Clinical cases
Cryoablation and left atrial appendage closure for atrial fibrillation in a patient with ulcerative colitis: case report
Crioablación y cierre de orejuela izquierda por fibrilación auricular en un paciente con colitis ulcerativa: reporte de caso
1 Cardiology Fellow. Tecnológico de Monterrey. Escuela de Medicina y Ciencias de la Salud. Instituto de Cardiología y Medicina Vascular, TecSalud, México. ORCID: 0000-0003-4271-7512
2 Cardiology Fellow. Tecnológico de Monterrey. Escuela de Medicina y Ciencias de la Salud. Instituto de Cardiología y Medicina Vascular, TecSalud, México. ORCID: 0009-0001-0390-3577
3 Electrophysiology Professor. Tecnológico de Monterrey. Escuela de Medicina y Ciencias de la Salud. Instituto de Cardiología y Medicina Vascular, TecSalud, México. ORCID: 0009-0006-3294-8252
4 Cardiology Fellow. Tecnológico de Monterrey. Escuela de Medicina y Ciencias de la Salud. Instituto de Cardiología y Medicina Vascular, TecSalud, México. ORCID: 0000-0002-4745-1277
5 Electrophysiology Professor. Unidad de arritmias y Marcapasos. CMN 20 de Noviembre, ISSSTE. México. ORCID: 0000-0001-8132-0724
Abstract:
Introduction:
when choosing treatment for atrial fibrillation, it is necessary to understand the patient beyond risk scores, to understand the need to drive to sinus rhythm or treatment goals and the speed to be employed given the risk conferred by their chronic diseases and the challenges these diseases pose to conventional strategies.
Case report:
69-year-old male with a history of chronic non-specific ulcerative colitis (CUCI), operated on with subtotal colectomy, since then with abundant, intermittent rectorrhagia. Preoperative assessment of para-stomal hernia revealed AF with an increase in bleeding after the start of anticoagulation, with a high number of episodes, even requiring hospitalization. Due to the hypercoagulable state and immuno-thromboinflammation associated with UC, it was considered a priority to revert to sinus rhythm. Pharmacological cardioversion with amiodarone was attempted without success. He was considered a candidate for cryotherapy ablation after unsuccessful electrical cardioversion, in addition to closure of the left atrial appendage, as he was not considered a candidate for long-term anticoagulation. Cryoablation of the four pulmonary veins was performed without achieving a return to sinus rhythm, so ablation was extended to the posterior wall and left atrial appendage, successfully jugulating the arrhythmia. Finally, a left atrial appendage closure device was placed. After three months of optimal medical management, the patient remained in sinus rhythm, and anticoagulation was discontinued. More than one year after the procedure, the patient is free of thrombotic and bleeding events.
Conclusions:
this case demonstrates the importance of individualizing the approach in atrial fibrillation. Furthermore, extended ablation in atrial fibrillation without origin in the pulmonary veins, and atrial appendage closure, is important as a treatment strategy for patients in complex scenarios who are not candidates for anticoagulation.
Keywords: cryoablation; ulcerative colitis; closure of the left atrial appendage; atrial fibrillation
Resumen:
Introducción:
al momento de elegir el tratamiento de la fibrilación auricular, es necesario entender al paciente más allá de las puntuaciones de riesgo, comprender la necesidad de llevar a ritmo sinusal o a metas de tratamiento y la rapidez que debe emplearse dado el riesgo que confieran sus enfermedades crónicas y los retos que plantean estas enfermedades a las estrategias convencionales.
Presentación de caso:
masculino de 69 años, con antecedente de colitis ulcerativa crónica inespecífica (CUCI), intervenido con colectomía subtotal, desde entonces con rectorragia abundante, intermitente. En valoración preoperatoria de hernia paraestomal se descubre FA. Con aumento de rectorragia tras inicio de anticoagulación, abundante en cantidad, llegando a requerir hospitalización. Por el estado de hipercoagulabilidad e inmuno-tromboinflamación asociada a CUCI, se consideró prioritario revertir a ritmo sinusal. Se intenta sin éxito cardioversión farmacológica con amiodarona. Fue considerado candidato para realizar ablación con crioterapia tras cardioversión eléctrica fallida, además de cierre de orejuela izquierda por considerarse no candidato a anticoagulación a largo plazo. Se realiza crioablación de las cuatro venas pulmonares sin lograr retorno a ritmo sinusal, por lo que se amplía ablación hacia pared posterior y orejuela izquierda, con lo que se logra yugular la arritmia exitosamente. Por último, se coloca dispositivo de cierre de orejuela izquierdo. Tras tres meses de tratamiento médico óptimo tras cirugía se retira anticoagulación, a más de un año del procedimiento el paciente se encuentra libre de eventos trombóticos y hemorrágicos.
Conclusiones:
este caso demuestra la importancia de individualizar el abordaje en la fibrilación auricular. Además, la importancia de la ablación extendida en la fibrilación auricular sin origen en las venas pulmonares, así como el cierre del apéndice auricular como estrategia de tratamiento en pacientes en escenarios complejos no candidatos a anticoagulación.
Palabras clave: crioablación; colitis ulcerativa; cierre de orejuela auricular izquierda; fibrilación auricular
Introduction
Atrial fibrillation (AF) is the most prevalent cardiac arrhythmia in Mexico.1 It is associated with complications such as stroke, heart failure, and death.
Pulmonary vein isolation is a treatment option that prevents disease progression and prevents complications by restoring sinus rhythm.2 Simultaneously, embolic events can be prevented with anticoagulation in most cases.
Thromboembolic prevention, guided by international recommendations, continues to be the first-line management. However, sometimes, the preventive benefit of anticoagulants is limited by the increased risk in the bleeding rate. In cases of high bleeding risk, occlusion of the left atrial appendage can be considered an alternative to anticoagulation in complex scenarios who are not candidates for long-term anticoagulation due to having a high risk of bleeding.
Case presentation
A male 69-years-old Latino with a history of intense smoking and a sedentary lifestyle underwent a subtotal colectomy in 2016 due to diagnosis of UC disease complicated with an episode of toxic megacolon. Since then, the patient has had episodes of intermittent rectorrhagia. In February 2023, the patient noted the presence of a parasternal hernia; during pre-surgical protocol for hernia repair, an atrial fibrillation rhythm was found. Following the current guidelines, antiarrhythmic medication and oral anticoagulation were started. However, the patient failed to return to sinus rhythm and developed gastrointestinal bleeding due to management, with increased rectorrhagia, which requires admission to the hospital due to bleeding, so he was disregarded as a candidate for lifelong anticoagulation.
In trying to find the trigger and the substrate that triggered the arrhythmia, a non-obstructive CAD in the coronary computed tomography angiography was found, and in the transthoracic echocardiography the findings where a biauricular dilatation and a decreased atrial function, RV dilatation, PASP was 54 mmHg, LV diastolic dysfunction grade III, and preserved biventricular function, without areas of hypokinesia or akinesia - revealing atrial dilatation as the likely trigger.
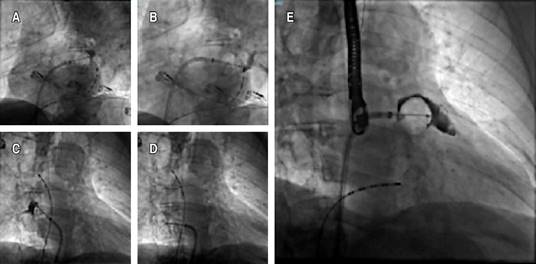
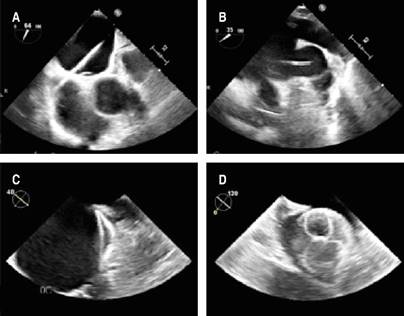
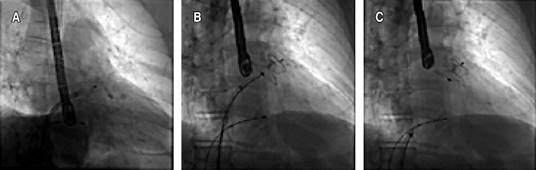
Even though conventional scores showed a low-risk result, it was considered essential to revert to sinus rhythm due to the strong thrombotic component conditioned by the UC and the contraindication for anticoagulation. An electrophysiological study was performed, followed by cryoablation of the four pulmonary veins (Figures 1 and 2), without achieving sinus rhythm, so it was decided to perform non-success electrical cardioversion twice (200 joules). The intervention team decided to perform a wide antral circumferential ablation (WACA) with posterior wall and left atrial appendage isolation, thus successfully achieving arrhythmia jugulation. Due to the hindrance of anticoagulation, after the left atrial appendage isolation, a closure device was placed in the left atrial appendage (Figures 2 and 3). After three months of optimal medical management with apixaban and amiodarone, the patient remained in sinus rhythm, and anticoagulation was discontinued. The patient is free of thrombotic and bleeding events for more than one year after the procedure and after stopping the anticoagulant.
Discussion
Cryoablation of pulmonary veins is a well-studied and effective treatment strategy for patients with atrial fibrillation. Nevertheless, there is always the possibility of procedural failure or recurrence of arrhythmia. In our patient, the arrhythmogenic substrate was in the left atrial appendage. After isolation, the arrhythmia stopped at a site with low incidence reported in the literature. In these scenarios, wide ablation techniques should be used and the search should be expanded to include structures outside the pulmonary veins.2 However, previous studies have demonstrated its potential arrhythmic capacity.3 Therefore, catheter ablation of the posterior wall and left atrial appendage has emerged as an option to increase therapeutic efficacy and improve outcomes in patients with persistent AF originating outside the pulmonary veins.4,5 It has been suggested that there is a substantial risk of thrombus in those undergoing left atrial appendage isolation, so patients undergoing isolation usually also require LAAC.2
This case highlights that anticoagulation given to reduce the risk of stroke carries the burden of an increased risk of bleeding, so finding the right balance is crucial. In patients with atrial fibrillation and high bleeding scores, which also have a high thromboembolic risk due to the thrombotic inflammation and immunothrombosis state by chronic diseases, another alternative must be sought.6-8 In complex scenarios with a high bleeding risk, occlusion of the left atrial appendage can be considered as an alternative to anticoagulation in those who are not candidates for long-term. In the Prague-17 trial, the use of the left appendage closure device has demonstrated non-inferiority compared to oral anticoagulation to prevent stroke, consistent with what has been reported by studies PROTECT AF and PREVAIL.2,9
In this case of ulcerative colitis and persistent atrial fibrillation with failed electric cardioversion, cryoablation of pulmonary veins, and WACA, including left atrial appendage before the placement of an occlusion device resulted in an effective strategy for rhythm control and stroke prevention. Current guidelines support the use of atrial appendage closure devices with a cautious level of recommendation in selected patients, particularly in cases such as this, where the use of anticoagulation is prohibitive.10 However, in complex scenarios, it is an extremely useful tool, and its use is growing exponentially.
Conclusions
This case demonstrates the importance of individualizing the approach in a patient at high risk of thrombotic and bleeding events, where the appendage closure device is a good treatment strategy. In addition, cryoballoon ablation of the left atrial appendage and left posterior wall ablation are innovative techniques with few reported cases and were critical to the successful management of our patient.
Acknowledgement
We want to thank Dr. Carlos Jerjes-Sánchez for his guidance and advice in the realization of this work.
References
1. Rodríguez-Reyes H, Laguna-Muñoz CI, Gallegos-de Luna CF, Ríos-Ibarra MO, Salas-Pacheco JL, Leyva-Pons JL et al. Fibrilación auricular en población mexicana: diferencias en presentación, comorbilidades y factores de riesgo entre hombres y mujeres. Arch Cardiol Méx. 2022; 92 (3): 349-357. doi: 10.24875/acm.21000120.
[ Links ]
2. Parameswaran R, Al-Kaisey AM, Kalman JM. Catheter ablation for atrial fibrillation: current indications and evolving technologies. Nat Rev Cardiol. 2021; 18 (3): 210-225. doi: 10.1038/s41569-020-00451-x.
[ Links ]
3. Al-Rawahi M, Liang J, Kapa S, Lin A, Shirai Y, Kuo L et al. Incidence of left atrial appendage triggers in patients with atrial fibrillation undergoing catheter ablation. J Am Coll Cardiol EP. 2020; 6 (1): 21-30. doi: 10.1016/j.jacep.2019.08.012.
[ Links ]
4. He B, Jiang LS, Hao ZY, Wang H, Miao YT. Combination of ablation and left atrial appendage closure as “One-stop” procedure in the treatment of atrial fibrillation: current status and future perspective. Pacing Clin Electrophysiology. 2021; 44 (7): 1259-1266. doi: 10.1111/pace.14201.
[ Links ]
5. Yorgun H, Canpolat U, Kocyigit D, Coteli C, Evranos B, Aytemir K. Left atrial appendage isolation in addition to pulmonary vein isolation in persistent atrial fibrillation: one-year clinical outcome after cryoballoon-based ablation. Europace. 2017; 19 (5): 758-768. doi: 10.1093/europace/eux005.
[ Links ]
6. Potere N, Abbate A, Kanthi Y, Carrier M, Toldo S, Porreca E et al. Inflammasome signaling, thromboinflammation, and venous thromboembolism. J Am Coll Cardiol Basic Trans Science. 2023; 8 (9): 1245-1261. doi: 10.1016/j.jacbts.2023.03.017.
[ Links ]
7. Senchenkova EY, Ansari J, Becker F, Vital SA, Al-Yafeai Z, Sparkenbaugh EM et al. Novel role for the AnxA1-Fpr2/ALX signaling axis as a key regulator of platelet function to promote resolution of inflammation. Circulation. 2019; 140 (4): 319-335. doi: 10.1161/circulationaha.118.039345.
[ Links ]
8. Shah AR, Jala V, Arshad H, Bilal M. Evaluation and management of lower gastrointestinal bleeding. Dis A Mon. 2018; 64 (7): 321-332. doi: 10.1016/j.disamonth.2018.02.002.
[ Links ]
9. Osmancik P, Herman D, Neuzil P Hala P, Taborsky M, Kala P et al. Left Atrial Appendage Closure Versus Direct Oral Anticoagulants in High-Risk Patients With Atrial Fibrillation. J Am Coll Cardiol. 2020; 75 (25): 3122-3135. doi: 10.1016/j.jacc.2020.04.067.
[ Links ]
10. Tzeis S, Gerstenfeld EP, Kalman J, Saad EB, Sepheri Shamloo A, Andrade JG et al. 2024 European heart rhythm association/heart rhythm society/Asia Pacific heart rhythm society/Latin american heart rhythm society expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace. 2024; 26 (4).
[ Links ]












 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink