











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Cancer encompasses a heterogeneous group of diseases, defined by the type and location of the primary tumor1. The increasing global burden of cancer underscores the need for efficient clinical management strategies that ensure timely, accurate, and coordinated interventions. These strategies must be patient-centered and adhere to the highest technical and scientific standards across all stages of care, aiming to reduce cancer incidence, disability, mortality, and improve quality of life at both the population and individual levels2-4.
Cancer care is inherently complex, involving not only diagnosis and treatment but also the integration of various components of the health system to provide continuous and comprehensive care5. Delays at any point along this care continuum-from initial symptom presentation to the initiation of definitive treatment-can significantly compromise clinical outcomes6. These delays may be driven by limitations in healthcare infrastructure, socioeconomic disparities, and unequal access to specialized services. Addressing these challenges requires a system-level approach that integrates advances in diagnostics, treatment modalities, and healthcare delivery models to ensure timely and equitable access for all patients1.
The high complexity of oncologic therapies, combined with barriers in accessing healthcare services or logistical constraints within oncology departments, often contributes to delays in care. These factors have played a role in maintaining elevated cancer mortality rates in Latin America, leading the World Health Organization to emphasize the importance of early cancer diagnosis programs, particularly in low- and middle-income countries7.
In Colombia, the general system of social security in health (SGSSS) provides universal coverage through a managed competition model involving public and private insurers (Entidades Promotoras de Salud), which contract services from healthcare providers (Instituciones Prestadoras de Salud). Although the system is designed to ensure access to healthcare, it is frequently challenged by bureaucratic inefficiencies, delays in authorization, prolonged waiting times for specialist consultations, and fragmented referral pathways. These structural deficiencies can result in significant delays across the cancer care continuum8.
Several local studies have identified barriers to timely oncology care in Colombia, particularly concerning breast and cervical cancer9,10. However, these investigations often have limited scope, focusing on single institutions, specific regions, or particular cancer types. Moreover, there is a lack of research evaluating how administrative processes within the insurance-based healthcare model impact the timeliness of diagnosis and treatment initiation. This represents a substantial gap in the literature.
To address this gap, the present study evaluates delays in cancer diagnosis and treatment initiation among patients affiliated with a Health Benefit Plan Administrator (Entidad Administradora de Planes de Beneficios) and explores their association with patients’ clinical characteristics. Given that timely access to oncologic care and effective coordination across services are fundamental for improving outcomes, this study aims to assess delays in diagnosis and treatment initiation, and their relationship with clinical characteristics of cancer patients affiliated with a health benefit management entity.
Materials and methods
A cross-sectional analytical study was conducted between January and July 2023, involving patients with a confirmed pathological diagnosis of cancer. Inclusion criteria required affiliation with the healthcare insurer under study, which operates under a vertical integration model, allowing for comprehensive traceability and consolidation of clinical information. Patients with a prior cancer diagnosis were excluded, as the focus was exclusively on the management of their present condition. All participants were residents of the northeastern region of Colombia.
No formal sample size calculation was performed; instead, a census approach was used, including all consecutive patients who met the eligibility criteria during the study period. This 6-month timeframe was selected to analyze delays in diagnosis and treatment within a defined temporal window. Patients were identified through electronic medical records using ICD-10 codes corresponding to malignant neoplasms.
The variables analyzed included age at diagnosis, cancer type, social security scheme, sex, clinical stage of the disease, municipality of residence, patient type (prevalent or incident), and the four delays11. The four-delay methodology was adopted to define delays: Type I lack of problem recognition refers to the patient’s failure to recognize the seriousness of symptoms or the need to seek medical attention, often due to limited awareness or knowledge. Type II: lack of timely decision-making and action involves sociocultural, geographical, or economic barriers that hinder timely access to health services. Type III: lack of access to care and referral logistics refers to logistical barriers and limitations in accessing a healthcare institution equipped to provide necessary services. Type IV: failure in the quality of care from primary to tertiary levels. This includes delays in receiving appropriate and timely treatment, related to the quality of care provided at lower levels of the health system (Figure 1).
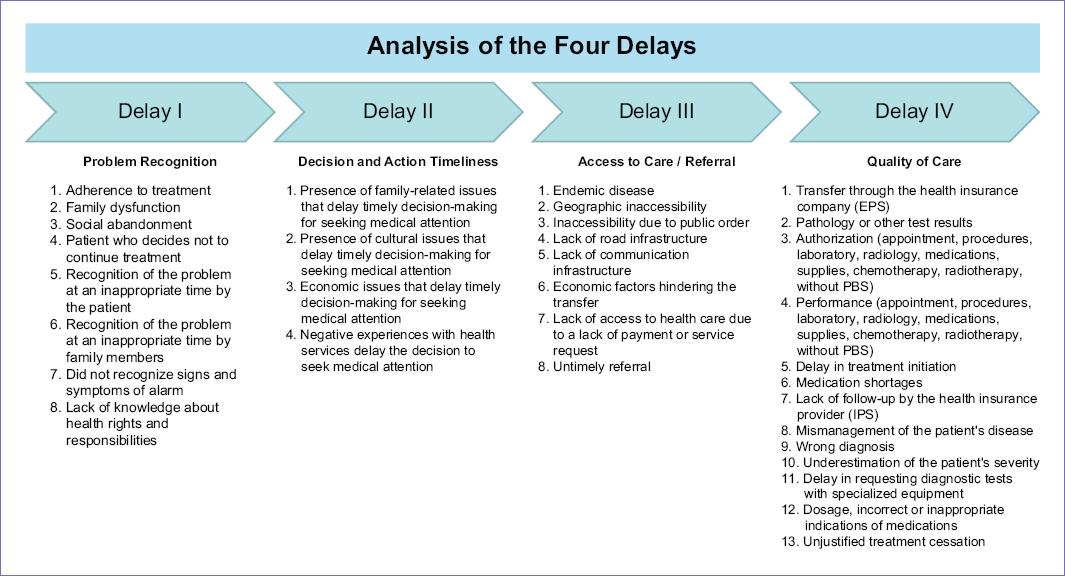
Figure 1 Definition of the four-delay analysis. Source: based on the general methodology of the unit of analysis for special cases related to public health events of interest.
To determine whether a patient experienced a delay, we used reference indicators for timely diagnosis and treatment initiation as defined by the Colombian Ministry of Health and Social Protection in Resolution 3339 of 2019, specifically for prioritized cancers12 (Table 1).
Table 1 Timelines established by the Ministry of Health and Social Protection of Colombia-high-cost account for prioritized cancers according to resolution 3339 of 2019
| Location | Timelines for timely intervention | Compliance range | ||
|---|---|---|---|---|
| Breast/cervix | Diagnostic opportunity in cancer | = 30 days | = 45 and > 30 days | > 45 days |
| Opportunity for treatment initiation | = 15 days | = 30 and > 15 days | > 30 days | |
| Prostate/colon and rectum/stomach/lung | Opportunity for diagnosis | = 30 days | = 30 - < 60 days | = 60 days |
| Opportunity for treatment | = 30 days | = 30 -< 60 days | = 60 days | |
| Melanoma | Opportunity for diagnosis | = 30 days | 31-44 days | = 45 days |
| Opportunity for treatment | = 30 days | 31-44 days | = 45 days | |
| Non-Hodgkin lymphoma | Opportunity for diagnosis | = 15 days | = 15 - < 30 days | = 30 days |
| Opportunity for treatment | = 30 days | = 30 - < 60 days | = 60 days | |
| Hodgkin lymphoma | Opportunity for diagnosis | = 15 days | = 15 - < 30 days | = 30 days |
| Opportunity for treatment | = 30 days | = 30 - < 60 days | = 60 days | |
| Acute myeloid leukemia | Opportunity from diagnosis to treatment, CNR | = 5 days | - | > 5 days |
| Opportunity for transplantation, CNR | To be defined | |||
| Acute lymphoid leukemia | Opportunity from diagnosis to treatment, CNR | = 5 days | - | > 5 days |
| Opportunity for transplantation, CNR | To be defined | |||
Source: dictionary of indicators consensus and risk-HIGIA-CAC.
Data collection was managed using the Research Electronic Data Capture, ensuring secure and efficient data handling. Each patient’s medical record was reviewed by trained personnel to ensure data accuracy and consistency. Delay classification was also conducted by trained reviewers. In cases where classification was uncertain, the final categorization was determined by consensus among the authors. Discrepancies were resolved promptly through collaborative review. For missing data, efforts were made to recover information through additional medical records or by contacting healthcare professionals involved in the patients’ care. Records with irretrievably missing data were excluded from the analysis to preserve the integrity of the results.
Descriptive statistics were applied to characterize the study population. Categorical variables, including delay types, were presented as absolute frequencies and percentages. For continuous variables, normality was assessed using the Shapiro-Wilk test. Variables with a normal distribution were reported as means and standard deviations, while non-normally distributed variables were described using medians and interquartile ranges. Bivariate analyses were performed using the ?2 test or Fisher’s exact test, as appropriate. Statistical analyses were performed using STATA software, version 16.
Ethical statement
This study complied with international ethical standards and was based on secondary data from routine clinical care, without altering medical management or exposing patients to additional risks. The study protocol was reviewed and approved by the Institutional Scientific and Research Ethics Committees, ensuring adherence to ethical research principles.
Results
A total of 102 patients were included in the analysis. The median age was 61 years, and the majority were female (66.7%). Most participants (70.6%) were affiliated with the contributory health insurance regime. Incident cases accounted for 83.3% of the sample, and 88.2% of patients presented with solid tumors. The most common cancer types were skin cancer (18.6%), breast cancer (12.8%), and prostate cancer (10.8%). Among solid tumors, stage III was the most frequently observed (17.8%), followed by stage I (16.7%) (Table 2).
Table 2 Participant characteristics
| Category | No. (%) |
|---|---|
| Age (median IQR) | 61 (46-72) |
| Sex | |
| Female | 68 (66.7) |
| Male | 34 (33.3) |
| Regimen | |
| Contributory | 72 (70.6) |
| Subsidized | 30 (29.4) |
| Diagnosis | |
| Incident | 85 (83.3) |
| Prevalent | 17 (16.7) |
| Pathology classification | |
| Hematological | 12 (11.8) |
| Solid tumors | 90 (88.2) |
| Staging (solid) | |
| In situ | 7 (7.8) |
| I | 15 (16.7) |
| II | 12 (13.3) |
| III | 16 (17.8) |
| IV | 10 (11.1) |
| No date | 14 (15.6) |
| Diagnostic group | |
| Skin | 19 (18.6) |
| Breast | 13 (12.8) |
| Prostate | 11 (10.8) |
| Thyroid gland and other glands | 9 (8.8) |
| Female genital organs | 9 (8.8) |
| Colon and rectum | 8 (7.8) |
| Cervix | 8 (7.8) |
| Non-Hodgkin lymphoma | 6 (5.9) |
| Digestive organs | 4 (3.9) |
| Stomach | 3 (2.9) |
| Urinary tract | 3 (2.9) |
| Chronic myeloid leukemia | 2 (1.9) |
| Trachea, bronchi, and lungs | 2 (1.9) |
| Acute lymphoid leukemia | 1 (0.9) |
| Acute myeloid leukemia | 1 (0.9) |
| Multiple myeloma and malignant plasma cell tumors | 1 (0.9) |
| Eye, brain, and other parts of the central nervous system | 1 (0.9) |
| Other classification | 1 (0.9) |
IQR: Interquartile range.
In this study, 83.3% were incident cases. Of the total population, 37.3% experienced delays in receiving pathology results or other diagnostic tests. These delays were significantly more frequent in incident cases (43.5%) than in prevalent cases (5.9%) (p = 0.001). Although most patients did not report delays in the authorization of procedures (99.0%) or the initiation of treatment (97.1%), delays in the execution of procedures were common, affecting 81.4% of patients. These delays were more frequent among incident cases (83.5%) compared to prevalent cases (70.6%), although the difference was not statistically significant (p = 0.18).
Delays related to problem recognition by patients or their families were relatively infrequent. Only 9.8% of participants reported a delay in recognizing the need for medical attention, with a slightly higher frequency in incident cases (11.8%) than in prevalent cases, though the difference was not statistically significant (p = 0.147). Other reported factors included lack of follow-up by healthcare institutions (9.8%), transfers to other insurers (3.9%), and referral or counter-referral delays (1.0%), none of which showed significant differences between groups (Table 3).
Table 3 Analysis of delays by incident and prevalent patients
| Type of delay | Total n = 102 (%) | Incident (n = 85) | Prevalent (n = 17) | p |
|---|---|---|---|---|
| Delay one: recognition of the problem | ||||
| Adherence to treatment | 2 (2.0) | 1 (1.6) | 1 (5.9) | 0.31 |
| Social abandonment | 1 (1.0) | 1 (1.2) | - | 0.83 |
| Patient decides not to continue treatment | 2 (1.8) | 1 (1.6) | 1 (5.9) | 0.31 |
| Late recognition of the problem by the patient | 10 (9.8) | 10 (11.8) | - | 0.15 |
| Late recognition of the problem by the family | 2 (2.0) | 2 (2.4) | - | 0.69 |
| Delay two: timeliness of decision and action | ||||
| Presence of family issues affecting timely decision to seek medical care | 1 (1.0) | - | 1 (5.9) | 0.17 |
| Delay three: access to care | ||||
| Referral and counter-referral (delays by personnel or family) | 1 (1.0) | 1 (1.6) | 1 (5.9) | 0.31 |
| Delay four: quality of care | ||||
| Transfer to EPS | 4 (3.9) | 2 (2.35) | 2 (11.8) | 0.13 |
| Results of pathology or other exams | 38 (37.3) | 37 (43.53) | 1 (5.9) | < 0.001 |
| Authorization* | 1 (1.0) | 1 (1.2) | 0 (0.0) | 0.83 |
| Execution* | 88 (81.4) | 71 (83.4) | 12 (70.6) | 0.18 |
| Delay in treatment initiation | 3 (2.9) | 3 (3.6) | 0 (0.0) | 0.58 |
| Lack of follow-up from IPS | 10 (9.8) | 8 (9.4) | 2 (11.8) | 0.52 |
*Appointments, procedures, labs, radiology, medications, supplies, chemotherapy, radiotherapy, non-PBS services. IPS: Instituciones Prestadoras de Salud.
An analysis of delays related to quality of care (Delay Type IV), comparing solid versus hematologic cancers, revealed statistically significant differences in treatment initiation. Patients with hematologic malignancies had a higher frequency of delays in treatment initiation (16.7%; n = 2), compared to those with solid tumors (1.1%; n = 1) (p = 0.04). Conversely, delays in the execution of procedures were more prevalent in patients with solid tumors (84.6%) than in those with hematologic cancers (58.3%) (p = 0.04). Delays in receiving pathology or test results were also more frequent in hematologic cancer patients (58.3%) compared to those with solid tumors (34.1%), although this difference did not reach statistical significance (p = 0.10). Family-related issues affecting timely decision-making were reported exclusively in hematologic cancer patients (8.3%), with a trend toward significance (p = 0.12) (Table 4).
Table 4 Analysis of delays and cancer type
| Type of delay | Hematologic (n = 12) | Solid tumor (n = 91) | p |
|---|---|---|---|
| Delay one: recognition of the problem | |||
| Adherence to treatment | - | 2 (2.2) | 0.78 |
| Social abandonment | - | 1 (1.1) | 0.83 |
| Patient decides not to continue treatment | - | 2 (2.2) | 0.78 |
| Late recognition of the problem by the patient | 2 (16.7) | 8 (9.8) | 0.33 |
| Late recognition of the problem by the family | - | 2 (2.2) | 0.78 |
| Delay two: timeliness of decision and action | |||
| Presence of family issues affecting timely decision to seek medical care | 1 (8.3) | - | 0.12 |
| Delay three: access to care | |||
| Referral and counter-referral (delays by personnel or family) | - | 2 (2.2) | 0.78 |
| Delay four: quality of care | |||
| Transfer to insurance provider | - | 4 (4.4) | 0.61 |
| Results of pathology or other exams | 7 (58.3) | 31 (34.1) | 0.10 |
| Authorization* | - | 1 (1.1) | 0.83 |
| Execution* | 7 (58.3) | 77 (84.6) | 0.04 |
| Delay in treatment initiation | 2 (16.7) | 1 (1.1) | 0.04 |
| Lack of follow-up from IPS | 1 (8.3) | 9 (9.9) | 0.67 |
*Appointments, procedures, labs, radiology, medications, supplies, chemotherapy, radiotherapy, non-PBS services.
Concerning the distribution of treatment delays by cancer type and stage, skin, breast, and prostate cancers showed the highest number of delays in stage IV, with 17, 11, and 11 cases, respectively. Overall, 87 delays (85.3%) occurred in stage IV, compared to 12 (11.8%) in stage I, 2 (2.0%) in stage III, and 1 (1.0%) in stage II. Supplementary table 1 highlights these findings, with red indicating the highest frequency of delays, green and yellow indicating low frequency or absence of delays, and no data recorded denoting missing data for certain groups.
Discussion
Cancer diagnosis at advanced stages remains a significant challenge for healthcare systems worldwide, leading to worse patient outcomes1. Early detection is crucial, as patients diagnosed in earlier stages typically experience better prognosis13. However, barriers at various levels, ranging from patient delays in seeking care to systemic issues in healthcare delivery, contribute to diagnostic delays, particularly in low- and middle-income countries14. Understanding the context surrounding delayed cancer diagnosis and treatment initiation is critical for improving patient outcomes and optimizing healthcare resources15.
The study included a majority of incident cancer cases, emphasizing the high prevalence of new cancer diagnoses within the study population and the urgent need for timely interventions1. The majority of participants were women, and although the age at diagnosis did not differ between incident cases and prevalent cases, the presence of advanced-stage cancer remains a relevant finding. A considerable proportion of cases were classified in advanced stages, with stage III being particularly prevalent16. This underscores the persistent barriers to early detection and timely diagnosis, which remain critical challenges in cancer care1.
Regarding the four types of delays, the most common and impactful for patients was delay type four: quality of care, accounting for 85.3% of the total delays. This was followed by delay type one: recognition of the problem, in third place was delay type three: access to care/referral, and finally, delay type two: timeliness of decision and action. This suggests that the most frequent delays affecting patients were those directly related to patient-driven issues and delays caused by healthcare providers within the care process17.
Significant differences were observed in delay type four, particularly in the subcategories related to pathology results. When analyzing the type of cancer, statistically significant differences were found in the initiation of treatment, with more delays in hematological cancers. The delays observed in hematological cancers (p = 0.04) are likely related to various factors, such as diagnostic complexity, treatment logistics, and, additionally, inefficiencies within the healthcare system. However, a more in-depth study is required to precisely determine the causes of these delays and their impact on patient outcomes. Minimizing delays in diagnosis and the initiation of treatment, as such delays can substantially impact patient survival and outcomes18.
These results are consistent with those reported in the systematic review association of treatment delays with survival for patients with head and neck cancer. This review found that the primary causes of delays were attributed to patient factors (e.g., failure to recognize symptoms as cancer-related) and professional factors (e.g., scheduling additional imaging or tests)19. Issues related to prolonged time to initiation of treatment appear to be more pronounced in academic medical centers, where patients are often diagnosed before referral and experience delays during the transition of care to the academic center20.
Comparing these findings with studies conducted in Colombia, a study in Bogotá identified similar delays, particularly in the recognition of symptoms and referral process, affecting the timely initiation of treatment in patients with breast and prostate cancer21. In addition, a study in Medellín found that diagnostic delays were associated with being enrolled in a state-subsidized regime and being older than 40 years for breast cancer22. These findings highlight the commonality of treatment delays within Colombia, where barriers at various levels-patient, healthcare provider, and system-affect cancer care delivery.
These findings are consistent with those reported in the systematic review and meta-analysis on cancer treatment delay and mortality. Delays in cancer treatment are a global issue across healthcare systems23. Even a 4-week delay in cancer treatment has been associated with increased mortality for surgical, systemic, and radiotherapy interventions across seven types of cancer24. The evidence also suggests a strong relationship between delays in pathology results or other diagnostic tests and a patient’s ability to receive timely diagnosis and treatment. This is likely due to the high volume of diagnostic requests, which often exceeds the capacity of the healthcare system. In addition, delays appear to originate from the primary care level, where physicians may face challenges in recognizing or suspecting cancer, leading to delays in referrals to secondary or tertiary care.
The structure of the Colombian healthcare system plays a significant role in the delays observed in cancer diagnosis and treatment. The system is a mixed model, consisting of both public and private sectors, with two primary regimes: the contributory regime for formal-sector workers and the subsidized regime for individuals with fewer resources. Despite efforts to ensure universal health coverage through the SGSSS, various challenges, including infrastructure limitations, regional disparities, and inefficiencies in service delivery, contribute to delays. These factors create barriers to timely diagnosis and treatment, as patients may face difficulties in accessing specialized care, particularly in rural or underserved areas. The fragmentation of the system, alongside its complex regulatory and referral processes, exacerbates these delays, further hindering prompt cancer care.
The findings from this study highlight several areas where policy changes could help mitigate delays in cancer diagnosis and treatment. One key policy recommendation is improving the infrastructure and resources in rural and underserved areas to ensure more timely access to specialized care. In addition, enhancing the efficiency of referral systems and diagnostic processes through digital health integration and better communication across healthcare levels could significantly reduce delays. It is also crucial to address systemic inefficiencies within the healthcare system by streamlining authorization processes and ensuring quicker turnaround times for pathology results. Public health policies should prioritize cancer awareness and early detection campaigns to reduce delays in problem recognition by patients. Furthermore, there should be continued investment in healthcare staff training to enhance decision-making, especially in primary care settings, where delays often begin. These interventions would likely lead to more timely diagnoses and treatments, ultimately improving patient outcomes.
Besides, our findings underscore the challenges in adhering to existing cancer care guidelines in Colombia, particularly regarding timely diagnosis and treatment initiation. According to the guidelines set by the Colombian Ministry of Health and Social Protection, cancer patients are expected to receive a diagnosis and begin treatment within specific timeframes to improve outcomes. However, the delays observed in this study, particularly those related to diagnostic results and the initiation of treatment, suggest that these guidelines are not always being followed. This discrepancy may be due to systemic issues such as limited healthcare resources, inefficient referral systems, and delays in obtaining pathology results. These barriers prevent the guidelines from being fully implemented in practice. Addressing these gaps through policy improvements and healthcare infrastructure enhancements is crucial to align the system more closely with the established guidelines.
Limitations
The analysis was based on retrospective data, which introduces inherent limitations. Moreover, the study was conducted in a single geographic area, which may limit the generalizability of the findings to other regions. To achieve greater representativeness of various cancer types and patient populations, especially those with rare cancers, it is recommended to replicate the study in larger and more diverse samples. Besides, the study did not examine the impact of patients’ socioeconomic status variables, such as income and education because they affect patients’ actions and access to healthcare. Finally, other variables that could account for clinical relationships, such as comorbidities and characteristics of patients, were not taken into consideration.
Conclusion
This study highlights the prevalence of advanced-stage cancer diagnoses, particularly among women and patients with solid tumors, such as skin, breast, and prostate cancers. A significant finding was the identification of delays in the diagnostic and treatment initiation process, with quality of care being the most substantial barrier. Notably, delays in pathology results and treatment initiation were more pronounced in hematologic cancers, with a higher proportion of delays observed in comparison to solid tumors. Furthermore, delays were more frequent among incident cases, especially in terms of obtaining pathology results and executing procedures. These delays were attributed to systemic inefficiencies, such as limitations in healthcare infrastructure and referral logistics. The evidence underscores the need for targeted policies to reduce these delays, particularly by improving the healthcare system’s infrastructure and ensuring timely access to care. These efforts are critical to improving patient outcomes and survival rates in Colombia.

