ORIGINAL ARTICLES
Bioequivalence study between two formulations of 25 mg lenalidomide capsules in healthy male subjects
Estudio de bioequivalencia entre dos formulaciones de lenalidomida de 25 mg en sujetos hombres sanos

-
Publication dates-
Oct-Dec , 2024
March 11, 2025
- Article in PDF
- Article in XML
- Automatic translation
- Send this article by e-mail
- Share this article +
Abstract
Background:
Lenalidomide, derived from thalidomide, is vital for treating multiple myeloma and other blood cancers due to its immunomodulatory and anti-angiogenic effects. Ensuring bioequivalence between generic and branded forms is crucial, especially for public health affordability.
Objective:
To evaluate pharmaceutical bioequivalence between two formulations of 25 mg lenalidomide capsules in healthy male subjects under fasting conditions.
Method:
Conducted as an open label, monocentric, randomized, 2 x 2 crossover trial with 32 participants in fasting state, analyte concentrations were measured using UPLC-MS/MS, and then the pharmacokinetic parameters were determined.
Results:
Statistical analysis has determined the geometric mean ratio (90% CI) of the test drug/reference drug for lenalidomide were 90.03 to 114.13% for Cmax and 88.21 to 101.02% for AUC0-t. Power of the test was 92.8% for Cmax and 100.0% for AUC0-t.
Conclusion:
Both formulations are bioequivalent and, therefore, they are interchangeable, according to the Brazilian criteria, since confidence intervals for Cmax and AUC0-t ratios were within 80 and 125%.
Keywords:
Lenalidomide, Bioequivalence, Capsules, Liquid chromatography-tandem mass spectrometry, Immune modulator, Antineoplastic
Introduction
Lenalidomide (IUPAC 3-(7-amino-3-oxo-1H-isoindol-2-yl)piperidine-2,6-dione), a thalidomide analog, is an immunomodulatory (IMiD) and antineoplastic agent used in multiple myeloma therapy1. Multiple myeloma is a malignant B-cell neoplasia characterized by the excess of monotypic plasma cells in the bone marrow. Established for the 1st time as agents with antiangiogenic properties, thalidomide, and the other IMiDs inhibit the production of interleukin, which is a growth factor for the proliferation of myeloma cells. In addition, they activate apoptotic pathways through cellular death by means of caspases 82.
-
1PubChem Compound Summary for CID 216326, Lenalidomide,
-
2Lenalidomide and thalidomide:mechanisms of action--similarities and differencesSemin Hematol, 2005
In 2005, the Food and Drug Administration (FDA) approved the marketing of 5 mg and 10 mg Revlimid® (Lenalidomide) capsules for the treatment of transfusion-depending anemia patients due to low-risk myelodysplastic syndrome (MDS) associated to 5q deletion abnormality with or without additional cytogenetic abnormalities and multiple myeloma in combination with dexamethasone3,4. The European Medicines Agency issued the authorization to market lenalidomide in 20075. In Brazil, ANVISA issued a public opinion for the approval of Revlimid in 2018 for the treatment of patients with relapsed/refractory multiple myeloma who had received at least one prior treatment; and for the treatment of patients with transfusion-depending anemia derived from low to intermediate-1 risk MDS associated to 5q deletion cytogenetic abnormality, with or without additional cytogenetic abnormalities6.
-
3Lenalidomide as a novel treatment of acute myeloid leukemiaExpert Opin Investig Drugs, 2013
-
4Drug Approval PackageRevlimid (Lenalidomide) Capsules. Celgene Corporation, 2005
-
5Revlimid Lenalidomide, 2007
-
6Agência Nacional de Vigilância SanitáriaREVLIMID, 2017
In 2017, ANVISA issued resolution RDC 191 (regarding the control of lenalidomide and any drugs containing it, among other provisions), later revoked in 2022 by a resolution with the same name (RDC 735/2022). Due to the risks associated to the teratogenic effects of lenalidomide-based drugs, the resolution stated, among other provisions, the design of a Risk Management Plan, including a pregnancy prevention program, which requires training of the physicians prescribing the drug by the register holder7.
-
7Agência Nacional de Vigilância Sanitária:resolução DA DIRETORIA COLEGIADA - RDC No 735, DE 13 DE JULHO DE 2022Dispõe Sobre o Controle da Substância Lenalidomida e de Medicamento Que a Contenha, e dáOutras Providências, 2022
In 2020, ANVISA issued RDC 393/2020, which included lenalidomide therapeutic indications for the treatment of multiple myeloma, in combination with bortezomib and dexamethasone, for patients with no prior treatment; for the treatment of follicular lymphoma or previously treated patients with marginal zone lymphoma, in combination with rituximab (anti-CD20 antibody), and relapsed/refractory mantle cell lymphoma8.
-
8Agência Nacional de Vigilância SanitáriaLenalidomida:autorizadas Novas Indicações Terapêuticas, 2020
As to the security profile, the authors report that lenalidomide is well tolerated and that most usual adverse events include hematologic toxicity with controllable neutropenia and thrombocytopenia9,10. According to the panel released by ANVISA through VigiMed, in the period between January 01, 2018, and September 09, 2022, 652 lenalidomide suspected adverse events were informed, out of which 16.10% corresponded to neutropenia and 4.45% to thrombocytopenia11.
-
9Lenalidomide in the treatment of multiple myeloma:a reviewJ Clin Pharm Ther, 2008
-
10A phase I trial of lenalidomide in patients with recurrent primary central nervous system tumorsClin Cancer Res, 2007
-
11Agência Nacional de Vigilância Sanitária:vigiMed - Eventos Adversos, 2022
The objective of this trial was to verify whether the rate and extent of absorption of the 25 mg lenalidomide immediate release capsule formulation manufactured by Eurofarma Laboratórios S.A. are equivalent to those of the reference product, REVLIMID® when administered in one single dose and under fasting conditions in adult healthy male subjects.
Methods
Study protocol and reporting
Bioequivalence studies are a type of study that follows specific rules dictated by the regulatory agencies in each country. Thus, study protocol drafting requirements follow the SPIRIT Statement12-14, where applicable. Data reporting is also carried out in the form of standardized reports by the agencies, but they contain all the information recommended for reporting according to the CONSORT Statement14,15. In Brazil, the following standards must be followed: (1) RE 894/2316, which defines the standardization for the preparation of bioequivalence study protocols, and (2) RE 895/2317, which defines the form of study reporting.
-
12SPIRIT 2013 statement:defining standard protocol items for clinical trialsAnn Intern Med, 2013
-
14An update to SPIRIT and CONSORT reporting guidelines to enhance transparency in randomized trialsNat Med, 2022
-
14An update to SPIRIT and CONSORT reporting guidelines to enhance transparency in randomized trialsNat Med, 2022
-
15CONSORT 2010 statement:updated guidelines for reporting parallel group randomised trialsBMJ, 2010
-
16Nacional de Vigilância Sanitária:resolução-RE No 894, DE 29 DE MAIO DE 2003:guia Para Elaboração de Protocolo de Estudo de Biodisponibilidade Relativa/Bioequivalênci, 2003
-
17Agência Nacional de Vigilância Sanitária:resolução-RE No 895, de 29 de Maio De 2003:ANEXO - Guia Para Elaboração de Relatório Técnico de Estudo de Biodisponibilidade Relativa/Bioequivalência, 2003
Study formulations
The test drug −25 mg lenalidomide immediate release capsule−, was manufactured by Eurofarma Laboratórios S/A. The reference product used in the study was Revlimid® (25 mg lenalidomide immediate release capsule), manufactured by Celgene Europe B.V. and registered in Brazil by Bristol-Myers Squibb Farmacêutica LTDA.
Study volunteers
Adult male healthy volunteers willing to participate in the study were selected based on the protocol eligibility criteria 90 days before the first study period. A sufficient number of eligible volunteers appeared in the research center facilities, and the 32 volunteers who fulfilled the protocol requirements were given information regarding the study, after having their inquiries clarified and having decided to willingly take part in the study, each subject signed the informed consent form, previously approved by the Avant Santé Research Center Research Committee (COFEPRIS 18 CI 19 019 021) along with the study protocol. Initially, 32 study subjects were selected and randomized, out of which only 28 completed all the study procedures due to exclusion and/or dropout reasons.
Study design
Single dose, randomized, open-label, two-treatment, two-sequence, two-period crossover bioequivalence study of 25 mg lenalidomide capsules manufactured by Eurofarma Laboratórios S.A. versus REVLIMID® (25 mg lenalidomide immediate release capsule) manufactured by Celgene Europe B.V. and registered in Brazil by Bristol-Myers Squibb Farmacêutica LTDA in adult male healthy volunteers under fasting conditions.
Drug administration
Study subjects were kept in fasting conditions for 10 h before the dose administration and at least 4 h afterward, on each period. The study was conducted under fasting conditions as required by ANVISA - Agência Nacional de Vigilância Sanitária18.
-
18Agência Nacional de Vigilância Sanitária:lista 1 - Forma de Administração (Formas Farmacêuticas de Liberação Imediata). RESOLUÇÃO - RE no 1170, de 19 de Abril de 2006, 2022
On each period of the study, a single dose (25 mg) of the test or the reference product was administered orally to the volunteers, in a seated position, with 200 mL of water at room temperature, under fasting conditions. The washout period was 7 days.
Blood sampling
A total number of 19 blood samples were collected from each volunteer in each period in tubes with K2EDTA. Blood samples (4 mL each) were collected at time points 0.00 h (before dose) and after administration at time points 0.25, 0.33, 0.50, 0.75, 1.00, 1.25, 1.50, 1.75, 2.00, 2.50, 3.00, 4.00, 6.00, 8.00, 10.00, 12.00, 16.00, and 24.00 h.
Biological samples processing
After collection, blood samples were processed in a refrigerated centrifuge at 3000 rpm for 10 min at 4 ± 2°C. The plasma obtained from the blood samples was transferred to two different cryogenic tubes (aliquot 1 and aliquot 2) previously identified and stored at a temperature below −50°C.
Lenalidomide quantification in plasma
METHOD VALIDATION
The validation of the bioanalytical method for quantification of lenalidomide in human plasma using Lenalidomide-d5 as internal standard and K2EDTA as anticoagulant through extraction in solid phase (Strata-X® 33 μm cartridge) and ultra-performance liquid chromatography-tandem mass spectrometry (LC-MS/MS) was performed in compliance with the acceptance criteria for selectivity, calibration curve, precision, accuracy, residual effect, matrix effect, and stability test in solution and the biological matrix (Table 1).
Tabla 1
Summary of the bioanalytical method
Summary of the bioanalytical method
| Analyte | Lenalidomide |
|---|---|
| Internal standard | Lenalidomide-d5 |
| Biological matrix | Human Plasma |
| Anticoagulant | EDTA |
| Linearity | 2.044 ng/mL-1015.506 ng/mL |
| Curve equation | y = a + bx [1/x] |
| Lower quantification limit | 2.044 ng/mL |
| Low quality control | 5.148 ng/mL |
| Medium quality control | 411.867 ng/mL |
| High quality control | 792.052 ng/mL |
| Post-processing stability time | 2 days 8 h 38 min |
| Freeze/thaw cycles | 4 cycles |
| Short-term stability time | 6 h 18 min |
| Long-term stability time | 106 days |
Chromatographic conditions adopted for the validation and quantification of the study subject samples included the use of a Luna omega 1.6 μm PS C18 50 × 2.1 mm chromatographic column, at 35 ± 2°C. Samples were kept at 5 ± 4°C. Mobile phase A used was Formic Acid 0.1% and mobile phase B was LC-MS grade Acetonitrile in an 87:13 v/v proportion. The injection volume was 3.0 μL and retention times were 1.07 ± 0.3 min for the analyte and 1.05 ± 0.3 for the internal standard, the running time being 2.10 min.
The method proved linear between concentrations of 2.044 ng/mL to 1015.506 ng/mL according to equation y = a + bx [1/x], where "y" is the response, "x" is the analyte concentration and "1/x" is the selected weight.
The lower limit of quantification (LLQ) established for the method was 2.044 ng/mL and validated quality control samples were 5.148 ng/mL, 411.867 ng/mL, and 792.052 ng/mL.
STABILITY
Stability analysis was carried out in plasma in concentrations of 5.148 ng/mL and 792.052 ng/mL and they complied with the acceptance criteria when the samples were subjected to 6 h and 18 min at room temperature (approximately 25°C) (short-term stability), for 2 days 8 h and 38 min in auto-injector (5 ± 4°C) after sample extraction completion (post-processing stability) 4 freeze-and-thaw cycles and 106 long-term days.
STANDARD SOLUTIONS
Reference standards: lenalidomide (TRC/Canada) was used as an analyte and Lenalidomide-d5 (TRC/Canada) was used as an internal standard for the preparation of the primary standard solutions in methanol HPLC grade. Working solutions were prepared using milli-Q water: methanol (20:80; v/v) as eluent. All solutions were stored at a temperature between 2 and 8°C.
Compounds quantification in biological samples
Compounds were extracted from human plasma samples and quantified through LC-MS/MS using the Xevo TQ-S/Acquity UPLC I-Class (Waters) spectrometer, equipped with positive electrospray (ESP+) ionization source, and the analyte and internal standard were detected using multiple reaction monitoring with m/z transitions 260.21 > 149.11 and 265.23 > 151.13, respectively.
Software used
Software Masslynx version 4.1 was used for calculating sample concentrations in the analytic phase.
Software Phoenix WinNonlin version 8.3 and Statistical Analysis System (SAS®) version 9.4 were used to perform the statistical analysis.
Results
Study population
The study began with 32 volunteers and ended with 28 healthy male volunteers between 18 and 42 years of age, who complied with the inclusion and exclusion criteria set forth in the protocol.
Pharmacokinetics and statistical analysis
Pharmacokinetic parameters Cmax and AUC0-t were established using software Phoenix WinNonlin version 8.3 and Sistema de Análise Estatística (SAS®) version 9.4.
Pharmacokinetic parameters are shown in table 2.
Tabla 2
Pharmacokinetic parameters (n = 28)
Pharmacokinetic parameters (n = 28)
| Ratio (test/reference) | Geometric mean (%) | CI (90%) | Test power (%) | p (sequence) |
|---|---|---|---|---|
| Cmax (ng/mL) | 101.4 | 90.03-114.13 | 92.8 | 0.5299 |
| AUC0-t (ng.h.mL-1) | 94.4 | 88.21-101.02 | 100.0 | 0.1203 |
The maximum concentration of Cmax obtained for the reference product Revlimid® was 439.761 ng/mL in 1.5 h. For the test product, lenalidomide, a Cmax of 477.742 ng/mL occurred at 1.1 h. Figure 1 shows intermediate concentrations of lenalidomide for the 28 study subjects along collection times.
Thumbnail
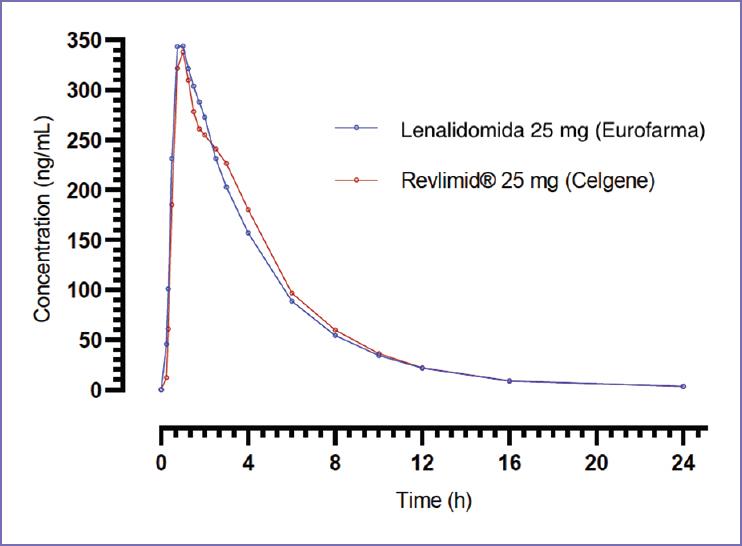
Figure 1
Lenalidomide intermediate concentrations along time for each formulation.
Lenalidomide intermediate concentrations along time for each formulation.
Tolerability/safety analysis
Eight adverse events were reported during the study: 3 headaches, 1 erythema, 1 rash, 1 hypertriglyceridemia, 1 rectal hemorrhage, and 1 normochromic normocytic anemia. No serious adverse events were reported; 6 events were classified as mild and 2 as moderate.
As to the relation with the study drug, 1 adverse event was classified as possibly related, 2 as probably related, and 5 as unlikely to be related to the study medication.
Discussion
The study was properly planned and conducted, obtaining pharmacokinetic parameters Cmax and AUC0-t which confidence interval values (90%) are within the acceptable limit for the ratio between the geometric means of the test and reference products (80−125%), according to the national legislation, ANVISA resolution RE no 1170/200619.
-
19Agência Nacional de Vigilância Sanitária:resolução - RE 1.170, de 19 De Abril De 2006Guia Para Provas De Biodisponibilidade Relativa/Bioequivalência De Medicamentos, 2006
The planned number of 32 healthy male subjects is consistent with studies published by other authors20,21. The population selected for the study was male gender only, as recommended by the FDA guidelines22 and consistent with resolution ANVISA RDC 735/20227.
-
20Single-dose comparative pharmacokinetics of two formulations of lenalidomide 25 mg in healthy subjects:a randomized crossover studyAdv Ther, 2018
-
21Bioequivalence study of single-dose lenalidomide capsule vs. Revlimid® capsule in healthy Chinese malesCancer Chemother Pharmacol, 2018
-
22Draft Guidance on Lenalidomide, 2013
-
7Agência Nacional de Vigilância Sanitária:resolução DA DIRETORIA COLEGIADA - RDC No 735, DE 13 DE JULHO DE 2022Dispõe Sobre o Controle da Substância Lenalidomida e de Medicamento Que a Contenha, e dáOutras Providências, 2022
Both formulations were well tolerated during the study and no serious adverse events were reported. Headache was the most frequent adverse event, contrary to the reports of other authors and the ANVISA panel, who stated neutropenia and thrombocytopenia as the most frequent adverse events9,11,23.
-
9Lenalidomide in the treatment of multiple myeloma:a reviewJ Clin Pharm Ther, 2008
-
11Agência Nacional de Vigilância Sanitária:vigiMed - Eventos Adversos, 2022
-
23Lenalidomide plus dexamethasone versus thalidomide plus dexamethasone in newly diagnosed multiple myeloma:a comparative analysis of 411 patientsBlood, 2010
The 7-day washout period seemed adequate, as all base collection samples of the volunteers of the second period had a concentration below the LLQ.
As in other published works, the analytical technique selected for the study of lenalidomide quantification of in human plasma samples was LC-MS/MS24-26.
-
24Development and validation of Lenalidomide in human plasma by LC-MS/MSSaudi J Biol Sci, 2019
-
26Development and validation of LC-MS/MS method for the quantitation of lenalidomide in human plasma using Box-Behnken experimental designAnalyst, 2013
Lenalidomide was quantified in its unaltered form, as required by the national legislation27.
-
27Agência Nacional de Vigilância Sanitária:lista 2 - Analito Para Estabelecimento da Biodisponibilidade Relativa/BioequivalênciaResolução - RE no 1170, de 19 de abril de 2006, 2022
Both reference and test drugs showed a maximum plasma concentration Cmax of 439.761 ng/mL and 477.742 ng/mL, respectively, consistent with those found in the literature20,21.
-
20Single-dose comparative pharmacokinetics of two formulations of lenalidomide 25 mg in healthy subjects:a randomized crossover studyAdv Ther, 2018
-
21Bioequivalence study of single-dose lenalidomide capsule vs. Revlimid® capsule in healthy Chinese malesCancer Chemother Pharmacol, 2018
Conclusion
The results show test and reference formulations are considered bioequivalent regarding the absorption rate and extent, as the criteria required by the Brazilian regulatory authority have been complied with (CI 90% between 80 and 125%). Consequently, the test formulation, i.e. lenalidomide manufactured by Eurofarma Laboratórios S/A and the reference product Revlimid®, both in 25 mg capsules, are bioequivalent and therefore, interchangeable.
Authors contributions
C. Sverdloff participated in the study design and supervision. V. Marcondes Rezende performed the data curation and wrote the manuscript and reviews. L. de Cassia Val and L. Nerath Bonanato participated in the Project Administration and supervision. M.E. Cedano Limón conducted the clinical investigation. S. Kakarla performed bioanalytical method validation and supervision of sample analysis. M.H. Badii performed the statistical analysis. M. Pendela performed general site supervision. N.C. Lemus Castro wrote the clinical protocol, supervised clinical investigation, and was the principal investigator. All authors contributed with data and revision and approved the final manuscript.
References
-
1PubChem Compound Summary for CID 216326, Lenalidomide. Available from:https://pubchem.ncbi.nlm.nih.gov/compound/lenalidomide [Last accessed on 2022 Oct 27]. Links
-
2Anderson KC. Lenalidomide and thalidomide:mechanisms of action--similarities and differences. Semin Hematol. 2005;42:S3-8. Links
-
3Chen Y, Borthakur G. Lenalidomide as a novel treatment of acute myeloid leukemia. Expert Opin Investig Drugs. 2013;22:389-97. Links
-
4FDA-Food and Drug Administration. Drug Approval Package. Revlimid (Lenalidomide) Capsules. Celgene Corporation;2005. Available from:https://www.accessdata.fda.gov/drugsatfda_docs/nda/2005/021880s000_RevlimidTOC.cfm [Last accessed on 2005 Dec 27]. Links
-
5EMA. Revlimid Lenalidomide;2007. Available from:https://www.ema.europa.eu/en/medicines/human/EPAR/revlimid#authorisation-details-section Links
-
6ANVISA. Agência Nacional de Vigilância Sanitária. REVLIMID. Brazil:ANVISA;2017. Available from:https://consultas.anvisa.gov.br/#/medicamentos/25351757160201560/?substancia=25181%20 Links
-
7ANVISA. Agência Nacional de Vigilância Sanitária:resolução DA DIRETORIA COLEGIADA - RDC No 735, DE 13 DE JULHO DE 2022. Dispõe Sobre o Controle da Substância Lenalidomida e de Medicamento Que a Contenha, e dáOutras Providências. Brazil:ANVISA;2022. Links
-
8ANVISA. Agência Nacional de Vigilância Sanitária. Lenalidomida:autorizadas Novas Indicações Terapêuticas. Brazil:ANVISA;2020. Available from:http://antigo.anvisa.gov.br/resultado-de-busca?p_p_id=101&p_p_lifecycle=0&p_p_state=maximized&p_p_mode=view&p_p_col_id=column-1&p_p_col_count=1&_101_struts_action=%2fasset_publisher%2fview_content&_101_assetentryid=5893220&_101_type=content&_101_groupid=219201&_101_urltitle=lenalidomida-autorizadas-novas-indicacoes-terapeutic-1&inheritredirect=true Links
-
9Armoiry X, Aulagner G, Facon T. Lenalidomide in the treatment of multiple myeloma:a review. J Clin Pharm Ther. 2008;33:219-26. Links
-
10Fine HA, Kim L, Albert PS, Duic JP, Ma H, Zhang W, et al. A phase I trial of lenalidomide in patients with recurrent primary central nervous system tumors. Clin Cancer Res. 2007;13:7101-6. Links
-
11ANVISA. Agência Nacional de Vigilância Sanitária:vigiMed - Eventos Adversos. Brazil:ANVISA;2022. Available from:https://www.gov.br/anvisa/pt-br/acessoainformacao/dadosabertos/informacoes-analiticas/notificacoes-de-farmacovigilancia Links
-
12Chan AW, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, Krleža-JerićK, et al. SPIRIT 2013 statement:defining standard protocol items for clinical trials. Ann Intern Med. 2013;158:200-7. Links
-
13Chan AW, Tetzlaff JM, Gøtzsche PC, Altman DG, Mann H, Berlin JA, et al. SPIRIT 2013 explanation and elaboration:guidance for protocols of clinical trials. BMJ. 2013;346:e7586. Links
-
14Hopewell S, Boutron I, Chan AW, Collins GS, de Beyer JA, Hróbjartsson A, et al. An update to SPIRIT and CONSORT reporting guidelines to enhance transparency in randomized trials. Nat Med. 2022;28:1740-3. Links
-
15Schulz KF, Altman DG, Moher D. CONSORT 2010 statement:updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. Links
-
16ANVISA. Nacional de Vigilância Sanitária:resolução-RE No 894, DE 29 DE MAIO DE 2003:guia Para Elaboração de Protocolo de Estudo de Biodisponibilidade Relativa/Bioequivalênci. Brazil:ANVISA;2003. Links
-
17ANVISA. Agência Nacional de Vigilância Sanitária:resolução-RE No 895, de 29 de Maio De 2003:ANEXO - Guia Para Elaboração de Relatório Técnico de Estudo de Biodisponibilidade Relativa/Bioequivalência. Brazil:ANVISA;2003. Links
-
18ANVISA. Agência Nacional de Vigilância Sanitária:lista 1 - Forma de Administração (Formas Farmacêuticas de Liberação Imediata). RESOLUÇÃO - RE no 1170, de 19 de Abril de 2006. Brazil:ANVISA;2022. Links
-
19ANVISA. Agência Nacional de Vigilância Sanitária:resolução - RE 1.170, de 19 De Abril De 2006. Guia Para Provas De Biodisponibilidade Relativa/Bioequivalência De Medicamentos. Brazil:ANVISA;2006. Links
-
20Lee S, Hwang JG, Park SY, Lim HJ, Lee SW, Seo MH, et al. Single-dose comparative pharmacokinetics of two formulations of lenalidomide 25 mg in healthy subjects:a randomized crossover study. Adv Ther. 2018;35:210-7. Links
-
21Wang J, Qi L, Wang Z, Chen G, Liu C, Liu Y, et al. Bioequivalence study of single-dose lenalidomide capsule vs. Revlimid® capsule in healthy Chinese males. Cancer Chemother Pharmacol. 2018;82:159-64. Links
-
22FDA-Food and Drug Administration. Draft Guidance on Lenalidomide;2013 Available from:https://www.accessdata.fda.gov/drugsatfda_docs/psg/lenalidomide_draft_oral%20cap_rld%2021880_rc11-13.pdf Links
-
23Gay F, Hayman SR, Lacy MQ, Buadi F, Gertz MA, Kumar S, et al. Lenalidomide plus dexamethasone versus thalidomide plus dexamethasone in newly diagnosed multiple myeloma:a comparative analysis of 411 patients. Blood. 2010;115:1343-50. Links
-
24Ranganathan P, Gunasekaran V, Singhvi I, Ansari MJ. Development and validation of Lenalidomide in human plasma by LC-MS/MS. Saudi J Biol Sci. 2019;26:1843-7. Links
-
25Iqbal M, Wani TA, Khalil NY, Darwish IA. Development and validation of ultra-performance liquid chromatographic method with tandem mass spectrometry for determination of lenalidomide in rabbit and human plasma. Chem Cent J. 2013;7:7. Links
-
26Hasnain MS, Rao S, Singh MK, Vig N, Gupta A, Ansari A, et al. Development and validation of LC-MS/MS method for the quantitation of lenalidomide in human plasma using Box-Behnken experimental design. Analyst. 2013;138:1581-8. Links
-
27ANVISA. Agência Nacional de Vigilância Sanitária:lista 2 - Analito Para Estabelecimento da Biodisponibilidade Relativa/Bioequivalência. Resolução - RE no 1170, de 19 de abril de 2006. Brazil:ANVISA;2022. Available from:https://www.gov.br/anvisa/pt-br/setorregulado/regularizacao/medicamentos/equivalencia-terapeutica/bioequivalencia/listas [Last accessed on 2022 Mar 31]. Links