2: Clinical data of the patients (N = 343).
| n (%) | |
|---|---|
| Duration of illness (years) | |
| Less than 5 | 48 (14.0) |
| Between 5 to 10 | 52 (15.2) |
| More than 10 | 243 (70.8) |
| Complications < 5 years | |
| Presented complications | 320 (93.5) |
| No complications | 23 (6.7) |
| Treatment | |
| With treatment | 307 (89.5) |
| Without treatment | 36 (10.5) |
| Clinical record | |
| Complete record | 337 (98.3) |
| Incomplete record | 6 (1.7) |
The mean and standard deviation of body mass index (BMI) was 27.50 ± 6.13, with 132 (38.5%) patients classified as overweight at the time of the study. Additionally, 87.7% of patients were non-smokers.
Regarding arterial hypertension, 65.3% of patients were hypertensive. Among them, 36.7% had controlled hypertension, while 28.6% had uncontrolled hypertension, further categorized as grade I (18.7%), grade II (7.9%), and grade III (2%). This highlights that while a significant proportion of patients achieved blood pressure control, a considerable subgroup remains with moderate to severe hypertension, elevating their risk for cardiovascular events.
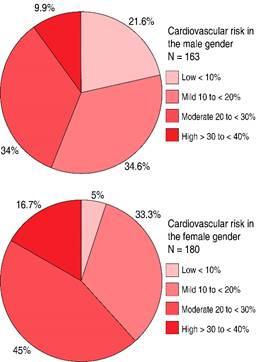
In the glycemic control section, 52.4% of patients demonstrated effective glycemic control. Regarding dyslipidemia, 63.6% of patients had normal cholesterol and triglyceride levels (Table 3). A modified Table was used to calculate cardiovascular risk, revealing that 44 patients (12.8%) had low risk, 132 patients (38.5%) had mild risk, 128 patients (37.3%) had moderate risk, and 39 patients (11.4%) had high risk of experiencing a cardiovascular event within the next 10 years (Table 4;Figure 3).
Table 3: Cardiovascular risk factors (N = 343).
| n (%) | |
|---|---|
| General BMI* | 27.50 ± 6.13 |
| Male* | 23.03 ± 3.88 |
| Female* | 23.37 ± 3.91 |
| Body mass index | |
| Underweight | 24 (7.0) |
| Normal weight | 88 (25.7) |
| Overweight | 132 (38.5) |
| Obesity grade I | 63 (18.4) |
| Obesity grade II | 23 (6.7) |
| Obesity grade III | 13 (3.8) |
| Smoking | |
| No | 301 (87.7) |
| Yes | 42 (12.3) |
| Hypertension | |
| Non hypertensive | 119 (34.7) |
| Controlled | 126 (36.7) |
| Grade I | 64 (18.7) |
| Grade II | 27 (7.9) |
| Grade III | 7 (2.0) |
| Type 2 diabetes mellitus | |
| Controlled (glucose < 130 mg/dL o HbA1c < 7%) | 180 (52.5) |
| Uncontrolled (glucose > 130 mg/dL o HbA1c > 7%) | 163 (47.5) |
| Dyslipidemia | |
| Normal cholesterol and triglycerides | 218 (63.6) |
| Mixed dyslipidemia | 72 (21.0) |
| Hypertriglyceridemia > 150 mg/dL | 39 (11.4) |
| Hypercholesterolemia > 200 mg/dL | 14 (4.1) |
* Data presented as mean ± standard deviation.
The variability of factors associated with cardiovascular risk is evident. Body mass index (BMI) and smoking status show the greatest variability, indicating significant differences among individuals. Additionally, outliers in weight categories and dyslipidemia suggest relevant extreme cases that warrant further detailed analysis. The highest medians in BMI and smoking underscore their potential impact on cardiovascular risk.
Table 4: Cardiovascular risk (N = 343).
| Grouped | n (%) |
|---|---|
| Low risk (< 10%) | 44 (12.8) |
| Mild risk (10 to < 20%) | 132 (38.5) |
| Moderate risk (20 to < 30%) | 128 (37.3) |
| High risk (> 30 to < 40%) | 39 (11.4) |
10-year cardiovascular risk according to the Framingham risk score in patients diagnosed with type 2 diabetes mellitus attended at the Medical Specialties Center of the Instituto de Seguridad Social del Estado de Tabasco between January-June 2024.
Spearman’s correlation analysis revealed positive correlations between BMI and dyslipidemia (p = 0.158, p = 0.003), hypertension (p = 0.200, p < 0.001), and smoking (ρ = 0.118, p = 0.029), indicating that BMI is a primary cardiovascular risk factor. Dyslipidemia was also significantly associated with hypertension (ρ = 0.299, p < 0.001) and poor diabetes control as indicated by HbA1c (p = 0.119, p = 0.028), which in turn predisposes individuals to cardiovascular disease (Table 5).
Table 5: Correlations between atherogenic cardiovascular risk factor variables.
| Variables | BMI | DP | Smoking | HTN | DM2 |
|---|---|---|---|---|---|
| Time since DM2 diagnosis | 0.158*
p = 0.003 |
– | 0.147*
p = 0.006 |
– | – |
| Body mass index | – | 0.158*
p = 0.003 |
0.118‡
p = 0.029 |
0.200*
p < 0.001 |
– |
| Dyslipidemia | 0.158*
p = 0.003 |
– | – | 0.109‡
p = 0.044 |
0.299*
p < 0.001 |
| Smoking | 0.118‡
p = 0.029 |
– | – | 0.225*
p < 0.C001 |
– |
| Hypertension | 0.200*
p < 0.001 |
0.109‡
p = 0.044 |
0.225*
p < 0.001 |
– | 0.119‡
p = 0.028 |
| Control of diabetes by HbA1c | – | 0.299*
p < 0.001 |
– | 0.119‡
p = 0.028 |
– |
* Correlation is significant at the 0.001 level (two-tailed).
‡ Correlation is significant at the 0.005 level (two-tailed).
BMI = Body Mass Index. DP = primary dyslipidemia. HbA1c = hemoglobin A1c. HTN = Arterial Hypertension. DM2 = Type 2 diabetes mellitus (control of type 2 diabetes mellitus by HbA1c.
Discussion
This study identified a significant prevalence of moderate and high cardiovascular risk in patients with type 2 diabetes, particularly in those with hypertension, poor glycemic control, and obesity. Our results contrast with those reported by Bacuilima-Zhañay et al.,4 in whom low cardiovascular risk predominated over five years. This difference could be explained by the population characteristics and the better glycemic control observed in their sample, which reduced the proportion of long-term cardiovascular complications.
Compared to Vega-Jiménez et al.,19 our population has a higher rate of glycemic control (52.4% versus 41%), which correlates with a higher proportion of moderate and high risk in our study. These results highlight the influence of glycemic control on cardiovascular risk classification, a finding consistent with previous literature. Similarly, Zamora-Fung et al.23 reported 80.2% of their population as low risk, which could also be attributed to better glycemic control (58.7%) compared to our sample.
The study by Zalapa-Farias et al.,24 which reported a similar prevalence of dyslipidemia (41%), underscores the importance of glycemic control as a key determinant. Although both populations have a high prevalence of dyslipidemia, the lower proportion of patients with glycemic control in their population (41% versus 52.4% in our study) may explain the observed differences in risk classification.
On the other hand, Poll-Cabrera et al.25 included additional factors, such as hypertriglyceridemia and chronic kidney disease, in their cardiovascular risk assessment, which were not included in our sample. This may explain the higher prevalence of severe cardiovascular risk in their population compared with the 11.4% high risk observed in our study. The inclusion of these factors could enrich future predictive models and provide a more comprehensive view of cardiovascular risk in patients with type 2 diabetes.
Finally, a comparison with Garza-López et al.,26 who used the Framingham model, highlighted the limitations of this model, particularly its inability to take into account factors such as obesity or duration of diabetes. In contrast, our approach using a modified model allowed for a more balanced distribution of cardiovascular risk, highlighting the importance of adapting models to the specific characteristics of the population studied.
In conclusion, our findings underscore the importance of a personalized approach to cardiovascular risk assessment and management in patients with type 2 diabetes. Factors such as glycemic control, hypertension, and obesity should be prioritized in prevention and treatment strategies. In addition, the inclusion of additional comorbidities and the validation of predictive models tailored to different population contexts are key areas for future research.
Conclusion
Comprehensive management of type 2 diabetes should be carefully tailored to the individual needs of each patient. This includes not only glycemic control but also management of major comorbidities, including hypertension, obesity, and other cardiovascular risk factors. The introduction of advanced pharmacological therapies, including Glucagon-Like Peptide-1 (GLP-1) receptor agonists (GLP-1 RAs) and SGLT2 inhibitors (SGLT2is), has demonstrated additional benefits beyond glucose lowering. These therapies have been shown to contribute significantly to cardiovascular and renal protection. These developments should be accompanied by the provision of ongoing diabetes self-management education and support (DSMES) programs, which are essential to improve adherence, optimize clinical outcomes, and reduce the risk of long-term complications.
The study results show that the cardiovascular risk profile of hospitalized patients with type 2 diabetes varies widely. The majority of patients are at moderate cardiovascular risk, while a small proportion are at high risk, particularly those with poor adherence. This finding underscores the importance of early intervention and close monitoring of glycemic control and comorbidities to reduce the risk of cardiovascular complications.
Factors such as the duration of diabetes and the presence of comorbidities, including high body mass index and poor glycemic control, have been identified as key determinants of cardiovascular risk profile. Modification of the Framingham Risk Score to incorporate these specific factors related to type 2 diabetes has improved the predictive ability of the model, allowing for more accurate cardiovascular risk stratification. This adjustment facilitates the early identification of high-risk patients and enables the implementation of preventive strategies.
From a clinical perspective, the results suggest that an integrated and personalized approach that addresses both appropriate glycemic control and management of associated comorbidities is critical to reducing cardiovascular risk in hospitalized patients with type 2 diabetes. It is imperative that treatment be individualized, that adherence to the therapeutic regimen be promoted, and that the influence of social and emotional factors in disease management be considered. The integration of these elements may have a significant impact on improving long-term outcomes and quality of life for patients.

