











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Hepatocellular carcinoma (HCC) remains the most prevalent primary liver malignancy worldwide and continues to pose a significant global health burden due to its dismal prognosis1,2.
The treatment of HCC is usually a clinical challenge due to the complexity of its management and the concurrent diagnosis of chronic liver disease2. For patients with HCC who meet transplantation criteria, the preferred curative options are liver transplant or resection, with reported 5-year survival rates of 75-80%2,3. However, many patients receive their diagnosis at an advanced stage, precluding surgical or ablative options and leading to systemic therapies4. Although there is no standard treatment for unresectable HCC, patients presenting with an intermediate HCC, classified as Barcelona Clinic of Liver Cancer (BCLC) stage B, are considered good candidates for trans-arterial embolization techniques5.
One of the hallmarks of HCC is tumoral neoangiogenesis which confers its classic pattern of arterial hypervascular enhancement and venous washout on dynamic imaging3. Since these tumors receive most of their blood supply through the hepatic artery, intra-arterial therapies represent the mainstay of treatment for such patients6. Among the available therapies, transarterial embolization (TAE) and transarterial chemoembolization (TACE) are the two main locoregional treatment options3. Both procedures lead to tumor ischemia and inhibition of tumor growth through tumor blood flow shutdown7. TACE involves a dual process of intra-arterial chemotherapy infusion combined with embolization6,7, aimed at selectively targeting the tumor while minimizing damage to healthy liver tissue6. In contrast, TAE aims to achieve the occlusion of tumor-feeding vessels without the addition of chemotherapeutic agents5,7. Both TACE and TAE induce tumor necrosis at rates in the range of 16-60%8,9. Although TACE is the most common procedure for the treatment of intermediate-stage HCC3, scarce data from observational studies and randomized clinical trials (RCT) have demonstrated any superiority of this approach over TAE9-16. Therefore, the most effective transcatheter embolization strategy for unresectable HCC is still uncertain, as confirmed by recent meta-analyses17-20. In this study, we sought to compare the effectiveness and liver-related complications of these two procedures in a real-world setting using a propensity score matching (PSM) analysis.
Methods
Patient selection
Patients with HCC diagnosed by histology or by non-invasive criteria at imaging based on European Association for the Study of the Liver guidelines, with a BCLC stage A or B, considered not resectable, not candidates for liver transplantation, and not amenable to ablation were retrospectively identified from electronic clinical records. We included all patients who underwent TACE or TAE as primary treatment for HCC, as indicated by a multidisciplinary tumor board (MTB) in two referral centers from January 2018 to December 2021. Patients were required to have a Child-Pugh score A or B and a performance status Eastern Cooperative Oncology Group (ECOG) 0 or 1. Patients who had one of these procedures as a bridge to liver transplantation were also selected. We excluded patients with any prior trans-arterial or local procedure. Any additional TAE/TACE or systemic therapy was recommended to some patients depending on tumor response and liver function, after discussion in the MTB.
Clinical characteristics were collected from medical electronic records. Patients were followed up with post-operative imaging (liver magnetic resonance imaging or computed tomography scan) every 4-6 months or clinically indicated to assess tumor response. The primary outcome was overall survival (OS). The safety outcome was the frequency of hepatic decompensation, defined by an increase of at least one point in the Child-Pugh score 1 month after the procedure. Per local protocols, patients with hepatic decompensation were not allowed to receive any further endovascular intervention.
Trans-arterial procedures
Patients were treated with trans-arterial therapy following standard local protocols. TACE using epirubicin was the standard of care for trans-arterial treatment in two hospitals, whereas TAE using lipiodol was the standard of care for patients in other.
In the case of TACE, 20 mg of epirubicin were either loaded on 100 μm drug-eluting beads (100 μm; Embozene Tandem® microspheres, Celonova Biosciences, Ulm, Germany), or manually emulsified with 5-10 mL of ethiodized oil (Lipiodol® Ultra Fluide, Guerbet, France) as previously described16. In lipiodol TACE, drug administration was immediately followed by embolization using biocompatible, hydrophilic, non-absorbable, and acrylic polymer microspheres impregnated with porcine gelatin (Embosphere Merit Medical Systems, UT, USA) under fluoroscopic control.
In the case of TAE, 10-15 mL of pure ethiodized oil (Lipiodol® Ultra Fluide, Guerbet, was injected through the catheter as selective as possible. This procedure was followed by embolization with Embospherel® microspheres of 300-500 um (Merit Medical Systems, UT, USA) until complete stasis of the arterial flow.
Statistical analysis
Descriptive categorical variables are presented as frequencies and percentages, or as means ± standard deviations in case of continuous variables. Categorical variables were compared through the Chi-square test, or Fisher test when indicated. Comparisons among baseline characteristics were performed before and after the PSM.
Since TAE and TACE procedures were not randomly assigned in the studied population, a PSM was used to reduce the influence of potential confounding variables between both groups. Patients were matched to receive one of these therapies based on a propensity score estimated by a multivariable logistic regression model, in which the TACE procedure was the dependent variable and the following baseline characteristics were used as covariates: Child-Pugh score, sex, and ECOG performance status. The PSM was performed using a 1:1 matching without replacement (Greedy-matching algorithm).
The primary outcome was OS as measured from the date of first TACE/TAE until death according to the National Registry System. The association between endovascular therapies (TAE or TACE) and OS was examined using a Kaplan-Meier survival curve. The log-rank test was used to compare the distributions of OS among therapies after adjustment using a PSM (1:1 greedy nearest-neighbor matching). An univariate Cox proportional-hazard regression model was used to determine the hazard ratio (HR) and its corresponding 95% confidence interval (CI) for the association between OS and the endovascular treatment received. The model was also adjusted for ECOG, Child-Pugh score, and age as covariates. The odds ratio (OR) and its 95% CI was used to measure the association between liver decompensation and the trans-arterial procedure. p < 0.05 was considered statistically significant. All the analyses were performed using the Statistical Analysis System (SAS)® software version 9.3 (SAS Institute Inc. Cary, NC, USA). The STROBE Guidelines were followed in reporting this observational study. The Institutional Review Board approved this protocol (R023-SABI-0337).
Results
General characteristics
During the study period, a total of 114 patients underwent TAE (n = 41; 35.9%) or TACE (n = 73; 64.1%). Clinical characteristics of the studied population before and after PSM are summarized in table 1. Most patients were male (n = 74, 64.9%), with a mean age of 68.5 ± 8.7 years, good performance status (ECOG 0-1: n = 102; 89.5%), and a BCLC stage of B (n = 87, 76.3%). All patients had chronic liver disease and 42.5% (n = 31) of them had clinical signs of portal hypertension. Most patients had metabolic-associated fatty liver disease as underlying hepatic disease (n = 72, 63.2%). After PSM, 76 patients were included in the analysis.
Table 1 General characteristics of the studied population before and after the propensity score matching
| Variable | Before PSM | p | After PSM | p | ||
|---|---|---|---|---|---|---|
| Trans-arterial procedure | Trans-arterial procedure | |||||
| TAE, n = 41 (35.9) | TACE, n = 73 (64.1) | TAE, n = 38 (50) | TACE, n = 38 (50) | |||
| Sex, n (%) | 0.03 (χ2 = 8.95) | 0.99 (χ2 = 0.12) | ||||
| Male | 32 (43.2) | 42 (56.8) | 29 (50) | 29 (50) | ||
| Female | 9 (22.5) | 31 (77.5) | 9 (50) | 9 (50) | ||
| Age, n (%) | 0.19 (χ2 = 6.125) | 0.17 (χ2 = 6.42) | ||||
| < 55 years | 0 | 11 (100) | 0 | 4 (100) | ||
| 55-70 years | 19 (41.3) | 27 (58.7) | 16 (59.3) | 11 (40.7) | ||
| > 70 years | 22 (38.6) | 35 (61.4) | 22 (28.2) | 23 (71.8) | ||
| ECOG (%) | 0.001 (χ2 = 16.27) | 0.04 (χ2 = 8.31) | ||||
| 0 | 28 (58.3) | 20 (41.7) | 26 (78.8) | 7 (21.2) | ||
| 1 | 13 (19.7) | 53 (80.3) | 12 (27.9) | 31 (72.1) | ||
| Underlying liver disease, n (%) | 0.44 (χ2 = 5.85) | 0.45 (χ2 = 5.77) | ||||
| Alcoholic liver disease | 5 (23.8) | 16 (76.2) | 5 (38.5) | 8 (61.4) | ||
| MAFLD | 28 (38.9) | 44 (61.1) | 27 (51.9) | 25 (48.1) | ||
| Autoimmune hepatitis | 1 (50) | 1 (50) | 1 (100) | 0 | ||
| Chronic HBV | 2 (28.6) | 5 (71.4) | 2 (50) | 2 (50) | ||
| Chronic HCV | 3 (75) | 1 (25) | 2 (100) | 0 | ||
| Other | 2 (28.6) | 5 (71.4) | 1 (25) | 3 (75) | ||
| Child-Pugh score, n (%) | 0.11 (χ2 = 7.54) | 0.99 (χ2 = 0.12) | ||||
| A | 33 (39.8) | 50 (60.2) | 31 (50) | 31 (50) | ||
| B | 7 (23.2) | 23 (76.7) | 7 (50) | 7 (50) | ||
| C | 1 (100) | 0 | 0 | 0 | ||
| Barcelona clinic liver cancer stage, n (%) | 0.55 (χ2 = 2.11) | 0.99 (χ2 = 0.12) | ||||
| A | 11 (40.7) | 16 (59.3) | 10 (50) | 28 (50) | ||
| B | 30 (34.5) | 57 (65.5) | 10 (50) | 28 (50) | ||
| Alpha-fetoprotein, n (%) | 0.66 (χ2 = 1.59) | 0.77 (χ2 = 1.13) | ||||
| > 400 ng/dL | 35 (36.8) | 60 (63.2) | 32 (50.8) | 31 (49.2) | ||
| < 400 ng/dL | 6 (31.6) | 13 (68.4) | 6 (46.2) | 7 (53.8) | ||
| TAE/TACE as a bridge for liver transplantation (%) | 1 (10) | 9 (90) | 0.09 (χ2 = 6.49) | 1 (33) | 2 (66) | 0.56 (χ2 = 2.06) |
PSM: propensity score matching; TAE: trans-arterial embolization; TACE: trans-arterial chemoembolization; ECOG: Eastern Cooperative Group; MAFLD: metabolic associated fatty liver disease; HBV: hepatitis B virus; HCV: hepatitis C virus.
Efficacy and safety outcomes
After a median follow-up of 17.9 months, a total of 72 patients died (63.2%). Median OS for the whole population was 19.9 months (95% CI: 15.8-26.2 months). The probability of survival at 3 years was 32%. As depicted in figure 1, there was no significant difference between the probability of OS between patients who received TAE or TACE as endovascular treatment for HCC (HR: 1.19; 95% CI: 0.64-1.96 p = 0.69). Table 2 shows the results of the multivariate analysis for OS. After adjusting for potential confounders, only the Child-Pugh score (B vs. A) was associated with poor OS (median OS 15.5 vs. 23.3 months, respectively).
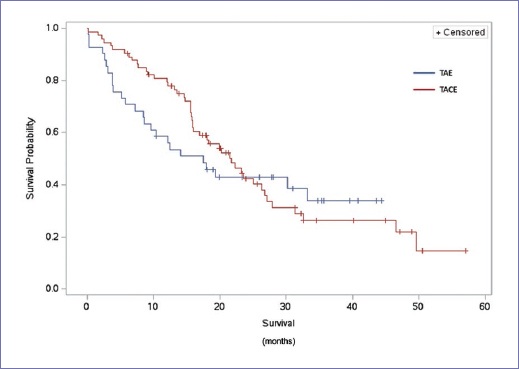
Figure 1 Overall survival for patients receiving trans-arterial chemoembolization or trans-arterial embolization according to the Kaplan-Meier method.
Table 2 Multivariate analysis for overall survival after propensity score matching analysis
| Variable | Hazard ratio (95% CI) | p |
|---|---|---|
| Sex (female vs. male) | 0.98 (0.50-1.92) | 0.95 |
| ECOG performance status (0 vs. 1) | 0.52 (0.18-1.55) | 0.235 |
| Child-Pugh score (A vs. B) | 0.32 (0.15-0.66) | 0.002* |
| Type of treatment (TACE vs. TAE) | 1.68 (0.84-3.33) | 0.138 |
CI: confidence interval; ECOG: Eastern Cooperative Group; TAE: trans-arterial embolization; TACE: trans-arterial chemoembolization.
Hepatic decompensation occurred in 9 (23.7%) and 3 (7.9%) patients who underwent TACE and TAE, respectively (OR TACE vs. TAE: 3.7; 95% CI: 0.90-14.62; p = 0.06). Among patients with hepatic decompensation, the most frequent event was grade I hepatic encephalopathy (n = 5), followed by worsening ascites (n = 4) and transient hyperbilirubinemia (n = 3). Similarly, infectious complications were numerically more common after TACE compared with TAE, although the difference was not statistically significant (13.2 vs. 5.3%; OR: 2.27; 95% CI, 0.4915.01; p = 0.23). Infectious complications included nosocomial pneumonia (n = 5), urinary tract infection (n = 3), and spontaneous bacterial peritonitis (n = 2). Other uncommon adverse events included hepatorenal syndrome in one patient treated with TACE and variceal bleeding in one patient from each treatment group.
Discussion
The findings of our study showed comparable OS and liver-related complications among patients receiving TAE or TACE for unresectable HCC. RCTs and observational studies comparing conventional TACE and TAE have shown conflicting results in determining the superiority of one technique over the other10-16. For instance, one RCT comparing TACE, TAE, and best supportive care (BSC) was prematurely closed due to the superiority of TACE over BSC, and it was not powered enough to determine the efficacy of TACE over TAE11. On the other hand, another RCT concluded that the addition of cisplatin did not enhance the therapeutic effect of TAE for the treatment of patients with unresectable HCC16. Similarly, a recent trial also failed to show the superiority of TACE (using doxorubicin-eluting microspheres) over bland embolization14.
Although the heterogeneity of the included patients in each trial can explain the aforementioned differences among studies, our results are in line with the null effect of chemotherapy when added to selective arterial embolization. Indeed, four recent reviews and meta-analyses found no conclusive evidence to support TAE or TACE for these patients17-20. Some authors have argued that available trials comparing bland embolization to TACE are inconclusive since they include populations that do not match the profile of patients for whom TACE would be recommended5. Besides, the selection criteria for these endovascular techniques are broad, from bridge or downstaging to liver transplantation to patients unsuitable for surgery. In contrast, our population was composed only by patients with a BCLC stage of A and B, for whom a MTB indicated TACE or TAE based on clinical judgment and current guidelines5. Hence, our results can adequately compare both procedures in a cohort of patients with a clear indication for the intravascular procedure, excluding subjects with vascular invasion, extrahepatic disease, or diffuse or extensive liver involvement.
Although the relatively small sample size of this analysis can affect the precision of our findings, and the retrospective design can arise some concerns regarding selection and informative bias, we were able to provide a fair comparison between both intra-arterial procedures in a cohort of patients from a real-world scenario, which frequently differs from the setting of a RCT. Indeed, previous studies have indicated that selection criteria of HCC patients for intra-arterial procedures are usually broader in real clinical practice in comparison to those criteria suggested by clinical guidelines21.
Although other cohort studies have reported similar results to ours regarding the inconclusive superiority of one of the intra-arterial procedures over the another13, the selection of a PSM in this research enhances the comparability between both comparison arms. Given these contradictory results and the absence of superiority of one technique over the other, many authors coincide that the effects of embolic therapies derive mainly from tumor ischemia produced by occlusion of the arterial vessels and that the addition of chemotherapy has little effect on tumor control3.
It has also been argued that TACE may incite more liver damage than bland embolization especially when conducted in a non-selective manner. Common side effects of liver embolization include fever, pain, and transient elevation of aminotransferases and bilirubin levels. More serious complications can also be present such as hepatic and kidney failure, sepsis, and death. Although our findings showed a higher percentage of patients with liver decompensation after TACE versus TAE, these differences were not statistically significant. Of note, all intra-arterial procedures were performed by well-trained interventional radiologists who prefer ultra-selective embolization in all cases when feasible, which lower the probability of side effects. Besides, the assessment of hepatic decompensation was performed 1 month after the procedure, and previous studies have confirmed that hepatic impairment is usually transient and self-limited22.
The decision to use OS as a primary endpoint responds to the interobserver variation during the evaluation of response after TAE/TACE, which makes less reproductible the assessment of progression23. Besides, in real-world studies, OS is a more appropriate endpoint since it is less prone to information bias. In addition, some authors have argued against the use of progression-free survival as a valid surrogate efficacy outcome in patients with HCC due to its vulnerability to interpretation bias and low correlation with OS24.
Of note, the 3-year OS rate in this cohort was inferior to the reported by recent series (33 vs. 55 to 66%)3, probably due to low access to medical therapies after TAE/TACE failure.
In conclusion, our findings demonstrated comparable long-term outcomes and liver-related complications in patients treated with TAE or TACE for HCC.
In the absence of new RCTs comparing these two strategies, our results are useful to challenge the routine use of chemotherapy-eluting beads or lipiodol chemoembolization for the treatment of patients with BCLC-A or BCLC-B HCC.
Conclusion
In this real-world retrospective analysis, TACE and TAE showed comparable efficacy after propensity score matching.

