











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
At the end of December 2019, a new viral infection belonging to the Coronavirus family emerged in China1, which spread rapidly worldwide2. The COVID-19 disease requires hospitalization in 20% of patients, 33.7% of whom require admission to the intensive care unit, with a mortality rate reaching up to 62.4%3. The need to find an urgent treatment to reduce the impact of the pandemic has led to the use of different therapeutic options, among them is the fixed combination of hydroxychloroquine (HCQ) and azithromycin (AZT), which became a promising option4,5.
HCQ exhibits non-specific antiviral activity in vitro against a wide range of emerging viruses and, more recently, against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in addition to its anti-inflammatory activity6,7. On the other hand, AZT is a macrolide antibiotic, which has shown anti-inflammatory and antiviral effects in vitro8, which is why it was proposed as an accessible and cost-effective option for SARS-CoV-2 infection9.
Even if these drugs have demonstrated efficacy in vitro nowadays, clinical results on the beneficial effect of the fixed combination HCQ + AZT in hospitalized or mechanically ventilated patients are inconsistent10,11, which is attributed to the delayed initiation of treatment12. Therefore, it is hypothesized that early use of these drugs is necessary to achieve benefits to prevent hospitalizations. This study aimed at determining the efficacy and safety of the fixed combination of HCQ + AZT compared to HCQ or placebo in mild COVID-19 outpatients to avoid hospitalizations13.
Method
Trial design
This study was designed as a multicenter, parallel, double-blind, randomized clinical trial. The study was conducted in two public ambulatory family medicine units, in Mexico City (UMF No. 28) and in the State of México (UMF No. 52). The protocol was approved by the National Research Committee Institutions review board of the IMSS with the number R-2020-785-138 and by COFEPRIS. Written informed consent was obtained from each of the included participants. Ultra-laboratories were the sponsors of the study; nonetheless, they were not involved in the development of the study, the analysis of results, or the preparation of the manuscript. The trial was registered at clinicaltrials.gov (clinical trials: NCT04964583). This report follows the CONSORT guidelines.
Eligible subjects
The study included patients aged 18-76 years who were diagnosed with mild COVID-19 with acute respiratory disease and who met the current operational definition of the Ministry of Health of Mexico14. The diagnosis was confirmed by reverse transcription-polymerase chain reaction (RT-PCR) for SARS-CoV-2; the severity of the disease was evaluated with the National Early Warning Score (NEWS). Patients with a score ≤ 4 points were considered to have mild disease.
Patients with cardiac disorders with delayed cardiac conduction (QT segment ≥ 450 ms), pregnant or lactating women, patients with hypersensitivity to study drugs, patients with chronic renal failure with (estimated glomerular filtration rate < 40 mL/min), patients with a history of retinopathy or macular degeneration, those with known glucose-6-phosphate dehydrogenase deficiency, and patients with liver disease were excluded from the study.
Intervention
Participants were randomly assigned to one of the three treatment arms. The participants in Group 1 (HCQ + AZT) received HCQ 200 mg/AZT 250 mg (provided by Ultra Laboratorios®) orally every 12 h for 5 days, followed by HCQ 200 mg (Plaquenil® from Sanofi Aventis, México) every 12 h for 5 more days. The participants in Group 2 (HCQ) received only HCQ 200 mg orally every 12 h for 10 days. The participants in Group 3 received an oral placebo (provided by Ultra Laboratorios®) every 12 h for 10 days. The placebo and active treatment were identical in appearance. Double-blinding was preserved until the end of the analysis of the results. All three treatment groups received symptomatic treatment for the management of COVID-19; the current standard was at the discretion of the treating physician based on acetaminophen, antihistamines, non-steroidal analgesics, and ivermectin. A computerized random number sequence was generated for assignment to study treatment groups and was stratified according to center. Randomization was carried out by one of the investigators who did not participate in the inclusion of patients or in the delivery of medication. The medical staff was responsible for the recruitment and selection of participants and the evaluation of the correct allocation of treatment according to the randomization. Adherence to treatment was evaluated by counting the tablets during the medical consultation and by the intake recorded by the participants in the digital application for smartphones.
Follow-up
The follow-up was carried out through a Web App on a smartphone, recording the medication intake, adverse events, oxygen saturation, and temperature. A clinical examination was performed at the time of inclusion, on days 6 and 11 after initiating the treatment, in which an evaluation of the severity of the disease was carried out along with an RT-PCR test, an electrocardiogram, and follow-up laboratory studies, a count of tablets to evaluate therapeutic adherence, and a radiography taken at the beginning of the study and on day 11. On day 21 of the follow-up, the participants were called by phone to evaluate symptoms and to investigate whether the patient had returned to routine activities, required hospitalization, or had any of the secondary outcomes.
Outcomes
The primary outcome of the study was hospitalization during the 21 days of the follow-up. The secondary outcomes included disease progression, which was defined by oxygen saturation < 90%, dyspnea, or pneumonia15, use of supplemental oxygen, and the presence of adverse events during the 21 days of follow-up.
Drug safety
All adverse events reported by the participants during the study period in the electronic patient diary app or during medical consultations were recorded. To assess the safety of the drug, QT intervals were measured by a certified cardiologist using the Bazett formula by performing a 12-lead electrocardiogram at the inclusion visit, on days 6 and 11 of the follow-up.
Sample size
The sample size was calculated using a comparative study formula. An expected difference of 40% in the clinical response between HCQ + AZT treatment and placebo was considered, an a error of 5%, and a statistical power of 80%. The estimated sample size obtained from the calculation was 84 participants, 28 participants per group, to which 20% was added for possible losses, obtaining a sample size of 105 participants. We used the Fleiss formula with continuity correction (Fleiss w/CC). Due to the decrease in the number of COVID-19 patients, only 92 participants were included.
Descriptive and inferential statistics
A descriptive analysis was carried out to determine the general characteristics of the population16.
To determine if there were differences in the baseline status of the population by the treatment assignment, the ANOVA test was used for systolic and diastolic pressure, PCR (computed tomography), total leukocytes and lymphocytes, the Kruskal-Wallis test was used for age, body mass index, temperature, oxygen saturation, NEWS, glucose, urea, lactic dehydrogenase, gamma-glutamyl transpeptidase, transaminases, serum iron, neutrophils and platelets, and the Pearsons X2 test or Fisher's exact test was used for sex, comorbidities, smoking and ivermectin.
The incidence of hospitalization, disease progression, pneumonia, use of supplemental oxygen on day 21, and negative test (PCR) on day 11 was determined according to the treatment assignment as a measure of association. The relative risk (RR) was calculated, with its 95% confidence interval17. A multiple logistic regression analysis was performed to evaluate the predictors of pneumonia adjusted for treatment, age, and comorbidities. Alpha was set at 5%, all data were analyzed using IBM Statistical Package for the Social Sciences v.28 (IBM Corp, NY, USA).
Clinical safety analysis
The safety analysis was carried out considering all the participants regardless of their completion of the study. The frequency and severity of the adverse events presented by the participants during the study were determined, and a comparison was made according to the types of treatment given using Pearson's X2 test or Fisher's exact test.
Results
Study population
From January 20 to August 20, 2021, 245 mild COVID-19 participants were invited to the study. One hundred and fifty-three patients were excluded, as shown in figure 1. A total of 92 participants were randomized and included in the intention-to-treat analysis.
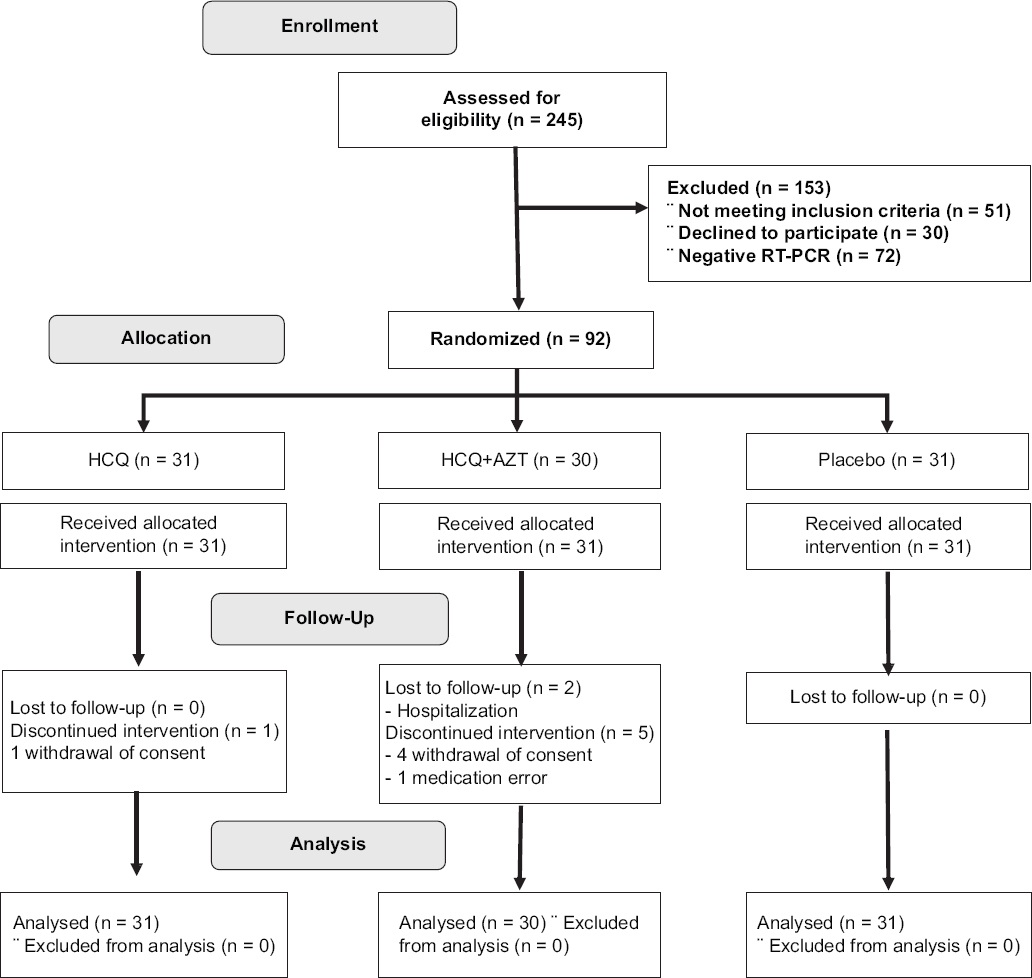
The median age was 37 years; 27.2% of the patients had comorbidities. The analysis of the time of evolution at the initiation of treatment revealed a median of 5 days, with a median saturation of 94%. The incidence of hospitalization in the study population was 2.2% (Table 1).
Table 1 General characteristics according to treatment arm
| Variables | Total n = 92 | HCQ n = 31 | HCQ+AZT n = 30 | Placebo n = 31 | p |
|---|---|---|---|---|---|
| Age (years)b | 37 (27.5-50.5) | 38 (24-49.5) | 41 (33.7-49.5) | 32 (24-51) | 0.34 |
| Male sex (n,%)c | 45 (48.9) | 13 (41.9) | 12 (40.0) | 20 (64.5) | 0.07 |
| Comorbidities (n,%)c | 25 (27.2) | 9 (29.0) | 7 (23.3) | 9 (29.0) | 1.0 |
| Smoking (n,%)c | 32 (34.8) | 10 (32.3) | 9 (30.0) | 13 (41.9) | 0.42 |
| Time of evolution until treatment start (days)b | 5 (3, 6) | 5 (4, 6) | 5 (3, 6) | 5 (3, 7) | 0.78 |
| Ivermectin (n,%) | 11 (11.9) | 7 (22.6) | 3 (10.0) | 1 (3.2) | 0.06 |
| BMI (Kg/m2)b | 26.9 (24.4-30.1) | 26.9 (24.6-28.6) | 27.3 (25.2-30.4) | 25.6 (24.1-31.7) | 0.53 |
| Temperature (°C)b | 36.6 (36.4-36.8) | 36.7 (36.4-36.8) | 36.6 (36.4-36.8) | 36.6 (36.5-36.8) | 0.97 |
| Systolic pressure (mmHg)a | 117.7 ± 13.7 | 117.2 ± 13.9 | 117.0 ± 12.5 | 118.3 ± 14.7 | 0.93 |
| Diastolic pressure (mmHg)a | 78.6 ± 8.4 | 78.3 ± 8.1 | 78.5 ± 8.8 | 78.9 ± 8.8 | 0.97 |
| Oxygen saturation (%)b | 94 (93-96) | 95 (93.7-96) | 94 (92-95) | 94 (93-96) | 0.53 |
| National early warning scoreb | 1 (0, 2) | 0.5 (0, 2) | 1 (0, 2) | 2 (0, 2) | 0.43 |
| PCR (CT)a | 26.6 ± 4.7 | 26.2 ± 4.8 | 26.4 ± 4.9 | 27.1 ± 4.5 | 0.72 |
| Glucose (mg/dL)b | 88.7 (79.3-96.3) | 92.4 (75.5-101.6) | 88.2 (78.8-99.5) | 84.6 (79.6-92.5) | 0.28 |
| Urea (mg/dL)a | 25.5 (21.1-33.1) | 26.8 (21.0-33.6) | 25.1 (19.5-33.3) | 24.9 (22.1-32.8) | 0.85 |
| Lactic dehydrogenase (U/L)b | 196.6 (164.6-221.1) | 198.3 (158.4-231.4) | 194.5 (167.7-217.5) | 182.9 (166.5-220.6) | 0.97 |
| Gamma glutamil transferasa (U/L)b | 32.9 (21.1-66.1) | 31.8 (21.2-66.9) | 35.8 (19.2-73.3) | 32.8 (21.9-65.7) | 0.98 |
| Glutamic pyruvic transaminase (U/L)b | 33.6 (19.9-55.3) | 36.7 (21.6-54.1) | 33.4 (23.3-58.7) | 24.2 (15.4-54.3) | 0.45 |
| Glutamic oxaloacetic transaminase (U/L)b | 31.5 (25.3-44.5) | 32.1 (27.7-46.8) | 32.0 (24.7-42.1) | 29.6 (23.7-40.8) | 0.53 |
| Serum iron (ug/dL)a | 50.8 (35.4-69.4) | 48.5 (32.7-69.8) | 55.1 (37.6-73.2) | 47.2 (35.3-65.3) | 0.56 |
| Total leukocytes (K/L)a | 4.99 ± 1.49 | 5.1 ± 1.5 | 5.1 ± 1.6 | 4.8 ± 1.2 | 0.78 |
| Neutrophils (K/L)b | 2.7 (2.3-3.8) | 2.7 (2.3-4.1) | 2.8 (2.1-3.9) | 2.7 (1.9-3.7) | 0.71 |
| Lymphocytes (K/L)a | 1.2 ± 0.4 | 1.2 ± 0.4 | 1.2 ± 0.4 | 1.2 ± 0.4 | 0.99 |
| Platelets (K/L)b | 212 (172-256.5) | 212 (175-257) | 202 (157.7-266) | 218.5 (181-257.5) | 0.76 |
aData is presented as mean, standard deviation, and statistical was done was ANOVA.
bData is presented as median and interquartile range 25-75 (IQR), statistical test was Kruskal-Wallis.
cData are presented as frequencies and percentages, statistical test was X2.
HCQ: hydroxychloroquine, AZT: azithromycin, IQR: interquartile range, ANOVA: analysis of variance.
Primary outcome
The analysis of the therapeutic efficacy to reduce the risk of hospitalization revealed that the incidence of the outcome in the HCQ + AZT group was 6.7% (2/30) compared to the HCQ group and the placebo group, in which there were no hospitalizations (Table 2). The use of ivermectin was not associated with hospitalization, pneumonia, or disease progression.
Table 2 Efficacy of treatment for primary and secondary outcomes
| Outcomes | HCQ+AZT n = 30 (%) | HCQ n = 31 (%) | Placebo n = 31 (%) | HCQ+AZT versus placebo RR (CI 95%) | p | HCQ versus placebo RR (95% IC) | p |
|---|---|---|---|---|---|---|---|
| Primary | |||||||
| Hospitalization | 2 (6.7) | 0 (0) | 0 (0) | NC | - | NC | - |
| Secondary outcomes | |||||||
| Progression | 9 (30) | 13 (41.9) | 4 (12.9) | 2.32 (0.80, 6.74) | 0.10 | 3.25 (1.19, 8.87) | 0.01 |
| Pneumonia | 9 (30) | 10 (32.2) | 3 (9.6) | 3.1 (0.92, 10.3) | 0.06 | 3.33 (1.01, 10.9) | 0.02 |
| Use of supplementary oxygen | 6 (20) | 2 (6.4) | 1 (3.2) | 6.2 (0.79, 48.4) | 0.10 | 2.0 (0.19, 20.9) | 0.61 |
| Negative test on day 11a | 21 (87.5) | 27 (90) | 30 (96.8) | 0.90 (0.76-1.06) | 0.30 | 0.93 (0.81-1.06) | 0.354 |
aData were missing for seven patients in the group with HCQ+AZT.
NC: not calculable; HCQ: hydroxychloroquine; AZT: azithromycin; RR: relative risk; CI: confidence interval.
Secondary outcomes
The incidence of disease progression was 30% (9/30) in the HCQ + AZT group, 41.9% (13/31) in the HCQ group, and 12.9% (4/31) in the placebo group. The RR for the HCQ + AZT group versus placebo was 2.32 (95% CI, 0.80-6.74; p = 0.10), figure 2, and the RR for the HCQ group versus placebo was 3.25 (95% CI, 1.19-8.87; p = 0.01). Even though there was a statistically significant risk for developing pneumonia in the HCQ group compared to the placebo group (RR = 3.33 [CI 95% 1.10, 10.9; p = 0.02]), the pneumonia incidence was 30% (9/30) in the HCQ + AZT group, 32.2% (10/31) in the HCQ group and 9.6% (3/31) in the placebo group. The fixed combination of HCQ + AZT did not benefit compared to placebo. The frequency of patients who required supplemental oxygen was 20% (6/30) in the HCQ+ AZT group, 6.4% (2/31) in the HCQ group, and 3.2% (1/31) in the placebo group. There were no significant differences between the groups. There was no statistical difference between groups for the negative test (PCR) on day 11. Treatment adherence was > 90%, with no differences between treatment arms.
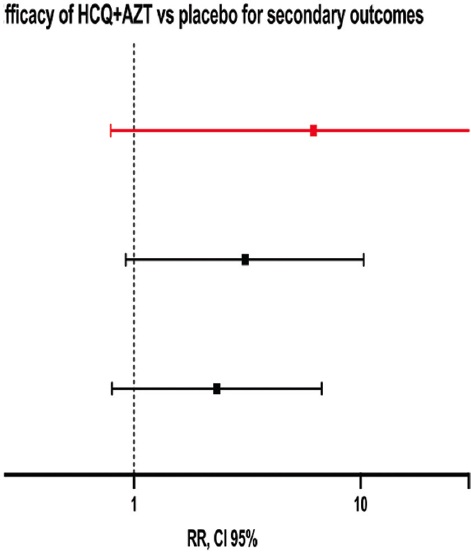
Table 3 shows the efficacy of a placebo for secondary outcomes. For the group receiving placebo, we found disease progression in 12.9% (4/31) of participants compared to the group receiving active drugs (HCQ + AZT, HCQ) in 36.1% (22/61), (RR of 0.35 [0.13, 0.94; p = 0.02]). When analyzing pneumonia development, the results showed an incidence of 9.6% (3/31) compared to an incidence of 31% (19/61) in the group with HCQ + AZT, HCQ, (RR of 0.31 [0.09, 0.96, p = 0.02]). We could not observe differences in the use of supplemental oxygen.
Table 3 Efficacy of placebo versus active treatment for primary and secondary outcomes
| Outcomes | Placebo n = 31 (%) | Active treatment n = 61 (%) | RR | p |
|---|---|---|---|---|
| Secondary | ||||
| Progression | 4 (12.9) | 22 (36.1) | 0.35 (0.13, 0.94) | 0.02 |
| Pneumonia | 3 (9.6) | 19 (31) | 0.31 (0.09, 0.96) | 0.02 |
| Use of supplementary oxygen | 1 (3.2) | 8 (13.1) | 0.24 (0.03, 1.87) | 0.13 |
RR: relative risk; p: exact Fishers test.
Table 4 shows the risk associated with pneumonia. In the univariate analysis, HCQ administration was associated with an increased risk of pneumonia. In the multivariate analysis, HCQ and age were associated with a higher risk of pneumonia.
Table 4 Risk associated with pneumonia, logistic regression analysis
| Step | Variable | b | SE | OR | 95% IC | p |
|---|---|---|---|---|---|---|
| Step 1 | HCQ | 1.49 | 0.71 | 4.44 | (1.08, 18.1) | 0.03 |
| HCQ+AZT | 1.38 | 0.72 | 4.00 | (0.96, 16.6) | 0.06 | |
| Placebo | Reference | |||||
| R2 = 0.093 | ||||||
| Step 2 | HCQ | 1.55 | 0.76 | 4.72 | (1.06, 20.9) | 0.04 |
| HCQ+AZT | 1.37 | 0.76 | 3.93 | (0.88, 17.5) | 0.07 | |
| Placebo | Reference | |||||
| Age (years) | 0.05 | 0.02 | 1.05 | (1.01, 1.09) | 0.007 | |
| Comorbidities | 0.12 | 0.58 | 1.13 | (0.36, 3.56) | 0.831 | |
| R2 = 0.212 | ||||||
B: beta exponent; OR: odds ratio; SE: standard error; HCQ+AZT: hydroxychloroquine with azithromycin; HCQ: hydroxychloroquine.
Adverse events
The most frequent adverse events were gastrointestinal symptoms with a rate of 16.6%, bradycardia with a rate of 6.4%, platelet elevation with a rate of 4.3%, and hypertriglyceridemia with a rate of 3.8%. Adverse events occurred with similar frequency between the different treatment groups. The analysis of whether there were differences in the QTc interval by the treatment group showed no differences in those who received HCQ + AZT or HCQ compared to the placebo group (Table 5).
Table 5 Adverse events according to treatment group
| Adverse event | Total 559 | HCQ + AZT 177 | HCQ 213 | Placebo 169 | p |
|---|---|---|---|---|---|
| Duration of the QTc segment (ms) at the end of the follow-upa | 416 (390-434) | 413 (387-439) | 421 (396-430) | 413 (384-435) | 0.903 |
| Gastrointestinal, n (%) | 93 (16.6) | 33 (18.6) | 36 (16.9) | 24 (14.2) | 0.269 |
| Urticaria, n (%) | 5 (0.9) | 0 (0) | 4 (1.9) | 1 (0.6) | 0.541 |
| Dizziness, n (%) | 14 (2.5) | 3 (1.7) | 5 (2.3) | 6 (3.6) | 0.271 |
| Hypoglicemia, n (%) | 12 (2.1) | 3 (1.7) | 4 (1.9) | 5 (3.0) | 0.421 |
| Thrombocytosis, n (%) | 24 (4.3) | 6 (3.4) | 9 (4.2) | 9 (5.3) | 0.376 |
| Hypertriglyceridemia, n (%) | 21 (3.8) | 5 (2.8) | 8 (3.8) | 8 (4.7) | 0.508 |
| Bradycardia, n (%) | 36 (6.4) | 13 (7.3) | 11 (5.2) | 12 (7.1) | 0.916 |
| Others, n (%) | 349 (62.4) | 111 (62.4) | 134 (62.9) | 104 (61.5) | 0.573 |
aMedian, interquartile range, Kruskal-Wallis test.
HCQ: hydroxychloroquine; AZT: azithromycin.
Discussion
At the beginning of the pandemic, the fixed combination of HCQ + AZT was proposed as a possible therapeutic option based on its antiviral and anti-inflammatory activity in vitro. However, clinical studies yielded inconsistent results. Therefore, this research project was conducted18.
The study population consisted of participants with mild COVID-19 who had a low risk of complications. Of whom, only 2% required hospitalization19.
The results of this study suggest that the fixed combination of HCQ + AZT for the treatment of patients with mild COVID-19 does not reduce the risk of hospitalization compared to the use of HCQ alone or placebo. These results coincide with those reported in a Brazilian clinical trial on patients with mild and moderate COVID-19, which showed no significant differences for any of the treatment groups in terms of hospitalization or mechanical ventilation20. These results also coincide with those reported by other authors who evaluated the separate use of HCQ or AZT and found no benefit to reduce the risk of hospitalization, mechanical ventilation, or mortality11,21-25.
The analysis of the secondary outcomes revealed that the administration of HCQ increased the risk of progression and pneumonia compared to placebo. However, for the combination of HCQ + AZT, the results showed only a trend in the risk for pneumonia, with no statistical significance, due to a lack of statistical power.
The increase in the risk of damage after the use of the combination of HCQ + AZT, as in this study, was also reported by Kuderer et al., who found a higher risk of mortality in patients who received this combination treatment, even in the multivariate model. However, these results were derived from an observational study where it was possible that the patients who received the use of HCQ + AZT had a more severe form of the disease at baseline, whereas in the present study, the participants included in the three treatment groups had mild symptoms26.
Our results on the lack of benefit for the different outcomes of the study contrast with the results reported by Gautret et al., who highlighted the efficacy of the combination of HCQ + AZT for viral clearance on day 6 of treatment. In this study, no significant differences were found in the negativization of the PCR at day 11. It is possible to attribute the differences to the design of the study, non-randomization, the evaluation of an intermediate regulator as an outcome, and not evaluating other clinically relevant outcomes, such as mechanical ventilation or mortality27.
Although an antiviral effect against SARS-CoV-2 was found for HCQ and AZT in vitro, the use of HCQ in this study conditioned a higher risk of progression and pneumonia. This paradoxical response suggests that the drug could impair the immune response, conditioning a delay in the cellular and adaptive immune response, as shown by Roques et al.27 analyzing the effect of chloroquine on Chikungunya virus infection, who highlighted the contrast between the in vitro antiviral effect of chloroquine and the exacerbation of the disease in vivo and who reported that they are like the results reported by Maisonnasse, as well as our results27,28.
Another concern about the use of HCQ + AZT for the treatment of COVID-19 infection is the risk of cardiovascular complications by prolonging QT interval30. In this study, no differences in QT segment duration or fatal arrhythmias were documented in the three treatment groups, suggesting that significant cardiac involvement and arrhythmias in patients infected with COVID-19 have a multifactorial etiology and are more common in patients with severe forms of the disease, comorbidities, and advanced age.
The most frequent adverse events were mild and gastrointestinal symptoms, characterized by nausea, vomiting, pain, and abdominal distension. The sample size calculation was 105 participants. However, the study was stopped after the inclusion of 92 participants due to a decrease in the number of patients in Mexico before the third pandemic wave. Participants who received ivermectin as concomitant treatment were included. However, there were no differences between the treatment arms.
Conclusions
The results of this study add information regarding the raised concern about the safety of HCQ and demonstrate that the fixed combination of HCQ + AZT is not useful in preventing hospitalization and disease progression. The use of HCQ and HCQ + AZT was associated with an increased risk of disease progression. The adverse events observed were mild and infrequent, predominantly consisting of gastrointestinal symptoms.

