











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
INTRODUCTION
A transjugular intrahepatic portosystemic shunt (TIPS) is a cornerstone in the management of complications of portal hypertension1,2. TIPS effectively reduces the hepatic venous pressure gradient by creating a low-resistance channel between the portal and systemic venous systems, reducing the risk of variceal bleeding, refractory ascites, hepatic hydrothorax, Budd-Chiari syndrome, portal vein thrombosis, and other portal hypertension complications1-9. In addition, TIPS has been accepted as a bridging therapy for liver transplantation (LT) in cirrhotic patients4,9.
The direct impact of TIPS on the survival of patients with cirrhosis is controversial. Some authors have demonstrated improved outcomes in carefully selected patients10,11; others have highlighted the increased risk of overt hepatic encephalopathy (OHE) and procedure-related mortality, reflecting the heterogeneity of the underlying liver disease and comorbidities3,5,6,8,9. Mortality after TIPS is influenced by several clinical and hemodynamic factors such as the Child-Pugh score, active bleeding, right-sided heart failure, and pulmonary hypertension, emphasizing the importance of appropriate patient selection1,12.
Data on the efficacy of TIPS in preventing complications due to decompensation after the procedure have been described13,14. To date, there is no conclusive evidence of a patient survival benefit after TIPS, even with the exclusive use of covered stents such as the Viatorr13. TIPS effectively controls portal hypertension complications. However, its association with OHE and age-related mortality with or without LT warrants further evaluation. This study evaluated 5-year mortality in cirrhotic patients after TIPS, compared patients after TIPS with or without LT, and identified risk factors as predictors of mortality.
MATERIAL AND METHODS
This retrospective cohort study was conducted from March 2014 to March 2025 in the Department of Interventional Radiology of the Hospital San Jose and Hospital Zambrano Hellion, TecSalud, a private tertiary-care institution in Monterrey, Nuevo Leon, Mexico. Patients with cirrhosis and decompensated portal hyper-tension who required TIPS were included. Exclusion criteria were LT before TIPS, incomplete information in the medical records, and patients who had undergone TIPS in other centers. Informed consent was not required for data collection as part of routine medical care. The institutional ethics and research committees approved the study protocol.
Study development and variables
Patients' medical records and monthly follow-up visits after TIPS were analyzed. Age, sex, indications for the TIPS procedure, the Child-Pugh score, the Model for End-Stage Liver Disease (MELD) score, and the final portosystemic pressure gradient (PSPG) during the TIPS procedure were recorded. The referring hepatologists determined the etiology of cirrhosis by laboratory analysis and/or liver biopsy results. Cirrhotic patients with TIPS who underwent LT during the study were recorded.
Technical TIPS procedure
All TIPS procedures were performed with a RUPS-100 Transjugular Liver Access Set (Cook Medical, Bloomington, IN, USA). The corrected sinusoidal pressure was calculated as the difference between the wedged hepatic venous pressure (WHVP) and the free hepatic venous pressure, with WHVP determined in the right hepatic vein by advancing the sheath or catheter until contrast injection produced no venous reflux. Under fluoroscopic guidance, the intrahepatic puncture was directed from the right hepatic vein towards the right portal vein. Splenoportography and sizing of the shunt were performed with a 4-5F pigtail catheter, followed by tract predilatation with 6-8 mm angioplasty balloons. Bare-metal stents were used from 2004 to 2011; a Viatorr™ expanded polytetrafluoroethylene (ePTFE)-lined stent-graft endoprosthesis (W.L. Gore & Associates, Newark, DE, USA) has been used since 2012. After placement of the stent, 8-10 mm high-pressure angioplasty balloons were used until the PSPG between the portal and hepatic veins reached the target value. The inferior vena cava and right atrial pressures were also measured before sheath removal. Hemostasis was achieved by manual compression, and large-volume paracentesis was performed immediately after the procedure in patients with ascites. Figure 1 shows digital subtraction angiography after performing a TIPS in a 39-year-old man with cirrhosis and variceal bleeding. A covered stent and hepatofugal flow with multiple venous collaterals, including gastric and renal shunts, are seen. Trans-TIPS embolization of the fugal shunts was performed with helical coils and ethanol + Gelfoam®. A team of three interventional radiologists with 31 years (MCM), 11 years (FPG), and two years (SKJ) of experience performed the TIPS procedures.
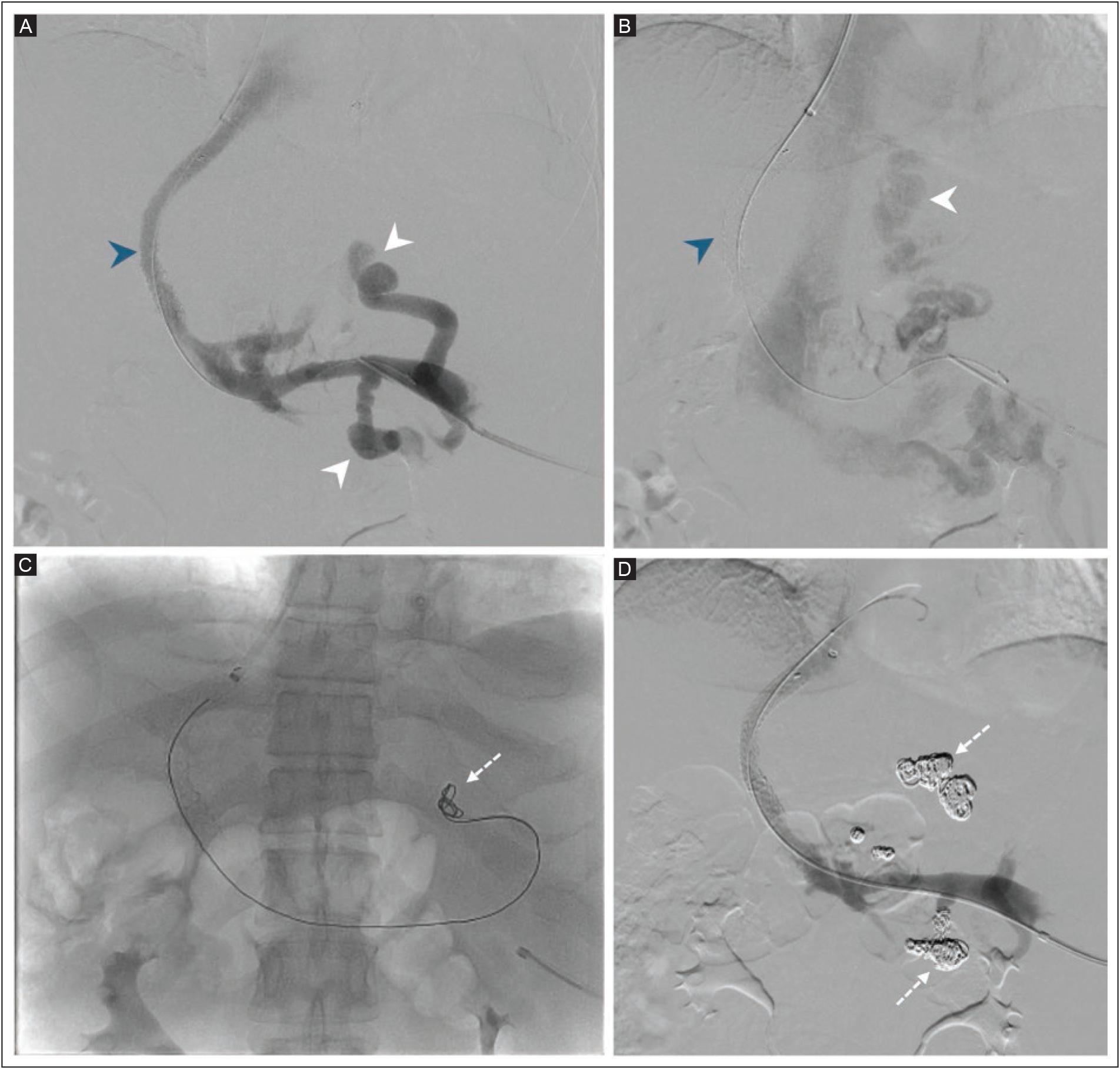
TIPS: transjugular intrahepatic portosystemic shunt.
Figure 1 Digital subtraction angiography after TIPS placement in a 39-year-old man with cirrhosis and variceal bleeding. A-B: a covered stent (blue arrowheads) with hepatofugal flow, with multiple venous collaterals, and gastric and renal shunts are seen (white arrowheads). C-D: trans-TIPS embolization of the fugal shunts performed with helical coils (dashed arrows) and ethanol + Gelfoam®.
Statistical analysis
The statistical normality of the continuous variables was determined with the Shapiro-Wilk test. Non-normal distributions are presented as median and interquartile range (IQR). Categorical data are summarized as frequencies and percentages. The primary endpoint was all-cause mortality. Mortality time, measured in years from the time of TIPS to death or last follow-up, censored patients at the time of LT. All-cause mortality was estimated using Kaplan-Meier analysis, with group differences evaluated using the log-rank test. Multi-variable Cox proportional hazards models were used to identify predictors of mortality and evaluate the effect of LT. Variables were selected for clinical relevance and univariate associations. All models were tested for proportional hazards assumptions. A standard Cox regression model was initially used to assess baseline predictors of cirrhotic patients with TIPS. To estimate the survival benefit of LT, a time-dependent Cox model treated LT patients as time-varying covariates, resulting in hazard ratios adjusted for baseline characteristics. A two-sided p value ≤ 0.05 was significant. Statistical analysis and plotting were performed using Python (v3.13) (Python Software Foundation, Wilmington, DE, USA) with the pandas, lifelines, and matplotlib libraries.
RESULTS
A total of 101 cirrhotic patients were eligible, but eleven were excluded due to incomplete medical records or missing follow-up. A cohort of 90 cirrhotic patients with a mean age of 56 ± 12.5 years who underwent TIPS was included (Table 1). The majority were men (n = 56, 62.2%), and the most common etiology of cirrhosis was metabolic-associated fatty liver disease (n = 30, 33.4%), followed by autoimmune hepatitis (n = 16, 17.8%) and alcohol-related liver disease (n = 14, 15.6%). The main indication for TIPS was variceal bleeding (n = 52, 57.8%), followed by refractory ascites (n = 36, 40.0%). The mean MELD score at the time of the TIPS procedure was 17 ± 7. Pre-TIPS encephalopathy was found in 21 (23.3%), and OHE was present in 14 (15.6%) of the 90 cirrhotic patients during a follow-up period of 5 years. The median final PSPG was 8 mmHg with an IQR of 6 to 10 mmHg.
Table 1 Characteristics of 90 cirrhotic patients with TIPS
| Description | Parameter |
|---|---|
| Age, years, mean ± SD | 56 ± 12.5 |
| Sex, n (%) | |
| Men | 56 (62.2) |
| Women | 34 (37.8) |
| Etiology of cirrhosis, n (%) | |
| Metabolic-associated fatty liver disease | 30 (33.4) |
| Autoimmune hepatitis | 16 (17.8) |
| Alcohol-related liver disease | 14 (15.6) |
| Viral hepatitis | 8 (8.9) |
| Primary biliary cholangitis | 3 (3.3) |
| Non-cirrhotic portal hypertension | 3 (3.3) |
| Idiopathic | 3 (3.3) |
| Overlap syndrome | 2 (2.2) |
| Not classified | 11 (12.2) |
| Indication for TIPS, n (%) | |
| Variceal bleeding | 52 (57.8) |
| Refractory ascites | 36 (40.0) |
| Hepatic hydrothorax | 2 (2.2) |
| Child-Pugh score, n (%) | |
| A | 13 (14.4) |
| B | 43 (47.8) |
| C | 34 (37.8) |
| MELD score, per point, mean ± SD | 17 ± 7 |
| Encephalopathy, n (%) | |
| PTE | 21 (23.3) |
| OHE | 14 (15.6) |
| Final PSPG, mmHg, median (IQR) | 8 (6-10) |
TIPS: transjugular intrahepatic portosystemic shunt; MELD: model for end-stage liver disease; PTE: pre-TIPS encephalopathy; PSPG: portosystemic pressure gradient; OHE: overt hepatic encephalopathy; IQR: interquartile range.
Five-year overall mortality in cirrhotic patients with TIPS
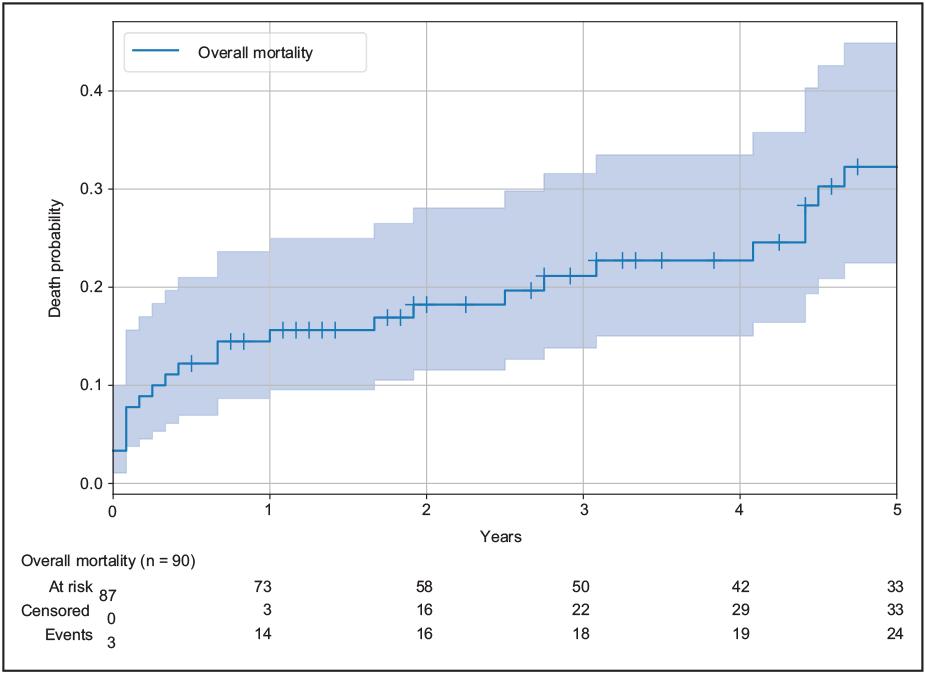
The estimated all-cause mortality for the cohort after the TIPS procedure is shown in figure 2. Mortality was 15.6% at 1 year, 21.1% at 3 years, and 32.3% at 5 years.
Comparison of mortality in cirrhotic patients with TIPS with or without OHE
Cirrhotic patients with OHE had higher mortality than patients without OHE (p = 0.001) (Figure 3A). Patients with OHE had a mortality of 35.7% at 1 year, 50.0% at 3 years and 60.0% at 5 years after the TIPS procedure. In contrast, mortality in cirrhotic patients without OHE with TIPS was 11.9% at 1 year, 15.2% at 3 years, and 26.2% at 5 years.
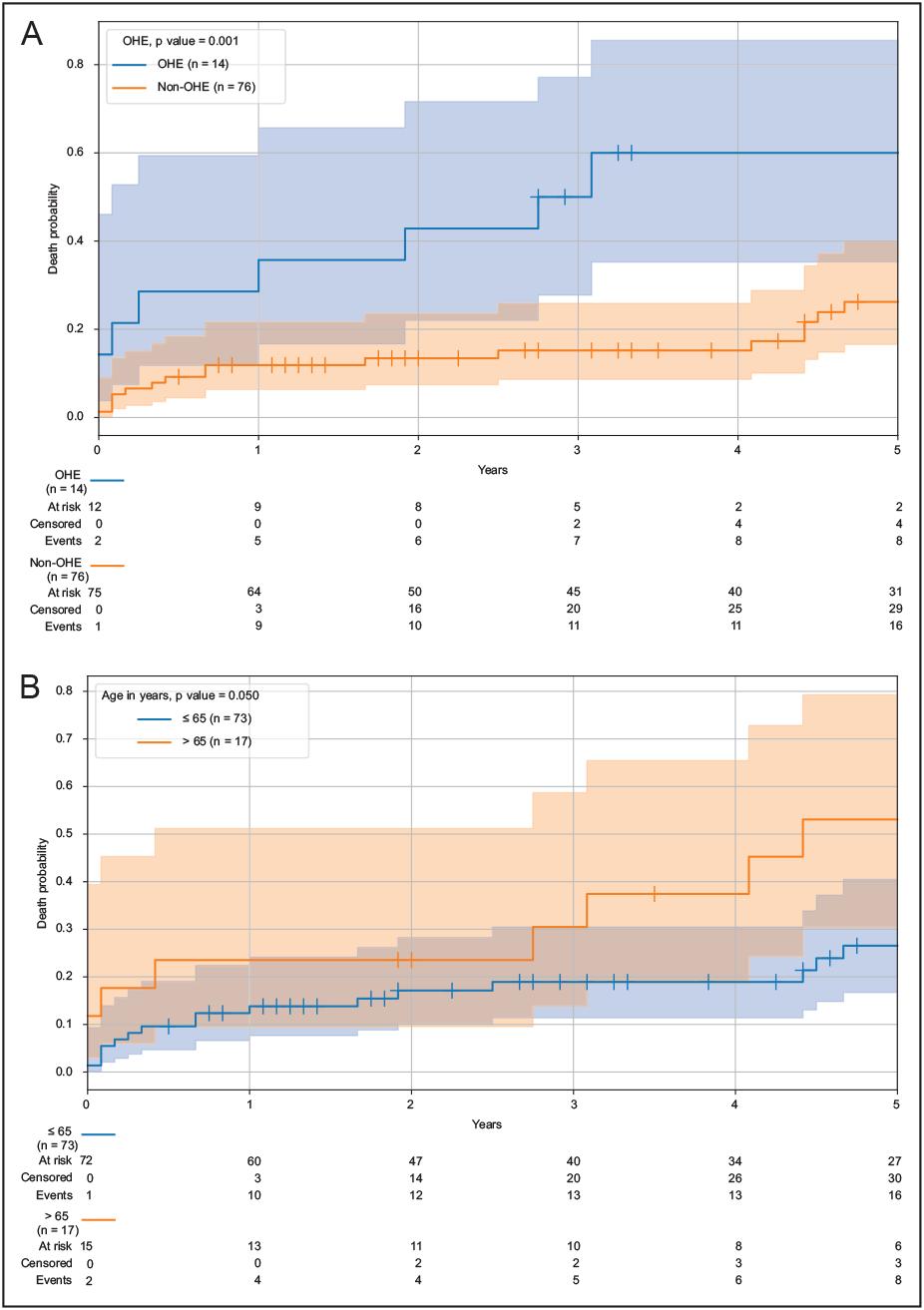
OHE: overt hepatic encephalopathy; TIPS: transjugular intrahepatic portosystemic shunt.
Figure 3 Mortality of cirrhotic patients with TIPS in relation to OHE and age. A: with OHE, mortality was 35.7% at 1 year, 50.0% at 3 years, and 60.0% at 5 years. Cirrhotic patients without OHE had a mortality of 11.9% at 1 year, 15.2% at 3 years, and 26.2% at 5 years. Cirrhotic patients with TIPS and OHE were significantly associated with higher mortality (p = 0.001). B: cirrhotic patients with TIPS ≤ 65 years showed a mortality of 13.8% at 1 year, 18.9% at 3 years, and 26.5% at 5 years. In patients aged > 65, mortality was 23.5% at 1 year, 30.5% at 3 years, and 53.1% at 5 years. Older age was significantly associated with mortality at 5-year follow-up (p = 0.05).
Univariate analysis of mortality associated with age in cirrhotic patients with TIPS
A Kaplan-Meier analysis using the log-rank test was performed to identify individual factors associated with mortality (Figure 3B). Cirrhotic patients with TIPS aged ≤65 years had a mortality of 13.8% at 1 year, 18.9% at 3 years and 26.5% at 5 years. In contrast, cirrhotic patients older than 65 years had increased mortality compared to younger patients, who had a mortality of 23.5% at 1 year, 30.5% at 3 years, and 53.1% at 5 years after TIPS. Patients older than 65 years had a significantly higher mortality than younger patients (p = 0.05).
A non-significant trend towards increased mortality was found in patients who underwent TIPS for variceal bleeding compared to patients with refractory ascites and hepatic hydrothorax (p = 0.09). Univariate analysis showed no significant association between other baseline characteristics and mortality. These included sex (p = 0.55), etiology of liver disease (metabolic-associated fatty liver disease vs. other, p = 0.17), a MELD score greater than 15 points (p = 0.16), or the presence of pre-TIPS encephalopathy (p = 0.19).
Multivariable analysis of mortality predictors in cirrhotic patients after TIPS
To identify independent risk factors for mortality, a multivariable Cox proportional hazards model was constructed focusing on the "TIPS-alone" therapeutic pathway. The model was fitted on the entire cohort of 90 patients. For this analysis, patient follow-up at the time of LT was censored (n = 16) (Table 2). This data corres-ponds to a model based on 90 subjects, including 24 deaths, with a concordance index of 0.716. After adjustment for other factors, the patient's age was the only significant independent predictor of mortality (HR: 1.06 per year; 95% CI, 1.01-1.10) (p = 0.009). This finding means that the risk of death increases 6% for each year that age increases. Although a higher MELD score was associated with an increased risk of death (HR, 1.06 per point; 95% CI, 0.99-1.13), this result did not reach statistical significance (p = 0.098). Sex and the presence of pre-TIPS encephalopathy were not significantly associated with mortality in this model.
Table 2 Multivariable Cox regression analysisa of the predictors of mortality in cirrhotic patients with TIPS
| Description | HR | 95% CI | p |
|---|---|---|---|
| Age, per year | 1.06 | 1.01-1.10 | 0.009 |
| Sex, women vs. men | 0.62 | 0.24-1.61 | 0.325 |
| MELD score, per point | 1.06 | 0.99-1.13 | 0.098 |
| PTE, yes vs. no | 1.43 | 0.55-3.70 | 0.462 |
aThe model is based on 90 patients with 24 deaths. Concordance index = 0.716. The model fulfilled the proportional hazard assumption. TIPS: transjugular intrahepatic portosystemic shunt; MELD: model for end-stage liver disease; PTE: pre-TIPS encephalopathy; HR: hazard ratio; CI: confidence interval.
Mortality in cirrhotic patients after TIPS compared to cirrhotic patients with TIPS and LT
A log-rank test compared cirrhotic patients with TIPS and cirrhotic patients with TIPS and LT. During the follow-up period, 16 (17.8%) patients underwent LT. There were no significant differences in outcome between the two groups and no evidence of increased mortality (p = 0.074) (Figure 4). The overall mortality in cirrhotic patients with TIPS and LT was 12.5% over 5 years. These were treated as censored events, leaving 24 deaths for the model analysis
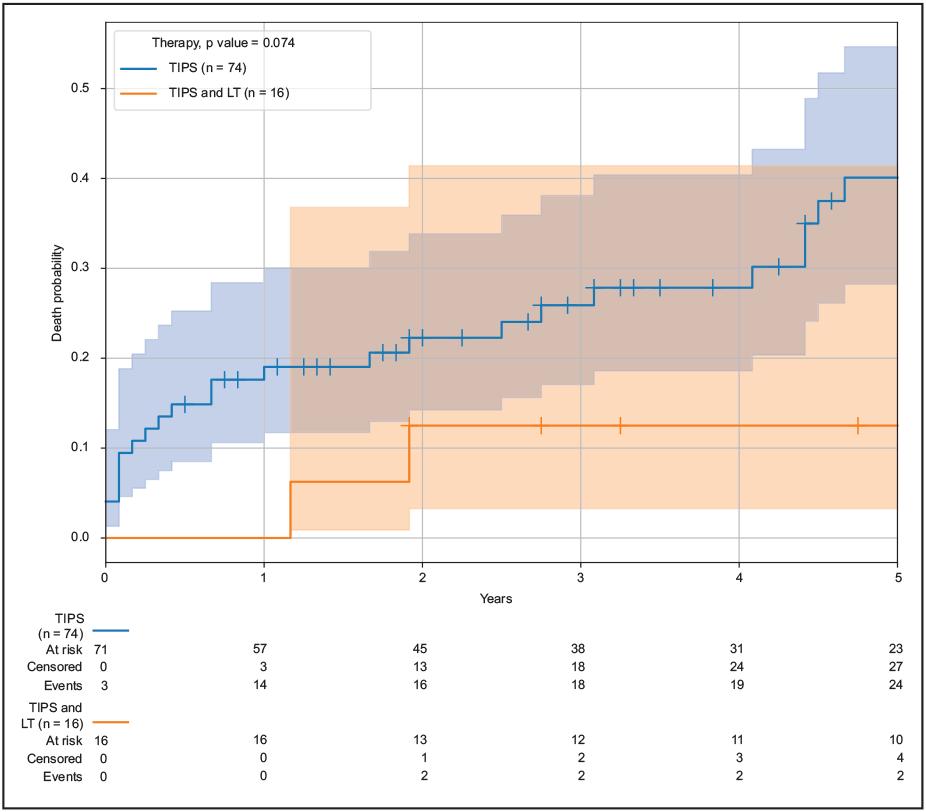
LT: liver transplantation; TIPS: transjugular intrahepatic portosystemic shunt.
Figure 4 Cirrhotic patients with TIPS had a 5-year mortality of 40.1%. Cirrhotic patients with TIPS and LT had a 5-year mortality of 12.5% (p = 0.074). In 16 (17.8%) cirrhotic patients with TIPS who underwent LT after TIPS had a non-significant reduction of 52.0% in the risk of death. The expected survival benefit of LT in patients with cirrhosis and TIPS did not reach statistical significance.
A time-dependent Cox regression model was cons-tructed to directly quantify the impact of LT on survival (Table 3). This analysis correctly accounts for a patient's transition from the "pre-transplant" to the "post-transplant" state over time. The model was built on 106 patient-periods with 90 patients, in which 26 deaths occurred (Figure 5). Based on 90 subjects and 106 patient-periods and after adjusting for baseline patient characteristics, patient age was the only significant independent predictor of overall mortality in this final model (HR 1.06 per year; 95% CI, 1.02-1.10; p = 0.006).
Table 3 Time-dependent Cox regression analysisa of mortality in cirrhotic patients with TIPS compared to patients with TIPS with or without LT
| Description | HR | 95% CI | p |
|---|---|---|---|
| Age | 1.06 | 1.02-1.10 | 0.006 |
| Sex, women vs. men | 0.52 | 0.21-1.29 | 0.160 |
| MELD score, per point | 1.05 | 0.99-1.12 | 0.100 |
| PTE, yes vs. no | 1.14 | 0.45-2.89 | 0.785 |
| LT, as an event | 0.48 | 0.11-2.14 | 0.330 |
aModel based on 90 subjects and 106 patient-periods. TIPS: transjugular intrahepatic portosystemic shunt; MELD: model for end-stage liver disease; PTE: pre-TIPS encephalopathy; LT: liver transplantation; HR: hazard ratio; CI: confidence interval.
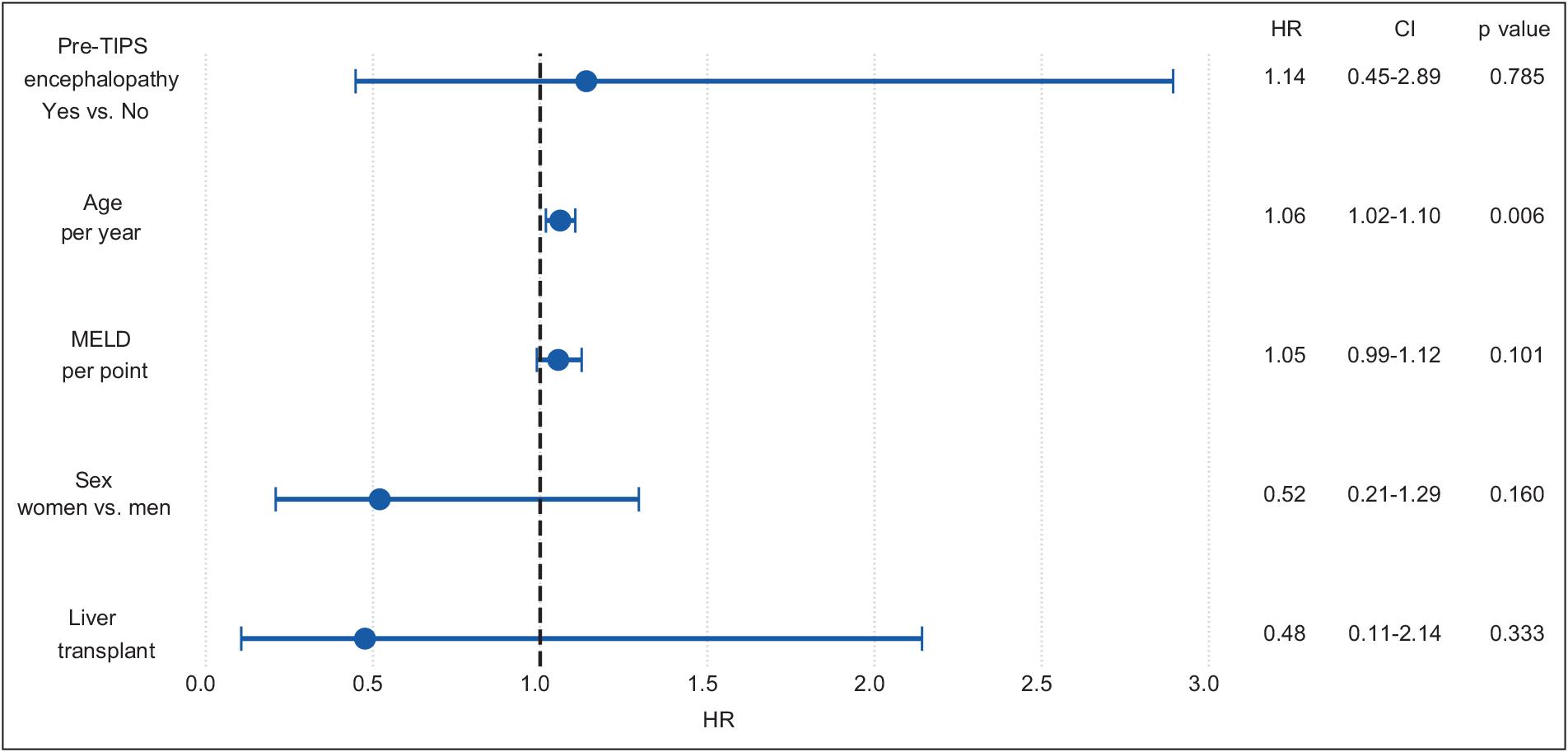
LT: liver transplantation; TIPS: transjugular intrahepatic portosystemic shunt; MELD: model for end-stage liver disease; HR: hazard ratio; CI: confidence interval.
Figure 5 Time-varying covariate analysis. In this model, patient age remains the only significant independent predictor of overall 5-year mortality (HR,1.06 per year; 95% CI, 1.02-1.10; p = 0.006).
LT in cirrhotic patients with TIPS was associated with a non-significant 52.0% reduction in the risk of death (HR, 0.48; 95% CI, 0.11-2.14; p = 0.33). The wide confidence interval suggests that although a large beneficial effect of LT in cirrhotic patients with TIPS was possible, the study was underpowered to prove this with statistical certainty. The effects of the MELD score, sex, and pre-TIPS encephalopathy were not statistically significant.
DISCUSSION
In our study, the 5-year mortality in cirrhotic patients with TIPS was 32.3%. We found that OHE and older age were significantly associated with a higher 5-year mortality in these patients, regardless of whether they underwent LT. This study is the first in Mexico on a cohort of cirrhotic patients with TIPS. We believe that TIPS, a more feasible intervention in our healthcare system, should be considered as a recommended therapeutic strategy.
The reported all-cause mortality during follow-up between 1 and 10 years in cirrhotic patients with TIPS varies widely (16.8 to 67.3.%)2,8,15-19. Five-year cumulative mortality and TIPS patency or dysfunction were evaluated in a retrospective single-center cohort study from Germany, including 228 cirrhotic patients with TIPS treated with ePTFE-covered stents (Viatorr®). The authors found a mortality rate of 31.3% (n = 71) at 1 year, 38.7% (n = 88) at 2 years, and a cumulative 5-year mortality of 57.3% (n = 130)16. Sonavane et al.17 conducted a prospective observational study in India of 42 patients with Budd-Chiari syndrome managed with TIPS and reported a cumulative mortality of 14% (n = 6) at 1 year, 19% (n = 8) at 5 years, and 24% (n = 10) at 10 years. Li et al.8 published a Chinese retrospective cohort of 132 cirrhotic patients with TIPS. They found a cumulative mortality rate of 7.6% (n = 10) at 1 year, 14.7% (n = 19) at 3 years, and 19.8% (n = 26) at 5 years. In our study, the overall 5-year mortality of 32.3% for cirrhotic patients with TIPS was consistent with internationally reported rates.
OHE is a known event after TIPS in cirrhotic patients due to shunt-induced changes in hepatic clearance of neurotoxins; however, its prognostic impact on mortality remains controversial3,5,8,20,21. Nardelli et al.3 in a multicenter observational study of 614 patients with cirrhosis undergoing TIPS in three Italian hospitals found that 293 (47%) of 614 patients developed at least one episode of OHE; 27 (9.2%) experienced recurrent/persistent OHE. The authors concluded that an OHE episode after TIPS was not associated with mortality in patients who underwent TIPS. In contrast, Xiang et al.20 conducted a multicenter retrospective study in 7 medical centers in China that showed the presence of OHE in 1076 (33.2%) of their 3262 cirrhotic patients with TIPS. Their study showed a mortality of 19.3% in patients with OHE. In our study, 5-year mortality was higher in patients with OHE (60.0%) than in patients without OHE (26.2%), showing a statistically significant association (p = 0.001). Our results, which are consistent with other published data3,5,20, showed that OHE is significantly associated with mortality and should not be underestimated as a prognostic factor.
While patient selection has traditionally relied on the severity of liver disease, such as the MELD and Child-Pugh scores, age has not been considered in most prognostic models. However, it has been shown to be an independent determinant of survival after TIPS8,22-24. Multivariate models consistently identify age as a predictor of short- and long-term mortality8,23,24. This effect may be related to a reduced physiologic reserve, a higher burden of comorbid conditions, and increased susceptibility to TIPS-related complications such as OHE. Regarding age in cirrhotic patients, Ascha et al.24, in a retrospective study at the Cleveland Clinic, exami-ned 418 patients with portal hypertension undergoing TIPS. They reported a 2% increased risk of death per year with patient age (HR: 1.02, 95% CI, 1.01-1.03, p = 0.004). The results of our study are consistent with those of Saad et al.23 and Ascha et al.24 in that older patients have a poor prognosis compared to the ≤ 65-year-old Mexican population. The studies differ in the thresholds chosen for prognostic assessment, which limits the direct comparability of the results. In addition, there is no consensus on an upper age limit for TIPS in cirrhotic patients. Consequently, including age in the pre-TIPS risk assessment could improve prognosis and enable individualized decision-making, balancing the potential hemodynamic benefits against the increased mortality risk in older patients.
The role of TIPS in conjunction with LT is being investigated as the two procedures overlap in terms of patient population and prognostic factors. Pre-transplant TIPS may optimize hemodynamics, control ascites, and reduce complications related to portal hypertension at the time of LT, which could facilitate surgery and improve early postoperative stability25. Mumtaz et al.25, in a retrospective cohort in the United States that included 32,783 patients on a United Network for Organ Sharing (UNOS) LT waiting list, showed that 1366 (4%) had TIPS, while a subset of patients were transplanted. TIPS had no effect on 30-day mortality after LT after logistic regression (OR = 1.26; 95% CI: 0.91-1.75). Another observational study suggested a potential survival benefit in selected candidates, particularly if TIPS effectively controls pre-LT portal hypertension complications26. The survival benefit of LT in cirrhotic patients after TIPS is not statistically proven, probably due to the relatively small number of transplanted patients and the fact that many TIPS studies censor outcomes at the time of LT20,22-24. In a Mexican LT cohort of 92 patients described by Hinojosa-Gonzalez et al.27, 9% (n = 9) had a TIPS before LT; similar mortality rates were found when comparing the TIPS group with the non-TIPS group over 2 years. Heinzow et al.28, in a retrospective single-center study conducted at a tertiary-care referral center in Germany that included 88 patients who underwent TIPS, 8 (10%) had LT. Survival in patients with TIPS before LT of more than 5 years improved in a univariate analysis (p = 0.024), but it was not an independent predictor in multivariate models. Our findings align with the existing literature, showing that LT after TIPS improves patient survival20-24. In our cohort, 16 (17.8%) patients who underwent LT after TIPS had a non-significant 52.0% reduced risk of death (HR, 0.48; 95% CI, 0.11-2.14; p = 0.33). Although this result is consistent with the expected survival benefit of LT in patients with cirrhosis and TIPS, the effect did not reach statistical significance. It may be underestimated due to the small sample size and the presence of competing risk factors for mortality.
This study has several strengths. First, it addresses the clinical relevance of TIPS in the Mexican population, a setting for which few data are available. Second, the procedure was performed using a standardized technique by an experienced interventional radiology team, ensuring consistency between cases. Third, validated statistical methods, such as Cox proportional hazards analysis and Kaplan-Meier analysis, were employed to evaluate survival and risk factors, enabling a comprehensive assessment of outcomes in cirrhotic patients with TIPS.
This study also has limitations that need to be considered. The small sample size and the retrospective nature of the study have the potential for selection bias. The lack of a control group without TIPS limits a direct comparison of the results with those of standard of care. There may also be exclusion bias, as patients from remote areas or lower socioeconomic backgrounds often have limited access to healthcare. This fact reflects the general inequalities in access to advanced procedures such as TIPS within the Mexican public health system, where high costs limit availability. Finally, the study relied on a dichotomous definition of OHE, which may not fully capture the clinical spectrum of this complication. Some recognized predictors of mortality in cirrhotic patients with TIPS were not available due to missing data. On the other hand, the LT analysis was limited by the small number of procedures during the follow-up period.
CONCLUSION
In our study, the 5-year mortality rate for cirrhotic patients with TIPS was 32.3%. Mortality was significantly associated with OHE and older age. We found no significant difference in outcomes in cirrhotic TIPS patients with or without a LT. Our findings are consistent with international mortality rates for TIPS patients and support the use of prognostic factors for monitoring and assessing mortality risk. Further prospective studies with control groups are needed to determine the survival impact of TIPS on cirrhotic patients with and without a LT.

