











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome, also referred to as Müllerian aplasia, is a congenital disorder characterized by aplasia of the uterus and upper part of the vagina in females with normal secondary sex characteristics and a normal female karyotype (46, XX)1.
The diagnosis is often made during adolescence following investigations for primary amenorrhea and has an estimated prevalence of one in 5000 live female births. MRKH syndrome is classified as Type I (isolated uterovaginal aplasia) or Type II (associated with extragenital manifestations)2. Extragenital anomalies typically include renal, skeletal, ear, or cardiac malformations2,3. The etiology of MRKH syndrome still remains elusive; however, increasing reports of familial clustering point toward genetic causes, and the use of various genomic techniques has allowed the identification of promising recurrent genetic abnormalities in some patients4.
Review of the McIndoe technique
Descriptions of congenital absence of the vagina have occurred in the literature for centuries, for example, Realdus Columbus (1572). However, centuries later the German anatomist Mayer (1829) was the first to describe a patient with vaginal agenesis and a rudimentary uterus, a malformation he named "uterus bipartitus."1 Over the next two centuries, descriptions by Rokitansky (1838), Küster (1910), and Hauser (1961) followed and led to the name of the syndrome1. Schmid-Tannwald and Hauser (1977) described cases of atypical MRKH syndrome with asymmetrically malformed ovaries, fallopian tubes, uterine buds, and renal abnormalities and Duncan et al. (1979) described cases of uterovaginal aplasia with renal and skeletal malformations, which was called MURCS association (Müllerian duct aplasia, renal aplasia, and cervicothoracic somite dysplasia)2.
The etiology of MRKH syndrome is unknown. For many years MRKH syndrome was thought to occur sporadically due to teratogenic exposure to drugs such as thalidomide (Hoffmann et al., 1976; Duncan et al., 1979). The idea of a non-genetic etiology was further supported by reports of discordance in monozygotic twins (Lischke et al., 1973; Regenstein and Berkeley, 1991) and missing recurrence in the outcome of surrogate pregnancies for intended mothers having MRKH syndrome (Petrozza et al., 1997). However, reports of familial clustering led to the idea of a genetic etiology. Hence far, a candidate gene approach has been used, investigating genes of known importance to urogenital embryologic development (AMH, AMHR2, WNT genes, WT1, LHX1, HNF1B, homeobox genes, PAX2, and others (Kobayashi et al., 2003) and genes causing diseases associated with MRKH syndrome such as GALT (Klipstein et al., 2003) and CFTR (Timmreck et al., 2003)2. Two types of MRKH syndrome have been described, referred to as Type 1 and Type 2. Type 1 MRKH syndrome occurs in an estimated 44% of MRKH patients and is described as a female presenting with Mullerian agenesis with a short vaginal pouch. Patients with Type 1 do not present congenital complications. Type 2 MRKH syndrome is estimated to present in 56% of cases, with Type 1 characteristics as well as with congenital abnormalities. These can include renal, skeletal, hearing, and cardiac complications (Table 1)3.
Table 1 Description of the treatment by others urogenital disorders
| Characteristics | SMRKH | Isolated vaginal atresia | WNT4 syndrome | Androgen insensitivity |
|---|---|---|---|---|
| Vaginal superior thrid | Absence | Variable | Absence | Absence |
| Uterus | Absence | Present | Absence | Absence |
| Gonads | Ovarius | Ovarius | Masculinization ovarius | Testicles |
| Breasts | Normal | Normal | Normal | Normal |
| Pubic hair | Norml | Normal | Normal | Scare |
| Hyperandrogenism | No | No | Yes | No |
| Karyotype | 46 XX | 46 XX | 46 XX | 46 XY |
Diagnosis of this syndrome is usually performed by means of ultrasound or magnetic resonance imaging. Treatment for these females consists of creating a sexually functioning neovagina and supportive psychological care2,3. Women with MRKH often present with a variety of complications. Most common are the difficulties in sexual intercourse and fertility. However, there is significant evidence in the literature to support that renal, skeletal, hearing, and cardiac complications can present in women with MRKH syndrome3. In the McIndoe procedure, skin is grafted to create epithelization of a surgical neovagina. An incision is made at the vaginal fovea, and a dissection is made in the vescirectal space to create a new vagina cavity. A skin graft is taken from the thigh or gluteal area, and the graft is wrapped around an acrylic mold, with the raw graft surface facing outward. The mold and graft are then inserted into the neovagina and left for about 2 weeks. During this period, the neovagina is thoroughly irrigated with sterile saline. After 2 weeks, patients are asked to dilate daily and to continue to use sterile saline3,4.
Abbé-McIndoe
This popular technique combines the retro vesical dissection described by McIndoe in 1938 and the use of a split-thickness skin graft (STSG) developed by Abbé4. Despite the procedure's relative simplicity and low complexity, complications such as graft contraction, partial graft take, and fistula formation may occur5. Advantages include minimal donor site morbidity, easy tissue harvesting, and avoidance of an abdominal approach. The most common drawbacks are vaginal dryness due to the absence of lubrication of the skin, prolonged use of a vaginal support, and visible scars at the donor site5. Functional success rates are around 80%. The surgery is successful when a ≥ 7 cm vagina with < 25% of graft contracture and a normal-looking functional neovagina are achieved5.
Technique
Pre-operative antibiotics and bowel preparation (to decrease inadvertent perforation) are recommended4,5. The approach is done through a perineal transverse or "Y-shaped" incision, then a space is created in the retro vesical space (between the urethra/bladder and rectum) with blunt dissection aiming to create a 12-13 cm length and 4.5-6 cm diameter cavity with the Douglas pouch as the upper and posterior limit. A < 0.5 cm thick and 18 cm wide and long STSG is harvested from a hair-free area, usually the posterior aspect of the thigh, inguinal area, buttocks, or suprapubic area. The graft is fenestrated and seated (with dermal surface facing toward the exterior) around a mold using mattress sutures with 4-0 polyglactin absorbable material. It is important to use a single suture line to secure the graft to the mold since this reduces potential graft contraction)5. Once the STSG is secured to the mold, it is introduced into the created space, and the free margins of the graft are fixed to the inner aspect of the labia and/or to the borders of the incision6. This mold is kept in place for 7-10 days and if it has a channel, patients can irrigate daily the neovagina with saline or diluted povidone-iodine solution (1%). Once the mold is removed and the neovagina is well-healed, regular penetrative intercourse or dilation (at least 3 times per week) is indicated to prevent contraction6. The mold is a key part of this procedure and can be created from different materials including a sponge, dental impression material, silicone, or latex which is wrapped with a soft sponge or a condom to ease insertion6. Many graft tissue variants have emerged over the past 10 years, including artificial dermis, human amnion, or oral mucosa graft, all with promising outcomes and decreased donor site morbidity6.
Materials and methods
An analysis of two cases operated in conjunction with the Gynecology and Plastic Surgery service was carried out, over a period of 4 years (from 2019 to 2022), with the McIndoe technique, evaluating the integration of the graft with the size of the conformer, and evaluating at the end of the 3rd month the sexual function by the Barcelona Scale.
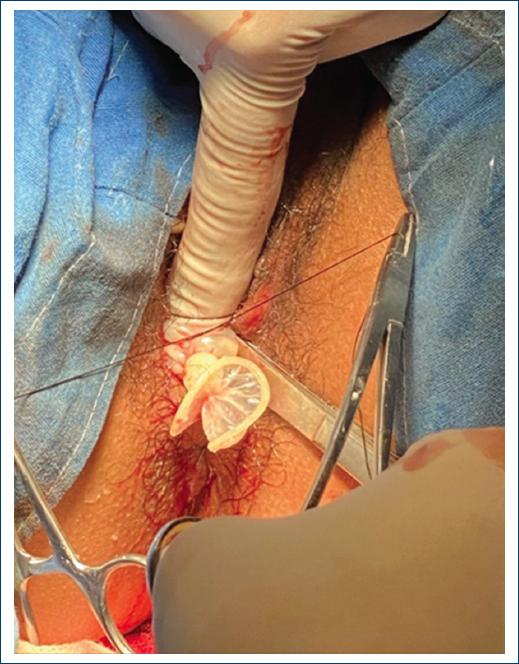
We made the surgery counting day 1, by the main object of created a neovagina with a 10-13 cm in average of deep (Fig. 1), and made the conformers with gauzes and extra strong condoms covered by a skin graft of 0.013 (Figs. 2 and 3), this conformer was placed in the neovagina, and removed at the day 7 to see the integration, during the follow-up of the patients, after the surgery the patients had to use a conformer of 12 cm in average, all day long for 2 weeks, and just remove in case of pain or during urination or evacuation, we cover the neovagina during 3 months until the skin graft were able to stabilize and have good vascularity, after we were sure of that, we order to them that they can began non-risky sexual relations, and evaluate in a Barcelona Scale (Fig. 4). The follow-up, to have an average of the deepness of the neovagina, was made at a year of being operated; we requested an X-ray with the conformer to size the neovagina and documented (Figs. 5 and 6).

Figure 2 P1RS: patient 1 Rokitansky syndrome; P2MS: patient 2 Morris syndrome. These are the results in a moderate range of sexual satisfaction 1 year after the McIndoe procedure.

Figure 3 The conformer made with extra durex material of latex, gauzes in the interior, Mepitel ONE®, and the partial thickness graft, with a long average of 13 in 66.6% of the patients.


Results
The results of the study showed that about two months after follow-up, during their initial sexual evaluation, both patients began sexual activity, with scores measured on a scale. The first patient a 25-year-old phenotypically female with 46XX karyotype, diagnosed with Rokitansky syndrome(P1RS) had a 28% satisfaction score, indicating a moderate level of satisfaction. The second patient a 31-year-old phenotypically female with 46XY sskaryotype, diagnosed with Morris syndrome (P2MS) had a satisfaction score of 36%, also indicating a moderate level of satisfaction.
During the follow-up, we assessed the depth of the neovagina using an X-ray of the pelvis. For the first patient, one year after follow-up, there was a 30% shortening of the neovagina depth, with an average depth of 8 cm from an initial 13 cm (Fig. 7). For the second patient, the neovagina depth was measured at 6 cm one and a half years after follow-up, showing a 50% shortening (Fig. 8).


In both patients, the initial best option for treatment was the McIndoe technique. The conformer was placed after 7 days, once the skin graft was integrated, and remained in the neovagina all day, except during urination and bowel movements. By the end of the first month, the conformer was removed at night, and by the end of the second month, it was no longer used. Subsequently, the patients could start having sexual relations. P1RS initiates sexual relations in the third month, reaching a score of 28 points on the Barcelona Scale, while P2MS obtains 36 points (Table 2). The primary objective of the study was to obtain a moderately to well-accepted and reproducible response, which suggests its viability as a first treatment option.
Table 2 Sexual satisfaction evaluation
| Personal approach | |||||
|---|---|---|---|---|---|
| 1. Sexual sensations | |||||
| Quality of caressing/feeling | Quality of sexual arousal | Frequency of excitation | Quality of orgasm | Orgasm frequency | |
| 1 | 2 | 2 | 3 | 3 | |
| 2. Sexual awareness | |||||
| Feeling of letting yourself go | To be centered | Sexual reaction to the couple | |||
| 2 | 1 | 2 | |||
| Relational approach | |||||
| 3. Sexual exchange | |||||
| The pleasure of receiving | Giving pleasure | Sexual availability of the couple | Sexual initiative of the couple | Sexual creativity of the couple | Balance between giving and receiving |
| 2 | 1 | 1 | 1 | 2 | 2 |
| 4. Emotional attachment | |||||
| Trust | Emotional openness | Emotional surrender of the couple | Emotional proximity | ||
| 1 | 1 | 1 | |||
| 1 | |||||
| Variety | Frequency | Intensity | Duration | ||
| 2 | 2 | 2 | 2 | ||
Evaluate with ratings from 1 to 3 according to the survey: 1. Good, 2. Acceptable, 3. Poor. < 25 = Bad response. Moderate response = 25-40. Good response = 40-. Value: patient 1 = 36; patient 2 = 28.
Discussion
In this study, sexual satisfaction was evaluated using the modified McIndoe technique in patients with urogenital disorders, through the application of the Barcelona Scale. The results obtained revealed that patients experienced a significant improvement in their sexual function after undergoing the surgical procedure. These findings conclusively support the hypothesis formulated at the beginning of the study, which held that the modified McIndoe technique would result in a substantial improvement in the patients' sexual function.
The main implication of these findings lies in the fact that the modified McIndoe technique is presented as a highly effective intervention to address urogenital disorders from a comprehensive perspective, not only resolving medical and anatomical concerns but also improving patients' sexual quality of life. This improvement in sexual function can have a positive impact on patients' self-esteem, confidence, and interpersonal relationships, thus contributing to their emotional and psychological well-being7.
The results of this study are consistent with previous research that has evaluated the effects of the modified McIndoe technique on sexual function. The previous studies have also noted significant improvements in patients' quality of sexual life after undergoing similar procedures. However, it is important to note that each study may differ in terms of patient population, methodology, and long-term follow-up. The convergence of these results with previous research strengthens the validity and clinical applicability of the modified McIndoe technique in the context of urogenital disorders.
This study provides strong and relevant evidence that the modified McIndoe technique leads to significant improvement in sexual function in patients with urogenital disorders, as assessed by the Barcelona Scale. These results support the importance of considering multidisciplinary approaches that address not only medical concerns but also the psychosocial dimensions of patients' health. Furthermore, it is hoped that these findings will encourage further research in the field and contribute to the optimization of surgical interventions in patients with urogenital disorders.
Complications and troubleshooting
Complications occur in 14% of cases including inadvertent rectal, urethral, bladder, bowel perforation, partial graft take, complete graft failure/graft necrosis, bleeding, fistula (rectovaginal, vesicovaginal and urethrovaginal), hair-growing vaginal skin, vaginal dryness, vaginal stenosis (pouch contracture), wound infection, keloid scar from the donor site and squamous adenocarcinoma8. The most common intraoperative complications with this technique according to a meta-analysis conducted in 2014 are intraoperative hemorrhage (< 1%) and rectal perforation (< 1%)8. Meticulous hemostasis is usually sufficient, but in the case of uncontrollable bleeding, cavity packing and blood transfusion may be needed. Rectal perforations can be repaired and the procedure finalized, but intestinal diversion should be concomitantly performed to avoid fistula formation9. The presence of fecal discharge and flatus through the neovagina are signs of fistula formation and a diverting colostomy should be performed as soon as possible with daily vaginal washing using saline, soap, or/and antiseptic. After confirming the cessation of the discharge (around 3 days after the colostomy is performed), the patient can replace a smaller mold to avoid putting pressure on the rectum9. After 12 weeks, a dye test can assess whether the fistula is still present and surgical repair can be planned. The use of a gracious flap is recommended in these cases. After 4 weeks, the colostomy can be taken down and dilations resumed10. In the case of urethral injury, a primary repair is often sufficient and should not affect outcomes. In case of bladder injury, the defect must be repaired and a catheter kept in place for 10-15 days. Youssef's syndrome triad (menouria, amenorrhea, and urinary incontinence) is a sign of vesicles-vaginal fistula. These complications are rare10.
The most feared complications are those related to the graft because they can lead to reoperation (< 10% in experienced hands). Partial graft take usually occurs at sites of infection or bleeding, causing granulation or neovaginal discharge. Most cases are successfully treated conservatively with silver nitrate cauterization or excision. Unfortunately, after the resolution, vaginal depth could be shortened1. Complete graft failure is mostly related to premature graft displacement or hematoma formed under the graft. Premature patient mobilization and the lack of bed rest the first post-operative week are the main causes of total graft failure. In these cases, reoperation with a new STSG is needed1. Donor site complications include bleeding, scarring, keloids, and hypertrophy, which may heal using topical treatments of corticosteroid injections10. Silver and the nanofibrillar cellulose dressings may promote donor site healing1. Late complications include neovagina dryness, stricture, contracture, urinary incontinence, granulation tissue, and recurrent urinary tract infections (UTI)1,9,10. Dryness can lead to pain and dyspareunia and lubricants are useful to reduce these symptoms. Stricture and contracture of the neovagina can be corrected with relaxing incisions and progressive dilation. Granulation tissue may be cauterized with silver nitrate or excised and recurrent UTIs may need prophylactic antibiotic therapy1.
Follow-up
Regular speculum examination is suggested to rule out malignancy or ulceration9. Because MRKH patients who are sexually active are at higher risk of getting a sexually transmitted infection, they should be screened at least 1 time annually and advised to use condoms. The human papillomavirus vaccination is recommended to decrease the risk of neoplasia and genital warts1.
Conclusion
In our study, we not only analyzed the surgical technique, which completely preserved its structural integrity, but also focused on preventing reductions in depth and width using the conformer. This approach led to acceptable sexual function in patients. We conclude that treating patients with Rokitansky Syndrome is more complex, requiring the use of the conformer for a longer period (as confidence takes longer to return compared to patients with Morris Syndrome). The reduction in depth was more significant in Rokitansky Syndrome patients over one year than in those with Morris Syndrome. Both patients were able to engage in sexual relationships with their partners and reported moderate satisfaction and full expectations.

