











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Myxomas are the most common primary heart tumor1. It is estimated that more than 75% of myxomas originate in the left atrium, either in the mitral annulus or at the edge of the oval fossa of the interauricular septum; 20% arise from the right atrium, whereas 5% come from both the atrium and ventricle2,3. Atrial myxomas are associated with a triad of complications, including obstruction, embolisms, and constitutional symptoms (such as fever and weight loss)2,4.
Due to the high systolic pressure and its location, left atrial myxomas were highly associated with an increased risk of systemic embolization, particularly in the central nervous system, retinal arteries, as well as viscera, spleen, kidneys, adrenal glands, abdominal aorta, iliac and femoropopliteal arteries5. Therefore, patients may have a variety of presentations, such as transient ischemic attack, hemiplegia, vision loss, chest pain, and dyspnea. The defects in neurological embolizations are probably the most serious complications of embolizations associated with left atrial myxomas6.
Clinical case
A 30-year-old woman with no personal pathological history, who 5 h before admission presented a clinical picture characterized by loss of alertness of 5 min accompanied by dysarthria, right hemiparesis on cardiovascular examination presented a protodiastolic murmur "tumor plop" on the left parasternal border.
The computed tomography (CT) image of the simple skull shows that; ischemic cerebral infarction in the subacute phase located in the left hemisphere with involvement of the temporal lobe, inferior frontal gyrus, deep area of the semioval center, lenticular nucleus, dorsolateral portion of the head of the caudate nucleus, anterior arm and knee of the internal capsule, rostral area of the thalamus and short gyrus of the insula, exerts a slight effect on volume and obliterates the corresponding gyrus (Fig. 1).

Figure 1 Ischemic cerebral infarction in the subacute phase located in the left hemisphere with temporal lobe involvement.
Transthoracic echocardiogram is observed in the left atrium with diameters of 37 × 37 × 49 mm, left atrium volume 38 mL/m2, multilobed and hypomobile tumor with the consistency of different echogenicities and cystic areas, of gelatinous consistency, adhered to the interatrial septum with a base of 25 × 27 mm very proximal at the anterior level of the septum and through it near the aortic valve. The size of the tumor is 40 × 20 mm and the larger lobe is 21 × 20 mm (Fig. 2), slides through the anterior leaflet of the mitral without being attached to it and interferes with the opening, causing functional stenosis of mild degree area by 3D planimetry 2.3 cm2, mean gradient 4 mm Hg, maximum velocity of 1.2 m/s, the insufficiency is mild with a 2 mm contract vein (Fig. 3).

Figure 2 Apical axis four chambers are observed in the left atrium tumor is 40 × 20 mm and the larger lobe is 21 × 20 mm.
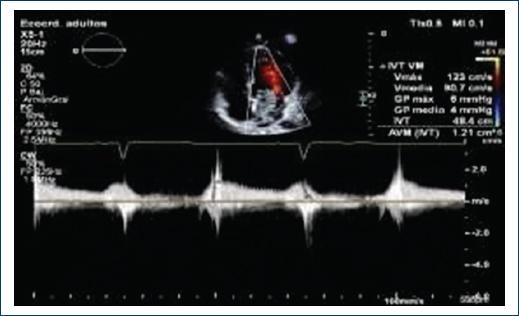
Figure 3 Continuous Doppler to the mitral valve presents functional stenosis of mild grade medium gradient 4 mmHG Maximum velocity of 1.2 m/s, insufficiency is mild with contracta vein of 2 mm.
A right auriculotomy was performed, an interauricular septum was opened, finding a left atrial tumor with a pedicle attached to the middle third of the interatrial septum, so the septum was resected, obtaining a mucoid-like tumor exit of approximately 5 × 4 cm. (Fig. 4) A biopsy (2408739) is performed, which describes; a fragment of tissue of irregular shape and surface, measuring 4.3 × 3.8 × 1.2 cm., white with translucent areas and areas of hemorrhage, of soft consistency, serial cuts are made, observing solid and heterogeneous in which white areas are intermingled with dark brown. The presence of atrial myxoma is concluded.

Discussion
Cardiac myxoma is a neoplasm of uncertain histogenesis that occurs only on the endocardial surface, most often in the atrial location. Histological diagnosis is based on the finding of typical cells in a matrix rich in mucopolysaccharides. Cardiac myxoma cells are histologically and histogenetically different from the spindle cells of soft-tissue myxomas. It has been postulated that the cells that give rise to this tumor are the so-called "subendothelial reserve cells," which are totipotent and have the capacity to form vascular structures7 and express endothelial and neural markers. The existence of a population of aneuploid cells in a tumor is generally considered to be evidence that the lesion is neoplastic8. The presence of aneuploidy, as well as the finding of chromosomal abnormalities in cases of myxomas, supports the neoplastic origin of this tumor.
The size and location of the myxomas determine the clinical manifestations of obstruction to intracardiac blood flow, with the simulation of valvulopathies of various types, especially mitral narrowing. The size of the tumor and also the different positions of the body can determine the severity of the obstruction and symptoms vary from dyspnea due to heart failure or syncope, to sudden death due to complete obstruction.
Embolization is a common manifestation, which is associated with small tumors (< 4.5 cm2). Most emboli migrate to the central nervous system and cause strokes; however, they can migrate to any part of the arterial system and produce a variety of signs and symptoms. There are reported cases of embolism to the lower limbs or to the coronary limbs, among others. In some cases, cardiac and extracardiac manifestations may occur, including acute myocardial infarction, cerebrovascular events, pulmonary embolism, and fever of unknown origin; however, a classic triad has been established, consisting of obstructive and constitutional symptoms, as well as embolic events5.
Cerebrovascular events associated with cardiac myxomas have been observed in up to 22% of cases, with a predominance in females1. The ideal imaging study is brain nuclear magnetic resonance imaging given the high rate of false negatives that CT of the skull yields. They have a low mortality rate and the ideal time for tumor resection is still unclear; despite this, it has been recommended that it be postponed until 4 weeks after the stroke event to reduce the risk of perioperative death9.
Diagnosis is challenging; it is made through transthoracic, transesophageal echocardiogram, and cardiac magnetic resonance imaging, although it can sometimes be identified by cardiac CT. The echocardiogram can easily visualize the mass and describe the location, shape, size, number, and morphological characteristics; in addition, it assesses the hemodynamic consequences of the tumor10. On tomography, myxomas may be well-defined and appear lobed, smooth, mobile, round, or oval, with a narrow pedicle; they are generally heterogeneous and have patchy foci of calcification and enhancement11.
As for treatment, expertise is required and will always be surgical. It is important to determine the origin and malignancy of these tumors in the pre-operative period. A well-known example is renal carcinoma with expansion to the right atrium, which can be mistaken for a primary tumor before being taken to surgery. In addition, not all of them are real tumors because there are "pseudotumors," thrombi, cysts, and tuberculomas11. Post-operative echocardiographic follow-up is recommended since the tumor recurrence rate after successful resection reaches up to 4-7%12.
Conclusion
Atrial myxomas are the most common primary cardiac tumors, with embolization being one of their most frequent forms of presentation, most emboli migrate to the central nervous system, which is why atrial myxoma should be considered one of the main causes of cerebrovascular events in young patients without comorbidities.

