











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The electroencephalogram (EEG) is the simultaneous recording in several channels at the extra-cerebral level, of cortico-subcortical electrical activity, spontaneous or provoked, by means of the placement of superficial electrodes1.
The EEG is one of the most widely used electro-physiological auxiliary tools in neurological, psychiatric, and other speciality diagnosis such as sleep medicine or somnology. This is because it is a non-invasive method auxiliary in clinical diagnosis that can be carried out on an outpatient basis (under some conditions), it is easy to perform; It can be requested urgently and in intensive care units or operating theatres. The EEG helps in the clinical diagnosis, classification, and prognosis of the patient. The presentation of the results is agile, can be sent by telemetry, and is applicable to all ages. For these reasons, in this review, we will update the state of knowledge about the EEG technique, its normal characteristics, and the pathologies in which it is indicated in the evaluation of sleep and its diseases1.
Neurophysiological basis of EEG
The origin of the cortical electrical activity observed in the EEG comes from the post-synaptic potentials (PSP)2. PSP are temporal variations in the resting membrane potential at synapse. PSP can be excitatory and inhibitory. PSP have the property of being able to be recorded in fields far from their neural generators and can be conducted by volume to the skin of the skull. When various neural networks synchronize to oscillate together, different oscillatory frequencies or brain rhythms are produced. For example, the temporal functional coupling of certain neural networks in the range of 8-13 cycles/s (Hz) can determine the electro-physiological oscillation in the alpha frequency in the temporo-parieto-occipital regions3.
Electroencephalographic rhythms
The recorded electrical activity is characterized by a series of more or less regular temporal oscillations according to the functional state (FS). The well-characterized FS for EEG in humans are: (1) wakefulness-eyes closed-physical and mental rest; (2) wakefulness-eyes open; (3) sleep in the initial or transitional sleep phase or N1; (4) sleep in light sleep or N2 phase; (5) sleep in deep sleep or slow wave or N3; and (6) sleeping in the rapid eye movement (REM) phase.
Brain rhythms are classified according to the frequency they present: oscillations between 0.1 and 3.9 Hz are known as delta rhythms; those between 4 and 7.9 Hz are called theta rhythms; between 8 and 13 Hz, are called alpha and between 14 and 35 Hz, are called beta rhythms4. There are other EEG rhythms, the best known of which are sigma rhythms, which are present during the N2 phase of sleep. Sigma rhythms have a frequency between 12 and 16 Hz, with a duration of between 0.5 and 1.5 s, in central regions and are of fusiform morphology, which is why they are also called: Sleep spindles5.
In the phase of wakefulness-eyes closed-physical and mental rest, the EEG is characterized by the presence of alpha rhythms in the temporo-parieto-occipital areas and frontal beta rhythms forming an anteroposterior amplitude gradient. In the wake-eyes open phase, the EEG shows generalized beta rhythms due to a cortical desynchronization phenomenon known as alpha rhythm blocking caused by eye-opening.
EEG rhythms in the initial sleep or N1 phase are characterized by a loss of alpha-based activity and the appearance of diffuse delta and theta rhythms of low to medium amplitude. In preschoolers, schoolchildren, and adolescents, slow-wave outbreaks may appear in the theta range of greater fronto-parietal amplitude called: hypnogenic hypersynchrony. In the N2 phase, sleep spindles or sigma rhythms are present in frontoparietal areas, as well as acute waves of the vertex that when grouped together are called K complexes. In the N3 phase, irregular or monorhythmic delta activity appears, in a generalized way, of high voltage. Finally, in the REM phase, the activity presents as generalized low-voltage rhythms, of higher frequency and lower amplitude, with a predominance in the range in diffuse theta and beta frequencies, and the typical sawtooth waves6.
Summary of the neurophysiological mechanisms of sleep
There are several neural networks that promote the various FS that occur during wakefulness and sleep. In the vigila, the ascending activating reticular formation and the posterior hypothalamic nucleus influence the non-specific thalamic nuclei to increase the tone of the cerebral cortex. To mantain wakefulnes, the hypothalamus secretes hypocretins, on the other hand, in the brainstem, the raphe nucleus releases serotonin while the locus ceruleus secretes noradrenaline. For its part, Meynert’s nucleus releases acetylcholine and the amygdala and suprachiasmatic nucleus dopamine7, there is much evidence that all these neurotransmitters are promoters of wakefulness.
In non-REM sleep, hypocretin secretion is inhibited by GABAergic and galinergic discharges from the ventro-lateral pre-optic nucleus that decreases the activity of wakefulness-promoting networks. The activity of the thalamic reticular nuclei generates sleep spindles by cortical desaferentation, inhibiting non-specific afferent sensory fibers. On the other hand, the nucleus of the solitary fasciculus is activated, influencing the activity of the midbrain, hypothalamus, thalamus, and limbic system, producing a progressive hyperpolarization of the thalamic reticular nuclei until the sleep spindles disappear and the dorsal thalamic nuclei are activated, projecting to the cortex, producing the delta activity characteristic of deep sleep (Fig. 1)8.
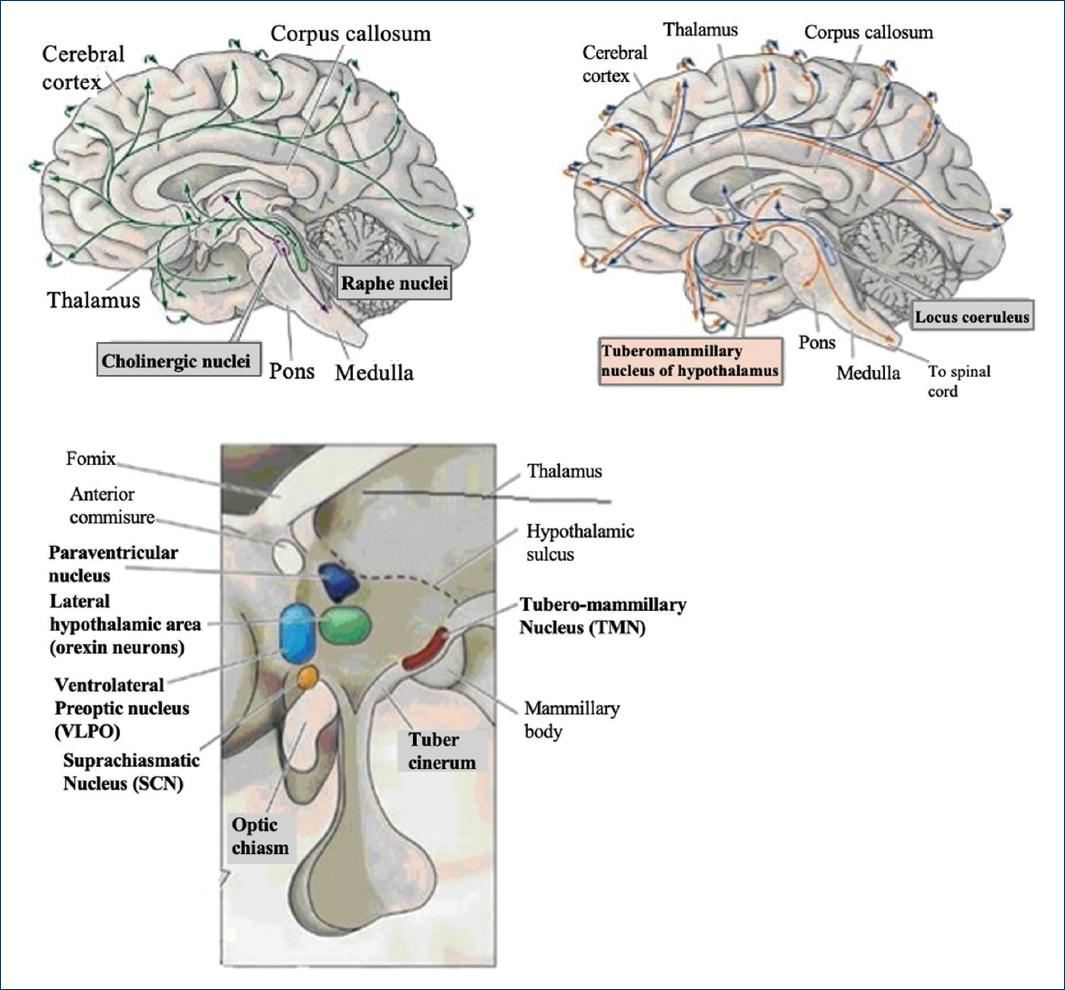
Figure 1 Brain structures and their sleep-generating circuits. Upper left panel, raphe core, and its cholinergic pathways. Upper right panel, locus coeruleus, and nordrenéric pathways. Bottom panel, hypothalamic nuclei involved in the generation of sleep. Explanation in the text (inspired by Purves et al. 2012).
The neural networks that promote REM sleep originate mainly in the pontine oralis reticular nucleus which, through activating ascending fibers, originate REM discharges, aided by the locus coeruleus (noradrenergic) and the raphe nucleus (serotonergic), which increase the activity of the geniculate nucleus and the cerebral cortex9. The behavior of these cycles is circadian coordinated daily by the suprachiasmatic nucleus in the hypothalamus, which clocks the duration of each sleep-wake cycle (Fig. 1).
On the other hand, there is a neuroendocrine system that promotes sleep. This system is especially active in the early stages of development through the secretion of melatonin, a hormone that is produced mainly by the pineal gland and to a lesser extent by the retina. Its secretion is stimulated by darkness and inhibited by ambient lighting. It acts by inhibiting the neural networks that promote wakefulness in a circadian way10.
The study of clinical EEG in sleep disorders
A clinical EEG for the study of sleep disorders (SD) includes the recording of the following conditions: (1) wakefulness-eyes closed-physical and mental rest; (2) wakefulness-eyes open; (3) intermittent light stimulation; (4) hyperventilation; and (5) asleep. The duration of the study ranges from 30 min to 8-12 h. The condition of wakefulness in closed eyes at physical and mental rest causes the appearance of alpha temporo-parieto-occipital rhythms and faster activity and lower frontal voltage or base activity. Wakefulness: eyes open: blocks the alpha rhythms and desynchronizes cortical activity, causing the appearance of generalized beta rhythms1,3.
Intermittent light stimulation consists of flashes of intermittent light at different frequencies under conditions 1, 2, or 5. The light stimulation frequencies can follow the following order: 1, 2, 4, 6, 8, 10, 12, 14, 16, 18, 20, 40, 60, 30, 10, 5 and 1 flash/s. The physiological response is a drag or synchronization to the stimulation frequencies when they are within the EEG rhythms or the generalized desynchronization of the base rhythms. The pathological response consists of the presentation of focal or generalized epileptiform graphoelements as in absence epilepsy (ELF), or reflex or photosensitive epilepsies11.
Hyperventilation is achieved by asking the subject to breathe deeply and rapidly, at a frequency of 1 Hz for 2-3 min; the maneuver produces a slowing of the baseline activity or the appearance of generalized slow waves in the theta-delta range. In pathological conditions, abnormal epileptiform graphoelements will appear. The patient should be warned that this exercise may cause dizziness, paresthesias, or a mild transient headache12.
In the interpretation of a clinical EEG study, the following parameters will be taken into account: (1) temporal organization, how cortical electrical activity is distributed over time; (2) spectral organization, what are the electroencephalographic rhythms present in the recording; (3) topographic organization, how electroencephalographic rhythms are geographically distributed in the skin of the skull; (4) inter-hemispheric symmetry, since there should be no inter-hemispheric amplitude differences > 25% between electrodes of homologous areas; (5) synchrony, since there should also be no inter-hemispheric differences > 50 ms between graph-elements of homologous areas; (6) presence of normal patterns, for example,: hypnogenic hypersynchrony, lambda waves, acute transitions, etc.; (7) presence of abnormal patterns, for example: spikes, sharp waves, slow spikes-waves, spikes-slow waves, etc.
Abnormal items in the EEG log
There are graphoelements in the EEG that are related to pathological conditions. We can highlight: (1) Spikes: elements with an acute cusp, of variable amplitude that usually stand out above the base amplitude, with a duration < 70 ms; when 2 or more are grouped together, they are known as polispikes. (2) Acute waves, elements with a punctiform cusp that last 70-200 ms. (3) Slow spike-wave complexes. Association of a tip with a sine wave with a rounded edge > 200 ms. (4) Polispikes-slow wave: association of 2 or more points with a slow wave. (5) Acute wave-slow wave. Association between a high and a slow wave. (6) Slow waves: presentation of rounded elements > 200 ms that stand out from the base activity, sometimes they are usually grouped into trains or discharges of 2 or more elements. The identification of these elements in the EEG tracing suggests the presence of abnormal activity of neural networks in the cerebral cortex associated with pathologies such as epilepsy.
EEG and polysomnography (PSG) in the study of SD
PSG is the simultaneous recording of the electrical activity of the EEG and various extra-cerebral variables during sleep that help determine the succession of the various phases of sleep (the architecture of the sleep that forms the hypnogram) and other elements that help in the diagnosis of SD. The EEG is usually reduced to the recording of only 2-4 channels of central and occipital regions, in addition, eye movements are recorded to identify non-REM sleep and REM, surface electromyography of the axial musculature (lower lip depressor muscle) and appendicular (tibialis anterior muscles) to determine the movements that accompany wakefulness, sleep apnea, periodic limb movements and bruxism, movements in parasomnias and epileptic seizures, atony in cataplexy and sleep paralysis; nasal airflow, plethysmography of thoracic movements, oxygen saturometry and electrocardiography are also recorded to determine respiratory behavior, its effect on blood chemistry and repercussions on heart rhythm. PSG is one of the most important objective and quantitative diagnostic aids in the study of SD13.
Methods
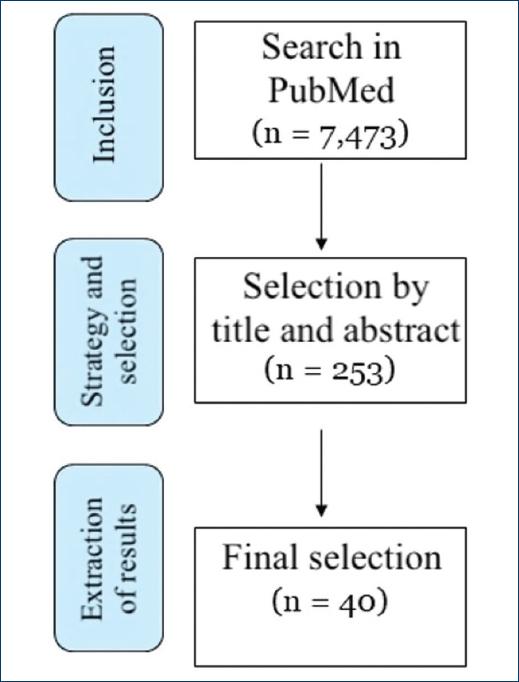
A review was carried out according to the PRISMA criteria14. The inclusion criteria of the articles were on original EEG articles in some phase of sleep, the exclusion criterion was experimental articles carried out in sleep in animals. The source of information was the basis of the U.S. National Library of Medicine, through PubMed. The search strategy was to use the terms MeSH (medical subjects headings) “electroencephalography” AND “sleep” IN “humans”, 7,473 articles were found. The selection process of articles was based on the title and abstract due to their probable usefulness for the purposes of the review (n = 253 articles). The data extraction process was carried out by downloading and reading the final pertinent articles by each of the researchers, leaving 40 articles (Fig. 2).
Results
Indications of an EEG and PSG study in SD
INSOMNIA
Although EEG is not indicated for the diagnosis and monitoring of the treatment of these alterations, some research studies have detected a reduction in beta, gamma, and anteroposterior synchronization activity in subjects with acute sleep deprivation15. PSG is also not very useful in the diagnosis and management of insomnia since it will only reveal an increase in the time of sleep onset and will only be indicated based on the associated comorbidity16.
SLEEP-DISORDERED BREATHING
The EEG is also not indicated for the diagnosis and monitoring of the treatment of these alterations. However, some research studies carried out in patients with obstructive sleep apnea have detected a reduction in beta activity in wakefulness, a reduction in sigma, beta, and gamma activity during non-REM sleep, and an increase in delta activity in REM sleep17. However, the PSG is the cornerstone in the identification, diagnosis, classification, and therapeutic monitoring of primary snoring and apnea, both central, obstructive, and mixed.18 However, of all the sensors used for this study, respiratory variables such as nasal airflow, thoracic respiratory movements, and oxygen saturation are the ones that provide the most information to the SD clinic18.
CENTRAL ALTERATIONS WITH HYPERSOMNIA
EEG is also not indicated for the diagnosis and monitoring of the treatment of these alterations; although in narcolepsy a lower density of delta potency has been observed during light sleep19. In PSG, the study of multiple sleep latencies has been developed, in which the patient is given four brief opportunities to sleep (30 min each) in the morning, measuring the latency to REM sleep. If a latency shortened to active sleep is recorded, then it is considered a positive result to suggest central hypersomnia20.
PARASOMNIAS
Outbreaks of atypical delta frequency activity have been detected during slow-wave sleep, immediately before or during an episode of pseudo-awakenings, for example, in non-REM parasomnia such as night terrors or sleepwalking21. However, EEG is not routinely indicated for the evaluation of these disorders. However, in PSG, an increase in latency to REM and non-REM sleep has been observed, as well as a reduction in the N1 and N2 states in a non-specific manner22. In REM parasomnias such as sleep paralysis, muscle atony has been documented in episodes of paralysis23, while in REM sleep behavior disorder; tone leakage and increased activity of electromyography activity are reported, associated with bizarre behavior during REM sleep24. In all these parasomnias, the events that characterize each of them can be recorded objectively and simultaneously on video recording.
DISORDERS OF CIRCADIAN SLEEP-WAKE RHYTHM
EEG is not very useful in these disorders; however, in irregular sleep rhythm disorder, an interhemispheric dyssynchrony between sleep spindles has been reported25. In PSG, in the disorder of advanced and delayed phase of sleep, the architecture of sleep is adequate, only that the time of sleep onset responds to the patient’s rest schedules, which occur at times that are out of step with those socially accepted26. In shift work disorder, alterations in sleep onset time, total sleep time, and sleep efficiency are reported in patients with these disorders27.
SLEEP-RELATED MOVEMENT DISORDERS
In restless legs syndrome (RLS) and periodic limb movement disorder during sleep (PLMD), the presence of an alternating cyclical pattern has been reported28 However, in general terms, EEG recording is not indicated in the evaluation of sleep-associated motor disorders. In PSG, sleep latency is prolonged, leg movements may be noticed when awake or shortly before the onset of sleep accompanied by increased activity of the appendicular muscles. There are usually several nighttime awakenings with long latency to restart sleep29. The rate of periodic limb movements in the sleeping state is increased to > 5 movements/hour, which supports the diagnosis of PLMD. A frequent association of RLS with PLMD can be found in the order of 70-90%. RLS and PLMD will produce morning sleepiness due to the alteration of sleep continuity. In nocturnal bruxism, an increase in rhythmic muscular masticatory activity is observed during sleep during various sleep states and is accompanied by micro-awakenings and therefore occurs with excessive daytime sleepiness, as well as pain and dental wear30.
SLEEP-RELATED MEDICAL AND NEUROLOGICAL DISORDERS
Epilepsies. Several types are favored by sleep in the N1 and N2 states because they increase the synchronization of the neural networks that produce the characteristic K complexes and sleep spindles and at the same time synchronize the abnormal epileptogenic tissue31. These include frontal lobe FLE, temporal lobe TLE, benign childhood epilepsy with centrotemporal spikes, BCECTS benign epilepsy with occipital spikes BEOS, juvenile myoclonic JME, generalized tonic-clonic seizures on awakening GTCSEA, West syndrome, Lennox-Gastaut syndrome, Landau-Kleffner syndrome, and continuous spike epilepsy during non-REM sleep (CSEnREM).
FLE. As the frontal lobe is the largest and contains numerous areas associated with various brain functions, including the primary motor and associative areas, eye movements, the motor area of language, for example, the FLE can present several symptoms of various modalities such as generalized tonic-clonic seizures, complex partial seizures, paroxysmal nocturnal pseudo-awakenings, paroxysmal nocturnal dystonia, paroxysmal nocturnal wandering, or sleep-related hypermotor seizures32. The interictal EEG pattern in wakefulness and sleep presents as spikes or slow wave-onset in the frontal and central regions that may evolve into a generalization of abnormal activity (Fig. 1).
TLE. The temporal lobe is also associated with various functions, but the clinical expression during sleep is less until the crisis is generalized. Seizures that come from deep regions such as the amygdala can be associated with complex partial seizures with bizarre behavior during the night33. Interictal EEG abnormalities can be observed in wakefulness and sleep in temporal leads with a tendency to generalization (Fig. 3).

Figure 3 Example of an electroencephalographic tracing of an epoch of 10 s in the N2 phase of sleep, in superior and inferior longitudinal assembly, right and left, showing two isolated tips that stand out from the base activity due to a left temporal-parietal phase inversion (between T3-T5/T5-O1 and C3-P3/P3-O1 electrodes), which presented a patient with focal temporal lobe epilepsy as an example of focal epilepsy.
BCECT. It presents as focal seizures characterized by ocular deviation, facial contractures, and vomiting that can produce rapid generalization. In the natural history of the disease, this alteration evolves into remission of the problem in a benign form. One of its main triggers is sleep deprivation. In the interictal EEG in wakefulness and sleep, it is observed that the abnormalities come from the central leads. Most seizures occur quickly after sleep or in the early morning hours34.
BEOS. It is a common epilepsy in childhood. Clinical presentation includes visual hallucinations, gaze deviation, and vomiting or discomfort induced primarily by flashes of light or from the television, computer, video games, or a screen phone. In this condition, spikes in the parieto-occipital and temporo-occipital leads are observed on the interictal EEG in wakefulness and light sleep. These alterations usually increase during intermittent light stimulation35.
JME. It is a hereditary condition characterized by the presence of myoclonic seizures with synchronous daytime shaking without loss of consciousness, some absence seizures, and generalized seizures. Myoclonic and generalized seizures frequently occur on awakening, they have a tendency to increase due to photosensitivity. It usually begins in adolescence. A characteristic generalized polyspike-slow wave pattern is usually observed on the interictal EEG, in wakefulness and sleep36.
West syndrome. It is a severe epileptiform encephalopathy that occurs in the 1st year of life. It consists of three main features: epileptic spasms, delayed psychomotor development, and a characteristic abnormal EEG pattern during sleep known as hypsarrhythmia (from Greek: hypsos = vertex, a = without, rhythmos = rhythm). In the interictal EEG in sleep, the baseline activity is abnormal with the presence of generalized high-voltage slow waves, multifocal spikes, and poor inter- or intra-hemispheric coherence alternating with short periods of voltage depression37.
Lennox-Gastaut syndrome. It is another encephalopathy condition present in childhood. It is characterized by a delay in psychomotor development, clonic, myoclonic, atonic epileptic seizures, and atypical absences, EEG with generalized slowing, and multifocal and generalized epileptiform elements. During interictal EEG recording in sleep, slowed background rhythm is observed with the presence of paroxysmal rapid activity, spikes, spike-wave complexes, and multifocal slow waves (Fig. 4)38.
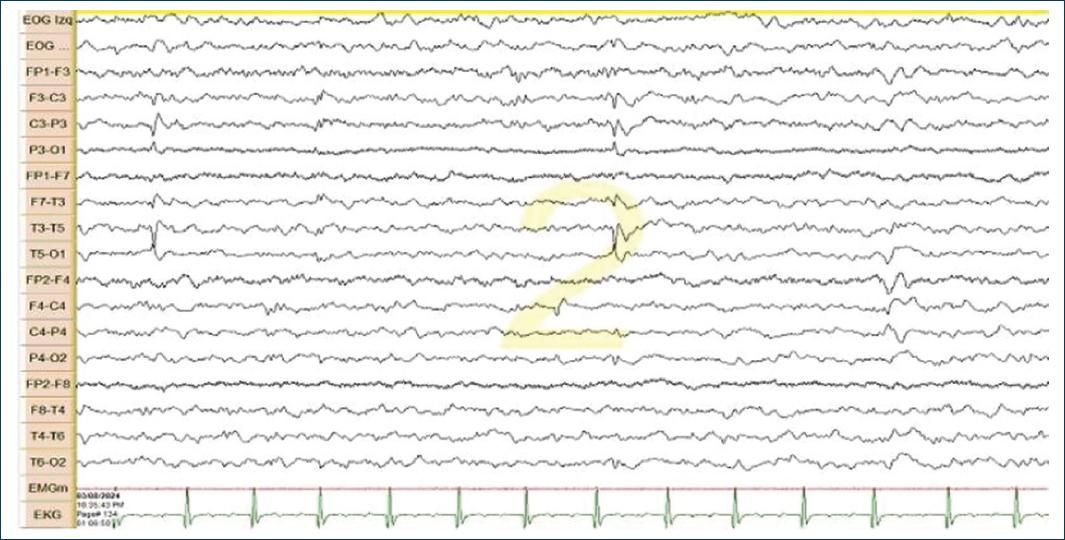
Figure 4 Example of a 10-s electroencephalographic tracing in the N2 sleep phase, in upper and lower, right and left longitudinal assembly showing slowed base activity, with scarce, asymmetrical and poorly organized sleep spindles and with brief outbreaks of 1-2 s, with generalized slow spike-wave complexes in a patient with Lennox-Gastaut syndrome as an example of generalized epilepsy.
CSEnREM. The abnormality initially presents as a delay in language development without motor alterations (Landau-Kleffner syndrome), generalized seizures may be observed in wakefulness. Subsequently, it is usually accompanied by significant motor, language, and cognitive impairment. In the EEG in sleep presents persistent generalized slow spike-wave complexes persistent during deep sleep without adequate organization of the initial phases of sleep39.
SDs induced by substance use
Anti-epileptic drugs can produce an increase in diffuse rapid activity of medium voltage40,41. Various antidepressants can cause voltage depression and increased rapid rhythms42,43. Computerized EEG analysis has been used to evaluate the alterations caused by the abuse of alcohol, nicotine, cannabinol, cocaine, opiates, and amphetamines, among other substances. Abnormalities of intrinsic activity, neural hyperactivation, and decreased neuronal communication between specific brain regions have been found. These alterations show partial recovery with abstinence44,45.
Conclusion
The EEG/PSG has proven to be a very useful para-clinical auxiliary tool in the evaluation of SD as it helps in the identification of various SDs and in the classification of various classes of sleep-associated epilepsies. It can also help to identify candidates for the use of non-invasive ventilation and the drugs necessary for its treatment. Other utilities are manifested in the study of wake/sleep rhythm and related research.
The spectral analysis of the EEG and the measurement of cortical connectivity will be useful tools in the near future for the evaluation of SD in which the EEG has had a lower use, such as in the study of insomnia, sleep-disordered breathing, hypersomnias, parasomnias, circadian rhythm disorders, and sleep-associated movement disorders.
Another useful use may be in the investigation of the pathophysiological mechanisms and effects of pharmacological and non-pharmacological treatment in SD.
As SD medicine is a relatively new and developing specialty, EEG can be used in the identification and description of new SDs and sleep-associated epilepsies.

