











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
The global increase in the elderly population has been accompanied by a rise in age-related physiological changes and chronic diseases. Cancer remains a leading cause of morbidity and mortality among older adults and is closely linked to advancing age and a heightened risk profile1. Colorectal cancer (CRC) is one of the most common malignancies worldwide and the most prevalent gastrointestinal tract cancer. According to global estimates from 2020, there were over 1.9 million new CRC cases and approximately 935,000 deaths, making it the second leading cause of cancer-related mortality globally2. In Türkiye, CRC ranks second among the most frequently diagnosed cancers and cancer-related deaths in the elderly population. Notably, it is the fourth most common cancer and the fourth leading cause of cancer-related death among both elderly men and women in Türkiye3,4.
The incidence and mortality of CRC increase with age, with the highest rates observed in individuals aged 65 years and older5. Epidemiological data from 1975 to 2006 show an overall decline in CRC incidence and mortality; however, this trend primarily benefited older populations. In individuals aged 65 and above, incidence rates declined by 4.6%, while those under 50 experienced a concerning annual increase of 1.6%. Importantly, mortality rates in this younger age group have also followed a similarly rising trajectory6.
Survival in CRC is influenced by several factors, including patient age, gender, disease stage at diagnosis, access to treatment, socioeconomic status, and the presence of comorbidities7. Individuals from lower socioeconomic backgrounds often face diagnostic delays and have limited access to healthcare services, which can postpone the initiation of treatment and negatively impact 5-year survival rates8. Numerous studies have demonstrated that early diagnosis and the application of effective treatment strategies significantly improve survival outcomes in elderly CRC patients9. Most CRCs develop through the malignant transformation of adenomatous polyps. The risk of malignant transformation is influenced by the polyps histological type, size, and the degree of cellular dysplasia. Since this transformation typically occurs over a prolonged period, often lasting 10 years or more, screening and early detection are considered essential components in the prevention and effective management of CRC10. Another important factor influencing prognosis in elderly patients with CRC is the treatment approach. Therapeutic decisions in this population require careful consideration due to age-related physiological changes and comorbidities. With the growing adoption of laparoscopic surgery, the use of minimally invasive techniques in elderly CRC patients has been associated with fewer post-operative complications, shorter hospital stays, and improved quality of life11. In addition, the variability in survival rates across different geographic regions and healthcare systems underscores the importance of health policies and treatment protocols in determining patient outcomes7,12.
Recent advances in surgical techniques, chemotherapy, and immunotherapy have led to significant improvements in the treatment of CRC13. However, the treatment process in elderly patients is often more complex than in younger individuals due to factors such as comorbidities, individual variability, and differences in treatment response9.
In a study conducted in Türkiye, including all age groups, the 5-year survival rate for CRC was found to be 49%14. In contrast, this rate is approximately 70% in the United States15. To date, no study has specifically investigated survival and the factors influencing it in elderly patients with CRC in Türkiye. The aim of this study is to evaluate 5-year survival rates, survival durations, and the factors affecting survival in patients aged 65 years and older diagnosed with CRC.
Method
This retrospective cohort study included CRC cases aged 65 years and older, who were registered in the Cancer Registry Database of the Sivas Provincial Health Directorate and had completed a 5-year follow-up period after diagnosis. Ethical approval was obtained from the Non-invasive Clinical Research Ethics Committee of Sivas Cumhuriyet University (January 18, 2023-January 08, 2023).
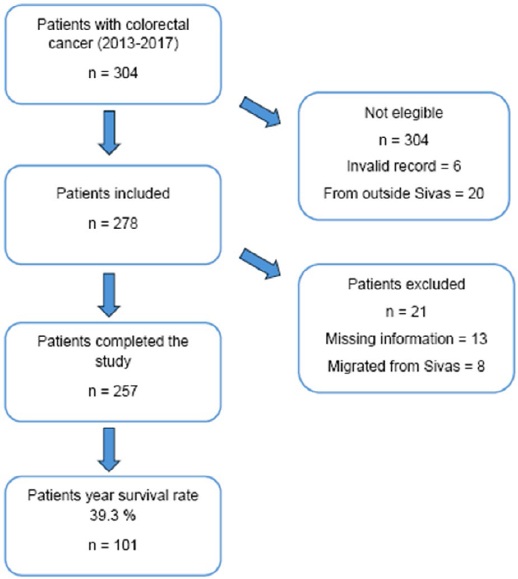
The required sample size was calculated using the OpenEpi program (updated April 06, 2013), based on a previously reported 49.0% 5-year survival rate from a national study on CRC in Türkiye, with a 6.0% margin of error14,16. Accordingly, the minimum required sample size was determined to be 267 patients. To approach this target while ensuring the inclusion of cases with completed 5-year follow-up, 257 eligible patients were selected from a total of 304 elderly CRC cases diagnosed between 2013 and 2017 (Fig. 1).
The dependent variable of the study is the 5-year survival rate; the survival rates of patients diagnosed with CRC between 2013 and 2017 were calculated for 1, 3, and 5 years. The independent variables are sociodemographic variables and disease-related factors. Sociodemographic variables include the patient's age (analyzed by grouping into young elderly [65-79 years] and very elderly [80 years and above]), gender, place of birth (Sivas and non-Sivas), health insurance status (evaluated in two groups: those with health insurance and those with a Green Card), place of residence (city center, district, and village), and the socio-economic development level of the districts in which they reside. The socioeconomic development level was determined using the Socioeconomic Development Ranking Report (SEGE-2017) prepared by the Ministry of Industry and Technology of the Republic of Türkiye17. In this report, districts are ranked from 1 to 6 based on their level of development. The most developed districts are in category 1, while the least developed districts are in category 6. Districts in Sivas province are ranked in categories 2, 3, 4, and 5.
Disease-related variables include the year of diagnosis (2013, 2014, 2015, 2016, 2017), histological type (adenocarcinoma, squamous cell carcinoma [SCC], neuroendocrine carcinoma, and lymphoma), metastasis status (yes, no), number of comorbidities (0, 1, 2 or more), treatment status (yes/no), treatment type (surgical, other [chemotherapy, radiotherapy, immunotherapy, hormone therapy], and both surgical and other types), and tumor number (single and multiple).
All statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 22.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation (min-max) and/or median with interquartile range (IQR), based on data distribution. Categorical variables were presented as counts and percentages. Survival estimates were obtained using the Kaplan-Meier method, and differences between survival curves were evaluated with the log-rank test. Variables with statistically significant associations in univariate analysis were included in a multivariate Cox proportional hazards regression model to determine independent predictors of survival. Hazard ratios (HR) with 95% confidence intervals (CIs) were reported, and a p < 0.05 was considered statistically significant.
Results
Among the 257 elderly CRC patients in the study group, 60.3% were male (n = 155). The proportion of patients born in Sivas was 95.3% (n = 245). The median age of the patients was 73.0 years (IQR 25-75: 68-78). When the age variable was grouped, it was found that the highest number of patients was in the 65-79 age group (80.5%). The proportion of patients living in the city center of Sivas was 54.1% (n = 139), while 20.2% (n = 52) lived in the districts, and 25.7% (n = 66) lived in villages. According to the SEGE 2017, 58.4% (n = 150) of patients live in the second category, which is the most developed level in Sivas province. The proportion of patients living in the lowest level, category five, was 19.1% (n = 49). All patients have health insurance, and 16.0% (n = 41) have a Green Card. The highest number of diagnoses was made in 2014 (n = 59). The distribution by year shows that the highest number of new CRC diagnoses occurred in 2014 (n = 59). It was observed that the number of patients decreased over the years (56 patients in 2013, 43 patients in 2017) (Table 1).
Table 1 Five-year survival rate and median survival time by sociodemographic characteristics
| n = 257 | Overall | Five-year survival rate (%) | Median survival (months) ± SE (95% CI) | p (log rank) | |
|---|---|---|---|---|---|
| n | % | ||||
| Gender | |||||
| Male | 155 | 60.3 | 37.4 | 23.58 ± 7.88 (8.14-39.03) | 0.238 |
| Female | 102 | 39.7 | 42.2 | 35.91 ± 11.84 (12.68-59.13) | |
| Age | |||||
| 65-79 | 207 | 80.5 | 43.0 | 33.97 ± 7.06 (20.11-47.82) | 0.017 |
| 80 and above | 50 | 19.5 | 24.0 | 16.59 ± 4.56 (7.63-25.54) | |
| Place of birth | |||||
| Sivas, n (%) | 245 | 95.3 | 40.4 | 31.54 ± 6.67 (18.45-44.62) | 0.107 |
| Other, n (%) | 12 | 4.7 | 16.7 | 18.00 ± 6.03 (6.18-29.82) | |
| Place of residence | |||||
| Center | 139 | 54.1 | 46.8 | 50.43 ± 11.25 (28.25-59.99) | 0.043 |
| District | 52 | 20.2 | 28.8 | 25.16 ± 7.34 (10.77 ± 39.56) | |
| Village | 66 | 25.7 | 31.8 | 13.70 ± 6.43 (1.07-26.32) | |
| District category (SEGE) | |||||
| Category 2 | 150 | 58.4 | 46.0 | 46.82 ± 11.91 (25.86-59.99) | 0.044 |
| Category 3-4 | 58 | 22.6 | 31.0 | 20.92 ± 9.15 (2.98-38.86) | |
| Category 5 | 49 | 19.1 | 28.6 | 21.35 ± 10.71 (0.35-42.35) | |
| Health assurance, n (%) | |||||
| Green card* | 41 | 16.0 | 40.3 | 31.70 ± 7.30 (17.37-46.02) | 0.562 |
| SGK + insured from abroad | 216 | 84.0 | 34.1 | 24.41 ± 5.25 (14.10-34.71) | |
| Years of diagnosis, n (%) | |||||
| 2013 | 56 | 21.8 | 35.7 | 20.92 ± 13.09 (0.00-46.58) | 0.427 |
| 2014 | 59 | 23.0 | 35.6 | 19.71 ± 6.12 (7.70-31.72) | |
| 2015 | 56 | 21.8 | 44.6 | 45.83 ± 13.52 (19.32-72.33) | |
| 2016 | 43 | 16.7 | 46.5 | 36.86 ± 9.05 (19.92-55.44) | |
| 2017 | 43 | 16.7 | 34.9 | 29.53 ± 4.58 (20.54-38.52) | |
*Green card: It is a card given by the state to those whose economic status is below 1/3 of the minimum wage. The patient benefits from public hospitals free of charge. Other: private insurance and overseas insurance.
CI: confidence interval; SE: Standard error; SGK: social security institution; SEGE: socioeconomic development ranking studies. Bold values indicate statistically significant results (p < 0.05).
About 95.7% (n = 246) of the patients were diagnosed with adenocarcinoma. According to the tumor location, the highest percentage, 71.2% (n = 183), was found in the colon, and 17.1% (n = 44) in the rectum. Treatment was applied to 74.7% (n = 192) of the patients. The proportion of patients who underwent surgical intervention was 74.0% (n = 142). The proportion of patients who did not receive treatment was 19.9% (n = 29). 14.4% (n = 37) had no chronic diseases, while 33.5% (n = 86) had two or more chronic diseases. The proportion of patients with metastasis at the time of diagnosis was 57.2% (n = 147) (Table 2).
Table 2 Five-year survival rate and median survival time by clinical characteristics
| n = 257 | Overall | Five-year survival rate (%) | Median survival (months) (95% CI) | p (log rank) | |
|---|---|---|---|---|---|
| n | % | ||||
| Histological type | 246 | 95.7 | 39.4 | 30.91 ± 6.09 (18.97-42.86) | 0.414 |
| Adenocarcinoma | 11 | 4.3 | 36.4 | 3.74 ± 4.70 (0.00-12.96) | |
| Other* | |||||
| Location | 183 | 71.2 | 39.9 | 29.53 ± 7.74 (14.35-44.71) | 0.991 |
| Colon | 74 | 28.8 | 37.8 | 30.91 ± 5.38 (20.36-41.47) | |
| Other** | |||||
| Treatment status*** | 192 | 74.7 | 41.1 | 37.22 ± 5.94 (25.58-48.86) | 0.044 |
| Yes | 29 | 19.9 | 28.1 | 10.25 ± 3.20 (3.96-16.53) | |
| No | |||||
| Treatment type | 142 | 74.0 | 40.1 | (Mean ± 95% CI) | 0.325 |
| Surgical | 23 | 12.0 | 34.8 | 33.54 ± 2.10 (29.42-37.67) | |
| Other | 27 | 14.0 | 51.9 | 32.12 ± 5.20 (21.89-42.35) | |
| Surgery + other | 42.19 ± 4.21 (33.92-50.45) | ||||
| Metastasis | < 0.001 | ||||
| No | 110 | 42.8 | 76.4 | 49.99 ± 1.92 (46.21-53.77) | |
| Yes | 147 | 57.2 | 11.6 | 19.40 ± 1.66 (16.14-22.67) | |
| Number of comorbid diseases**** | 0.268 | ||||
| No | 37 | 14.4 | 29.7 | 19.38 ± 5.39 (8.81-29.95) | |
| One | 115 | 44.7 | 40.9 | 35.91 ± 7.80 (20.62-51.20) | |
| 2 and above | 86 | 33.5 | 41.9 | 31.70 ± 9.58 (12.92-50.48) | |
| Tumor number | 0.379 | ||||
| Single primary | 234 | 91.1 | 40.2 | 30.91 ± 6.32 (18.52-43.31) | |
| Multi primary | 23 | 8.9 | 30.4 | 19.71 ± 17.65 (0.00-54.32) | |
*Histological type other: SCC, Lymphoma, neuroendocrine carcinoma.
**Location other: Anal, rectosigmoid junction, rectum.
***Patients with unknown treatment status were not included in the analysis 9.8%.
****Patients with unknown chronic disease were not included in the analysis 7.4%.
CI: confidence interval; SCC: squamous cell carcinoma. Bold values indicate statistically significant results (p < 0.05).
The 1-year survival rate in elderly patients with CRC was found to be 63.8% (n = 164). 58.7% of men survived at the end of the 1st year, while this rate was higher in women (71.6%). The proportion of those who survived at the 3rd year after diagnosis was 47.1% (n = 121). More than half of the male patients died by the end of the 3rd year (45.2%), while half of the female patients also passed away (50.0%). At the end of the 5th year, 39.3% (n = 101) of the study group remained alive. This rate was 37.4% (n = 58) in men and 42.2% (n = 41) in women (Table 3).
Table 3 One-, three-, and five-year survival rates and five-year mean and median values by gender
| Survival rate (n = 257) | Total | Female (n = 102) | Male (n = 155) | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| One-year survival | 164 | 63.8 | 73 | 71.6 | 91 | 58.7 |
| Three-year survival | 121 | 47.1 | 51 | 50.0 | 70 | 45.2 |
| Five-year survival | 101 | 39.3 | 41 | 42.2 | 58 | 37.4 |
| Five-year survival duration (months) | ||||||
| Mean ± SE (95% CI) | 32.50 ± 1.57 (29.41-35.85) | 35.45 ± 2.41 (30.72-40.18) | 30.54 ± 2.05 (26.52-34.58) | |||
| Median ± SE (95% CI) | 30.48 ± 5.99 (18.73-42.24) | 35.91 ± 11.84 (12.68-59.13) | 23.58 ± 7.88 (8.14-39.03) | |||
CI: confidence interval; SE: standard error.
The 5-year median survival time was 35.91 ± 11.84 months (95% CI 12.68-59.13) in women and 23.58 ± 7.88 months (95% CI 8.14-39.03) in men (Table 3). When evaluated by age groups, the survival rate was 43.0% (n = 89) in the 65-79 age group, while it was 24.0% (n = 12) in those aged 80 and above. The median survival time was 33.97 ± 7.06 months (95% CI 20.11-47.82) in the 65-79 age group and 16.59 ± 4.56 months (95% CI: 7.63-25.54) in those aged 80 and above (p = 0.019) (Fig. 2A and Table 1).
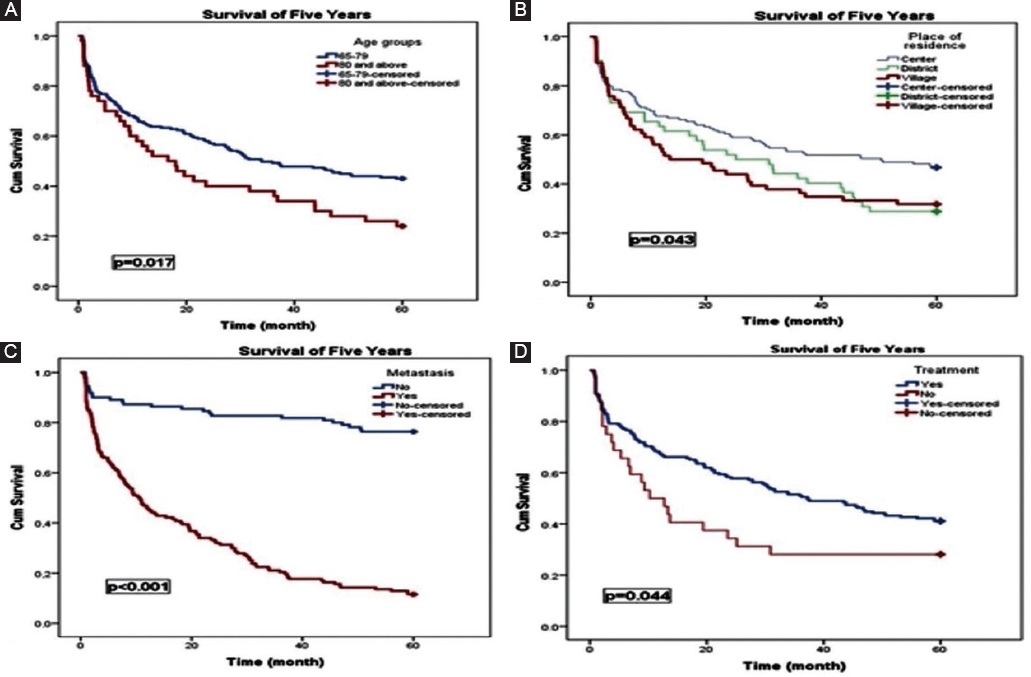
Figure 2 Kaplan-Meier survival curves showing 5-year survival according to (A) age groups, (B) place of residence, (C) metastasis status, and (D) treatment status.
In the city center of Sivas, 46.8% (n = 65) survived at the end of 5 years, while 28.8% (n = 15) of those living in the districts and 31.8% (n = 21) of those living in the villages survived (Table 1). The median survival time was 50.43 ± 11.25 months (95% CI: 28.25-59.99) in the city center, while it was 13.70 ± 6.43 months (95% CI: 1.07-26.32) in the villages (p = 0.043) (Fig. 2B and Table 1).
In the city center, with a development level of 2, the 5-year survival rate was 46.0% (n = 69), while it was 28.6% (n = 14) in those living in level 5 areas. The median survival time in level 2 areas was 46.82 ± 11.91 months (95% CI: 25.86-59.99), while it was 21.35 ± 10.71 months (95% CI: 0.35-42.35) in level 5 areas (p = 0.044) (Table 1).
The survival rate was 40.3% (n = 87) for those with health insurance and 34.1% (n = 14) for those with a Green Card. The mean survival time for those with health insurance was 32.90 ± 1.73 months (95% CI: 29.51-36.30), while for those with a Green Card, it was 30.35 ± 3.75 months (95% CI: 23.03-37.67) (Table 1).
When survival rates were examined according to the characteristics of the disease, 39.4% (n = 97) of patients diagnosed with adenocarcinoma and 36.4% (n = 4) of patients in the other group (SCC, lymphoma, neuroendocrine carcinoma) survived the 5-year survival period. The 5-year median survival time for adenocarcinoma patients was 30.91 ± 6.09 months (95% CI: 18.97-42.86), while for the other group, it was 3.74 ± 4.70 months (95% CI: 0.00-12.96) (Table 2).
About 39.9% (n = 73) of patients with colon cancer and 37.8% (n = 28) of those in the other group (anal, rectosigmoid junction, and rectum) survived the 5-year survival period. The median survival time for patients with colon cancer was 29.53 ± 7.74 months (95% CI: 14.35-44.71), while for those in the other group, the median survival time was 30.91 ± 5.38 months (95% CI: 20.36-41.47) (Table 2).
Among CRC patients with metastasis, 11.6% (n = 17) completed the 5-year survival period. In contrast, 76.4% (n = 84) of those without metastasis survived. The median survival time for patients without metastasis was 49.99 ± 1.92 months (95% CI: 46.21-53.77), while for those with metastasis, it was 19.40 ± 1.66 months (95% CI: 16.14-22.67) (p < 0.001) (Fig. 2C and Table 2).
Of the 224 patients who received treatment, 41.1% (n = 79) survived the 5-year survival period, while 28.1% (n = 9) of those who did not receive treatment survived for the same period. The 5-year median survival time for patients who received treatment was 37.22 ± 5.94 months (95% CI: 25.58-48.86), while for those who did not receive treatment, it was 10.25 ± 3.20 months (95% CI: 3.96-16.53) (p = 0.044) (Fig. 2D).
The highest survival rate among treatment types was observed in patients who received both surgical and other treatment methods (51.9%, n = 27). The median survival time was also longest in this group, with those receiving both surgical and other treatments having a median survival time of 42.19 ± 4.21 months (95% CI: 33.92-50.45) (Table 2).
In the research group, the 5-year survival rate for patients without any chronic diseases was 29.7% (n = 11), while for those with two or more chronic diseases, the survival rate was 41.9% (n = 36). The median survival time for patients without chronic diseases was 19.38 ± 5.39 months (95% CI: 8.81-29.95), whereas for those with two or more chronic diseases, it was 35.91 ± 7.80 months (95% CI: 20.62-51.20). There was no statistically significant relationship (Table 2).
In our study, the 5-year survival rate for patients with a single primary tumor was 40.2%, while for those with multiple primary tumors, the survival rate was 30.4%. The median survival time for patients with a single primary tumor was 30.91 ± 6.32 months (95% CI: 18.52-43.31), whereas for those with multiple primary tumors, it was 19.71 ± 17.65 months (95% CI: 0.00-54.32). However, this difference was not found to be statistically significant.
In this study, the variables that were included in the Cox regression analysis, which showed statistically significant results in the log-rank test, were age group, district development level, treatment status, metastasis, and gender. According to the results of the Cox regression analysis, the presence of metastasis was identified as the variable with the strongest impact on survival (p < 0.001). The risk of death in patients with metastasis was found to be 7.77 times higher compared to patients without metastasis (Table 4).
Table 4 Cox regression analysis of factors associated with 5-year survival
| Survival time of 5 years | ||
|---|---|---|
| Variable | Hazard ratio (95% CI) | p |
| Gender | ||
| Female | 1.00 (reference) | |
| Male | 1.25 (0.90-1.75) | 0.177 |
| Age | ||
| 65-79 | 1.00 (reference) | |
| 80 and above | 1.38 (0.94-2.02) | 0.092 |
| District category | ||
| Category 2 | 1.00 (reference) | |
| Category 3-4 | 1.28 (0.87-1.89) | 0.412 |
| Category 5 | 1.30 (0.86-1.97) | 0.212 |
| Treatment status | ||
| Yes | 1.00 (reference) | 0.003 |
| No | 2.00 (1.26-3.17) | |
| Metastasis | ||
| No | 1.0 (reference) | |
| Yes | 7.76 (5.01-12.03) | < 0.001 |
CI: confidence interval. Bold values indicate statistically significant results (p < 0.05).
Receiving treatment for CRC was identified as a significant factor for survival in elderly patients (p = 0.008). The risk of death in patients who did not receive treatment was found to be higher compared to those who received treatment (p = 0.003).
Although higher mortality risk was observed in male patients, those aged 80 and above, and those living in socio-economically less developed areas, Cox regression analysis did not find these differences to be statistically significant.
Discussion
In this study, the 5-year survival rates of elderly patients with CRC and the factors affecting these rates were analyzed. The median survival time was found to be 30.48 months. Shorter median survival times were observed in patients aged 80 and above, those living in rural areas, those residing in areas with a fifth-level development status, patients with metastasis, and those who did not receive treatment. After Cox regression analysis, it was determined that the risk of death was higher in patients who did not receive treatment and in those with metastasis.
In this study, the 5-year survival rate was determined to be 39.3%. In a study conducted by Joachim et al., between 2008 and 2012 with 2230 elderly patients in the Caribbean, the 5-year survival rate was found to be similar at 38.2%18. In studies that include all age groups, higher survival rates have been observed. In the United States, the 5-year survival rate for CRC across all age groups was reported as 65% for the period 2012-201815. In a study conducted by Leong et al., this rate was found to be 49.6%19. In Brazil, a study by Silva et al., which focused solely on deaths related to CRC, found the 5-year survival rate to be 84.2%20. In a study conducted in Turkey, the 5-year overall survival rate for CRC patients across all age groups was reported as 49%14. Differences in survival rates may be attributed to the demographic characteristics of the patient populations in these studies, as well as the stage distribution at the time of diagnosis and variations in the treatment protocols applied.
In this study, a significant relationship was found between survival time and age groups. Survival time and rates for those aged 80 and above were significantly lower compared to the 65-79 age group. Similar studies have reported that as age increases, particularly after the 7th decade, survival rates and times for CRC patients decrease15,21. In the literature, this has been attributed to the inability to apply aggressive treatments in older ages and the presence of metastases22,23.
In the study group, CRC was found to be more common in men. Studies in the literature also show that CRC is more prevalent in men in the older age group. This finding is consistent with the current literature8,24-27. In addition, our study found that the 5-year average lifespan was shorter in men. This result is similar to previous studies15,18,28. Some studies explain this finding by the generally shorter average lifespan of men compared to women28.
In this study, when evaluated in terms of regional inequality indicators, it was found that the risk of death was higher in individuals living in villages and districts compared to those living in the city center of Sivas. Similarly, according to SEGE 2017 data, individuals living in regions with a lower development level also exhibited an increased risk of death. In the individual inequality indicator, health insurance, it was found that individuals with a green card had a higher risk of death. These findings, reflecting socioeconomic status and consistent with studies in the literature, were significant in univariate analyses, but no significance was observed in multivariate analyses. Research has shown that both regional and individual inequalities increase the risk of death, and socioeconomic status is emphasized as an important prognostic factor for cancer survival. Factors such as access to healthcare services, benefiting from advancements in cancer surgery and treatment, access to screening methods, and the control of comorbidities contribute to longer survival times in individuals living in regions with a higher socio-economic status. In contrast, it has been reported that survival times are shorter in individuals who are unable to benefit adequately from these opportunities and those living in rural areas15,17,29,30.
In the study group, it was determined that the most common histological subtype was adenocarcinoma (95.7%). Leong et al. reported this rate as 83.1%19, while in the study by Tamakoshi et al., the adenocarcinoma rate was found to be 95%31. In the study by Degu et al, the adenocarcinoma rate was found to be 99.6%27. In this study, no statistically significant relationship was found between the histological subtype of cancer and survival time. Similarly, in many studies in the literature, no significant relationship was identified between the type of cancer and survival32. Particularly in studies conducted in elderly patient groups, it has been reported that the histological subtype of cancer is not a determining factor for survival18.
It was determined that 71.2% of the study group had colon cancer, and 17.1% had rectal cancer. In similar studies in the literature, the most common type of CRC is colon cancer, and colon cancer ranks first19,32-34. However, in this study, no significant difference in survival was found between colon and rectal cancers. This finding is consistent with other studies in the literature17,35. However, in some studies, it has been reported that the survival rates for rectal cancer are lower compared to colon cancer18,33-34. It is believed that this difference could be attributed to factors such as the use of different treatment methods, patients overall health status, and disease stage.
In this study, it was determined that 57.2% of the study group had metastasis at the time of diagnosis. According to the 2023 data by Siegel et al., the metastasis rate in CRC patients over 65-years-old is 56.0%5. In a study by Joachim et al., this rate was reported to be 63.0%18. This finding, consistent with the literature, shows that metastasis is an important prognostic factor in elderly patients with CRC.
In the study group, 11.6% of patients with metastasis completed the 5-year survival period. The literature reports that elderly patients with metastatic CRC have shorter survival times, and metastasis, particularly spread to organs such as the liver, lungs, lymph nodes, bones, brain, and peritoneum, negatively affects survival22. In addition, in elderly patients, the effect of metastasis is associated with various factors such as biological age, comorbidities, response to treatment, and changes in quality of life. CRC tends to develop at more advanced stages and more aggressively in elderly patients. In elderly individuals, cancer is typically diagnosed later, and detection of the disease at advanced stages complicates treatment response. Biological changes occurring in the body with age significantly affect the progression of cancer. Especially in patients over 70 years of age, metastasis can progress more rapidly, limiting treatment options. Elderly patients responses to treatment are generally weaker compared to younger patients, and treatment side effects can be more severe. Therefore, survival times in elderly patients with metastatic CRC are generally shorter23.
In this study, survival time and survival rate were found to be lower in patients who did not receive treatment. Literature indicates that elderly cancer patients face many barriers regarding their treatment status. These barriers are often due to the physician's approach to treatment, as well as the attitudes of the patient and their family. Barriers to treatment in elderly patients include frailty, multiple comorbidities, limitations in treatment eligibility, and the inability to recommend standard or more aggressive treatment options36. This situation leads to restrictions in treatment decisions for elderly patients and consequently negatively impacts their survival. Some studies have indicated that difficulties regarding treatment decisions for elderly cancer patients are more pronounced. For example, it has been reported that two-thirds of elderly cancer patients have limited treatment options when making treatment decisions37. This situation negatively affects the survival rates of patients who do not receive treatment. In addition, elderly patients' responses to treatment are generally weaker compared to younger patients32. It has been observed that survival times in cancer patients who do not receive treatment are generally shorter, with challenges in treatment resistance, treatment adherence, and treatment responses being more frequent among elderly patients. However, some elderly patients may prefer not to receive treatment, as they believe it may reduce their quality of life and may not be effective38. The literature also suggests that elderly patients with CRC are less likely to receive the recommended treatments9.
Conclusions
The Cox regression analysis conducted in this study demonstrated that the 5-year mortality risk was significantly higher among patients with metastases and those who did not receive treatment. These findings align with existing literature, where metastasis and treatment have been consistently identified as key prognostic factors14. Furthermore, socioeconomic status and regional disparities are critical determinants influencing the effectiveness of cancer treatment and patient survival outcomes. These results underscore the necessity for more equitable and effective healthcare policies and service organization. The data obtained in this study hold particular importance for healthcare planning for the elderly population, emphasizing the need to strengthen local healthcare infrastructure and develop targeted strategies for cancer treatment.
This study has several limitations. First, the use of data from a single province and the retrospective design limit the generalizability of the results. In addition, the lack of access to individual-level socioeconomic data, which serve as important indicators of inequality, prevented the assessment of their impact on survival outcomes.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institutions confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.

