











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Mediastinal lymph node enlargement is a critical computed tomography (CT) finding that can range from benign to malignant in patients with respiratory complaints and may require further examination. Since the presence of mediastinal lymphadenopathy (MLAP) is related to the severity of the disease in post-COVID patients who have had and recovered from severe COVID-19 infection, the presence of MLAP should be carefully examined in subsequent examinations, even in patients without lung involvement on admission CT1. The detection of MLAP in patients with idiopathic pulmonary fibrosis (IPF) is thought to be a result of high-grade chronic inflammation, and a correlation between the severity of IPF disease and MLAP has been shown in the literature2.
When the current literature on MLAP and COVID-19 were examined, studies were conducted in the acute and active period of COVID-19 pneumonia. However, in our study, MLAP in the controls was performed 6-12 months after the patients had COVID-19 pneumonia. After suffering severe COVID-19 pneumonia, the mediastinal lymph nodes begin to enlarge during acute inflammation, which is considered a poor-prognosis marker at that time. After 6 months, this turns into chronic inflammation, and MLAP occurs. It is thought that there may be a correlation between the severity of chronic inflammation and mediastinal lymph node enlargement in patients with severe COVID-19 pneumonia, just as in IPF.
MLAP can be caused by infectious or non-infectious causes and is defined as a measurement of the lymph node short axis ≥ 10 mm. SUVmax value ≥ 2.5 was defined as pathological MLAP3. The most common atypical CT features of COVID-19 pneumonia are MLAP, linear opacities, tree bud sign, interlobular and intralobular septal thickening, cavitation, and pleural effusion4. MLAP is frequently associated with benign diseases such as heart failure, sarcoidosis, and diseases accompanying malignant diseases. Although MLAP is not the typical chest finding in COVID-19 pneumonia, it is associated with the prognosis of COVID-19 patients. The mortality rate in hospitalized COVID-19 patients with MLAP was found to be higher than in those without MLAP, and it has been reported in the literature that it should be investigated as a prognostic factor for severe disease. The literature shows a correlation between the severity of IPF disease and the presence of MLAP, suggesting that MLAP results from severe chronic inflammation in these patients1,5,6.
For MLAP, the size and number of lymph nodes are essential for surgical treatment and follow-up. MLAP, usually over 2 cm in size, should be closely monitored regardless of the cause6. The radiological findings of one of our patients are shown in figure 1.
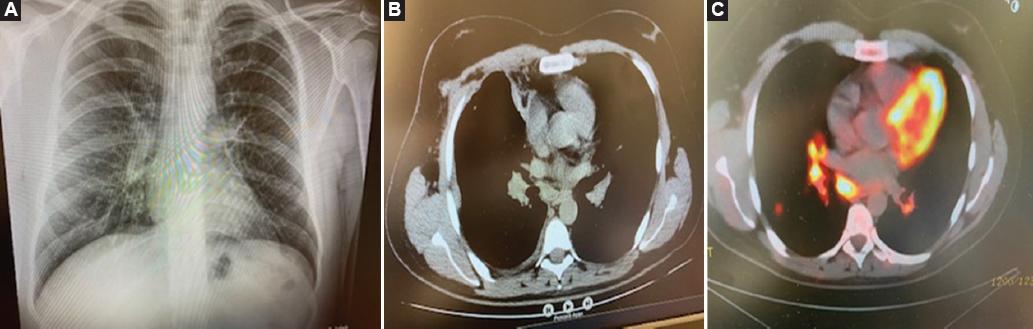
Figure 1 A view from the chest radiograph of the patients*. A: a section with Hilar fullness from the chest X-ray findings of the patients. B: a section from the mediastinal window view with mediastinal lymphadenopathy. C: a section with positive fluorodeoxyglucose from positron emission tomography-computed tomography findings. *It was taken from the hospital file archives of the patients in our study, and their permission was obtained.
COVID-19 is a respiratory disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. In this study, we aimed to determine whether MLAP, which was detected in patients with severe COVID-19 pneumonia in the controls at least 6 months after the disease (post-COVID-19 period), was related to having the disease. If the detected MLAP formation is determined to be secondary to COVID-19 pneumonia, then immediate referral to the surgery clinic for further examination may be unnecessary. At the same time, by closely monitoring the patients in whom we detect MLAP, we can protect them from surgical complications and not be late in making the diagnosis.
Methods
This study was approved by the Ethical Committee of the University of Health Sciences Şişli Hamidiye Etfal Training and Research Hospital. Ethics Committee approval was granted by our institution on September 06, 2022, protocol number 2137. It was conducted according to the Declaration of Helsinki and Good Clinical Practice. The authors have obtained the approval of the Ethics Committee for the analysis and publication of clinical data obtained routinely. The informed consent of the patients was not required because it was a retrospective observational study. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Study population and data collection
Our study was a single-center, retrospective, casecontrol study. Our study analyzed the data of 140 patients who applied to our hospitals Şişli Hamidiye Etfal Training and Research Hospital Chest Diseases Outpatient Clinic between January 01, 2022, and August 01, 2022, and were reviewed retrospectively. During etiological investigations, individuals over 18 years old, regardless of gender, who applied to our hospitals chest diseases outpatient clinics with the MLAP, who had not been diagnosed with lymphoma and sarcoidosis, immunodeficiency, cancer, tuberculosis, asthma, chronic obstructive pulmonary disease, and had no previous mediastinal pathology. Patients with MLAP detected in thorax CT examinations were included in the study. Patients with lung and other malignancies, under 18 years of age, pregnant women, and patients who had image artifacts on their CT scans were excluded from the study. A total of 140 cases who were followed up in our clinic and diagnosed with chest MLAP by CT were included in the study. These cases were divided into two categories: 83 cases with COVID-19 who had COVID-19 pneumonia and recovered, and 57 cases without COVID-19. The two categories were compared using data obtained from demographic characteristics, clinical findings, reverse transcription-polymerase chain reaction (RT-PCR) results, chest radiography findings, thorax CT findings, positron emission tomography (PET)-CT findings, histopathological results, and treatment approaches. Data were collected from the hospital automation system and analyzed with Statistical Package for the Social Sciences (SPSS) 24.
Sample size
The sample of the study was determined as a total of 140 patients, at least 51 in both groups, with an effect size of 0.40, a = 0.05, and power (1-b) = 0.85, using the G-power program. There were two groups: 57 patients without covid-19 and 83 patients with RT-PCR (+)
Image analysis
Demographic information, clinical findings, comorbidities, thorax CT, and PET-CT images were obtained from hospital computer records and Picture Archiving and Communication System. RT-PCR testing was performed using nasopharyngeal or oropharyngeal swabs using the Biospeedy SARS-CoV-2 Dual Gene RT-qPCR Kit (Bioeksen). Chest CT scans were performed with patients in the supine position, during last inspiration, and without intravenous contrast administration. The protocol included a peak voltage of 100 kV and an effective milliampere-second setting of 20 mA-s, resulting in unenhanced chest CT scans. These scans used a 512 × 512 pixel image matrix with 2 mm thin sections taken in the axial plane.
In this study, adjustments were applied to the mediastinal windows (width: 400 HU; level: 100 HU) and lung windows (width: 1500 HU; level: -500 HU). Tomography findings were evaluated by two experienced radiologists who agreed on the CO-RADS value. In routine axial CT images, the short axis of the mediastinal lymph node was measured, and if the short axis was 10 mm or more, it was considered MLAP. When the SUVmax value was ≥ 2.5 in the PET-CT examination of patients diagnosed with MLAP, fluorodeoxyglucose (FDG) uptake was considered pathological and was called "FDG positive".
Statistical analysis
Patient data collected within the scope of the study were analyzed with the IBM SPSS for Windows 23.0 (IBM Corp., Armonk, NY) package program. Frequency and percentage were given for categorical data, and median, minimum, and maximum descriptive values for continuous data. The normality test of the data was conducted with the Kolmogorov-Smirnov Test. In the comparisons between the groups, the "Independent Sample T-Test" was used for those with normal distribution for the two groups, the "Mann-Whitney U Test" for those who did not show normal distribution, and the "Fisher's Exact Test or Chi-Square Test" was used for the comparison of categorical variables. Logistic regression analysis was used to examine the risk factors affecting the SUVmax value of ± 2.5. The results were considered statistically significant when p < 0.05.
Results
A total of 140 patients, 38.6% (n = 54) female and 61.4% (n = 86) male, were included in the evaluation. 40.7% (n = 57) of the patients were diagnosed without COVID-19, and 59.3% (n = 83) had positive RT-PCR test results, and it was determined that they had COVID-19. The distribution of demographic characteristics of all patients according to MLAP (lymph node short axis, SUVmax value) is shown in table 1. When table 1 was examined, no statistically significant difference was detected between demographic characteristics and mediastinal lymph node short axis and SUVmax values p > 0.05).
Table 1 Distribution of demographic characteristics of all patients according to MLPA (lymph node short axis, SUVmax value)
| Characteristics | Lymph node short axis | p | SUVmax | p | ||||
|---|---|---|---|---|---|---|---|---|
| 10-20 (n = 103) | 21-30 (n = 27) | > 30 (n = 10) | < 2.5 (n = 22) | 2.5-5.0 (n = 51) | > 5.0 (n = 49) | |||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Age (years) | 0.553 | 0.432 | ||||||
| 18-64 | 62 (60.2) | 19 (70.4) | 7 (70) | 16 (72.7) | 33 (64.7) | 28 (57.1) | ||
| 65-94 | 41 (39.8) | 8 (29.6) | 3 (30) | 6 (27.3) | 18 (35.3) | 21 (42.9) | ||
| Gender | 0.696 | 0.428 | ||||||
| Male | 64 (62.1) | 15 (55.6) | 7 (70) | 16 (72.7) | 29 (56.9) | 29 (59.2) | ||
| Female | 39 (37.9) | 12 (44.4) | 3 (30) | 6 (27.3) | 22 (43.1) | 20 (40.8) | ||
| Smoking status | 0.988 | 0.276 | ||||||
| Smoker | 44 (42.7) | 13 (48.1) | 4 (40) | 13 (59.1) | 22 (43.1) | 20 (40.8) | ||
| Non-smoker | 38 (36.9) | 9 (33.3) | 4 (40) | 8 (36.4) | 21 (41.2) | 17 (34.7) | ||
| Ex-smoker | 21 (20.4) | 5 (18.5) | 2 (20) | 1 (4.5) | 8 (15.7) | 12 (24.5) | ||
| Symptoms | 0.058 | 0.275 | ||||||
| Dyspnea | 17 (16.5) | 1 (3.7) | 5 (50) | 4 (18.2) | 5 (9.8) | 12 (24.5) | ||
| Chest pain | 14 (13.6) | 5 (18.5) | 1 (10) | 1 (4.5) | 9 (17.6) | 7 (14.3) | ||
| Cough | 61 (59.2) | 17 (63) | 4 (40) | 13 (59.1) | 33 (64.7) | 26 (53.1) | ||
| Back pain | 11 (10.7) | 4 (14.8) | 0 (0) | 4 (18.2) | 4 (7.8) | 4 (8.2) | ||
| Concomitant disease | 0.118 | 0.950 | ||||||
| Asthma | 36 (38.7) | 4 (15.4) | 2 (20) | 5 (27.8) | 13 (26) | 15 (34.1) | ||
| DM | 7 (7.5) | 3 (11.5) | 0 (0) | 1 (5.6) | 5 (10) | 2 (4.5) | ||
| GIS | 5 (5.4) | 3 (11.5) | 2 (20) | 2 (11.1) | 6 (12) | 2 (4.5) | ||
| HT | 13 (14) | 4 (15.4) | 1 (10) | 3 (16.7) | 7 (14) | 8 (18.2) | ||
| HD | 6 (6.5) | 2 (7.7) | 3 (30) | 2 (11.1) | 5 (10) | 3 (6.8) | ||
| COPD | 26 (28) | 10 (38.5) | 2 (20) | 5 (27.8) | 14 (28) | 14 (31.8) | ||
DM: diabetes mellitus; GISD: gastrointestinal system diseases; HT: hypertension; COPD: chronic obstructive pulmonary disease; HD: heart disease; MLAP: mediastinal lymphadenopathy.
The distribution of demographic characteristics of the patients with COVİD-19 and without COVID-19 is denoted in table 2. When the table was examined, there was only a statistically significant difference between the two groups regarding age (p < 0.05).
Table 2 Distribution of demographic characteristics of patients with COVİD-19 and without COVİD-19
| Characteristics | Total (n = 140) | without COVID-19 (n = 57) | with COVID-19 (n = 83) | p |
|---|---|---|---|---|
| n (%) or Median (Min-Max) | n (%) or Median (Min-Max) | n (%) or Median (Min-Max) | ||
| Age (years) | 61 (20-94) | 55 (22-78) | 62 (20-94) | 0.006 |
| Gender | 0.477 | |||
| Male | 86 (61.4) | 33 (57.9) | 53 (63.9) | |
| Female | 54 (38.6) | 24 (42.1) | 30 (36.1) | |
| Smoking status | 0.115 | |||
| Smoker | 61 (43.6) | 25 (43.9) | 36 (43.4) | |
| Non-smoker | 51 (36.4) | 25 (43.9) | 26 (31.3) | |
| Exsmoker | 28 (20) | 7 (12.3) | 21 (25.3) | |
| Symptoms | 0.656 | |||
| Dyspnea | 23 (16.4) | 8 (14) | 15 (18.1) | |
| Chest pain | 20 (14.3) | 7 (12.3) | 13 (15.7) | |
| Cough | 82 (58.6) | 34 (59.6) | 48 (57.8) | |
| Back pain | 15 (10.7) | 8 (14) | 7 (8.4) | |
| Concomitant disease | 129 (92.1) | 50 (87.7) | 79 (95.2) | 0.122 |
| Asthma | 42 (32.6) | 19 (38) | 23 (29.1) | |
| DM | 10 (7.8) | 5 (10) | 5 (6.3) | |
| GIS | 10 (7.8) | 4 (8) | 6 (7.6) | |
| HT | 18 (14) | 8 (16) | 10 (12.7) | |
| HD | 11 (8.5) | 2 (4) | 9 (11.4) | |
| COPD | 38 (29.5) | 12 (24) | 26 (32.9) |
DM: diabetes mellitus; GISD: gastrointestinal system diseases; HT: hypertension; COPD: chronic obstructive pulmonary disease; HD: heart disease.
Significant differences were observed between the two groups in all clinical findings (p < 0.05) (Table 3). Peripheral lymphadenopathy was in the intra-abdominal region in 24.1% (n = 20) of RT-PCR-positive with COVİD-19 patients and 3.5% (n = 2) of those without COVİD-19 patients (p < 0.001). Mediastinal width and lymph node size were higher in COVİD-19 patients than in non-COVID-19 patients (p = 0.008; p < 0.001). The pathology result of the majority of COVID-positive patients with COVİD-19 was benign (65%), whereas this rate was 22.8% in patients without COVİD-19 (p < 0.001). As a result, 77.2% of the patients without COVİD-19 PCR results regressed in the follow-up, whereas this rate was 24.1% in the patients with COVİD-19 (p < 0.001).
Table 3 Distribution of clinical characteristics of patients with COVİD-19 and without COVİD-19
| Characteristics | Total (n = 140) | Without COVID-19 (n = 57) | With COVID-19 (n = 83) | p |
|---|---|---|---|---|
| n (%) or Median (Min-Max) | n (%) or Median (Min-Max) | n (%) or Median (Min-Max) | ||
| Peripheric LAP | < 0.001 | |||
| None | 55 (39.3) | 35 (61.4) | 20 (24.1) | < 0.001 |
| Cervical | 43 (30.7) | 15 (26.3) | 28 (33.7) | 0.454 |
| Intraabdominal | 22 (15.7) | 2 (3.5) | 20 (24.1) | < 0.001 |
| Pelvic | 4 (2.9) | 1 (1.8) | 3 (3.6) | 0.646 |
| Diffuse | 16 (11.4) | 4 (7) | 12 (14.5) | 0.276 |
| Chest X-ray | 0.002 | |||
| Normal | 78 (55.7) | 42 (73.7) | 36 (43.4) | < 0.001 |
| Enlarged mediastinum | 50 (35.7) | 13 (22.8) | 37 (44.6) | 0.008 |
| Hilar fulness | 12 (8.6) | 2 (3.5) | 10 (12) | 0.122 |
| Computerize tomografi | 0.024 | |||
| M2R right upper paratracheal | 39 (27.9) | 14 (24.6) | 25 (30.1) | 0.597 |
| M3 prevascular | 20 (14.3) | 12 (21.1) | 8 (9.6) | 0.099 |
| M4R right lower paratracheal | 39 (27.9) | 21 (36.8) | 18 (21.7) | 0.049 |
| M4L lower left paratracheal | 14 (10) | 3 (5.3) | 11 (13.3) | 0.207 |
| M7 subcarinal | 28 (20) | 7 (12.3) | 21 (25.3) | 0.093 |
| Lymph node size (mm) | 17 (10-51) | 15 (10-44) | 18 (10-51) | < 0.001 |
| SUVmax | < 0.001 | |||
| FDG (-) | 18 (12.9) | 15 (26.3) | 3 (3.6) | < 0.001 |
| < 2.5 | 22 (15.7) | 18 (31.6) | 4 (4.8) | < 0.001 |
| 2.5-5.0 | 51 (36.4) | 15 (26.3) | 36 (43.4) | 0.039 |
| > 5.0 | 49 (35) | 9 (15.8) | 40 (48.2) | < 0.001 |
| Pathology | < 0.001 | |||
| None | 57 (40.7) | 40 (70.2) | 17 (20.5) | < 0.001 |
| Benign | 67 (47.9) | 13 (22.8) | 54 (65.1) | < 0.001 |
| Malign | 16 (11.4) | 4 (7) | 12 (14.5) | 0.276 |
| Pathology result | < 0.001 | |||
| Granulomatous lymphadenitis (benign) | 20 (14.3) | 4 (7) | 16 (19.3) | 0.073 |
| Regressed at follow-up (benign) | 64 (45.7) | 44 (77.2) | 20 (24.1) | < 0.001 |
| Reactive lymph node (benign) | 37 (26.4) | 5 (8.8) | 32 (38.6) | < 0.001 |
| Anthracosis (benign) | 3 (2.1) | 0 (0) | 3 (3.6) | 0.271 |
| Cancer metastasis (malignant) | 16 (11.4) | 4 (7) | 12 (14.5) | 0.276 |
LAP: lymphadenopathy; FDG: fluorodeoxyglucose.
Table 4 elaborates on the logistic regression analysis results, examining the factors causing the SUVmax value to be ≥ 2.5 in the patients included in the study. COVİD-19 patients caused a 15-fold SUVmax value of ≥ 2.5. In addition, peripheral lymphadenopathy caused a 3.9-fold SUVmax value of ≥ 2.5, abnormal chest X-rays caused a 9.3-fold SUVmax value of ≥ 2.5, and abnormal pathology results led to a 33.9-fold SUVmax value of ≥ 2.5.
Table 4 Laboratory parameters affecting SUVmax≥ 2.5
| Characteristics | Univariant | Multivariant | ||
|---|---|---|---|---|
| Odds ratio (95% CI) | p | Odds ratio (95% CI) | p | |
| Age | 1.013 (0.990-1.037) | 0.271 | ||
| Gender | ||||
| Male | Reference | - | ||
| Female | 1.690 (0.771-3.702) | 0.190 | ||
| RT-PCR | ||||
| Negative | Reference | - | Reference | - |
| Positive | 15.000 (5.856-38.058) | < 0.001 | 5.964 (1.937-18.370) | 0.002 |
| Peripheric LAP | ||||
| No | Reference | - | Reference | - |
| Yes | 3.890 (1.801-8.398) | < 0.001 | 1.451 (0.491-4.289) | 0.500 |
| Chest X-Ray | ||||
| Normal | Reference | - | Reference | - |
| Abnormal | 9.280 (3.355-25.662) | < 0.001 | 2.777 (0.758-10.165) | 0.123 |
| Pathology | Reference | - | Reference | - |
| Normal | 33.857 | < 0.001 | 13.452 | < 0.001 |
| Abnormal | (10.833-105.818) | (3.864-46.831) | ||
RT-PCR: reverse transcription-polymerase chain reaction; LAP: lymphadenopathy.
The statistically significant variables in the univariate model were re-evaluated in the multivariate model. RT-PCR positivity with COVİD-19 and abnormal pathology findings were statistically significant. Accordingly, it was determined that positive RT-PCR test results with COVİD-19 were 5.9 times higher than without COVİD-19 outcomes, and abnormal pathology results were found to be 13.4 times more frequently in SUVmax value being ≥ 2.5 compared to normal samples.
Discussion
In the study, MLAP was detected in the 6-month follow-up of patients with severe COVID-19, and the aim was to evaluate the relationship between these MLAP SUVmax values and having COVID-19 disease. While the frequency of MLAP in patients with COVID-19 pneumonia is 0-66% in the literature, the frequency of MLAP in this study (965 patients with COVID-19 pneumonia were scanned, and MLAP was detected in 83 and included in the study) was found to be 11.6%, similar to the literature1,6,7.
Thorax tomography and PET-CT scans were performed on our patients who applied to us with respiratory complaints at least 6 months to 1 year after COVID-19, that is, during the post-COVID-19 patient controls. Diagnostic PET-CT was performed in patients with MLAP detected in thorax CT examination. In addition, we evaluated that MLAP size (SUVmax value) and FDG uptake are not associated with malignancy in patients with severe COVID-19, but may be associated with the severity of chronic inflammation.
Our results showed that mediastinal width and lymph node size were higher in patients with COVID-19 than in those without COVID-19. The pathology result of most COVID-19-positive patients was benign (65%), whereas this rate was 22.8% in patients without COVID-19. As a result, 77.2% of the patients without COVID-19 regressed in the follow-up, whereas this rate was 24.1% in the patients with COVID-19.
COVID-19-positive patients included in the study increased the incidence of MLAP ≥ 2.5 above the SUVmax value 15 times more than those without COVID-19. In addition, detecting peripheral lymphadenopathy in PET-CT increased the incidence of ≥ 2.5 times above the SUVmax value, 3.9 times more. Abnormal chest X-rays of the patients increased the incidence of ≥ 2.5 above the SUVmax value 9.3 times, and abnormal pathology results increased the incidence of ≥ 2.5 above the SUVmax value 33.9 times.
In our study, the chest X-ray findings of the patients without COVID-19 were mostly expected. In contrast, the chest X-ray of the patients with COVID-19-positive patients was found to be more abnormal, resulting in mediastinal enlargement and hilar lymphadenopathies8-10. The most common thorax CT finding detected in our study was M4R right lower paratracheal lymph node enlargement. Pulmonary parenchyma findings were deficient, and sequelae were reported as changes11.
Regarding the results of our study, the presence of aggravated COVID-19 is linked with the occurrence of MLAP. COVID-19-positive patients and abnormal pathology results have indicated higher SUVmax values, thus the presence of lymphadenopathy. To date, MLAP has been observed widely in COVID-19 (0-66%). However, it should be emphasized that not all lymphadenopathies are located in the mediastinal region. In published case reports, two cases (both female) are reported to have MLAP at the initial and repeated CT scan on the 6th day (1/6/10R and 2R/4R/4L)12,13.
However, there are controversial data on this subject. Bayramoglu et al. indicated the presence of MLAP as 0-8.1% in their retrospective analysis14. In another retrospective research, no MLAP was found during pregnancy15. Grassi et al. found the incidence of MLAP as 1.3% in a cohort of 80 patients from Italy16. In two different studies (n = 418 and n = 134), the rate of MLAP was reported as 18.2% and 54.8%16-18. Fang et al. did not detect any association between MLAP and gender, age, cancer history, intensive care unit (ICU) admission, length of hospital stays, and laboratory parameters, but with cobblestone imaging findings19. In a French study, Valette et al. published that MLAP existed in six of nine individuals with severe COVID-19 in the ICU20. Studies from Chinese patients indicated the presence of MLAP at 43.5%, 41.7%, and 19.8%18,19,21.
Kaya and Akman investigated the relationship between MLAP and ICU hospitalization and mortality in COVID-19 patients and found a statistical significance between the three parameters6. They claimed that the more severe findings on CT scans predict the prognosis. In addition, they stated that increased bronchial wall thickness was more common in patients with MLAP. The mortality rate was higher in patients with MLAP1.
In another study, Satici et al.22 reported that mediastinal lymphadenopathies were detected more in elderly patients with comorbid diseases and were significantly associated with mortality. The rate of MLAP was 9.2% in the whole study population but 19.65% in deceased individuals21. Both studies declared that the presence of MLAP led to increased mortality. Similar to our findings, mediastinal lymph node involvement has been an essential factor in COVID-19.
In the study of Bhatti et al.,23 MLAP was detected in 131 (62.4%) of 210 patients included in the study. Covid-19 patients with MLAP had a higher mean and median severity score than those without MLAP. This study documents the high prevalence of MLAP in hospitalized COVID-19 patients and shows that the severity score, which represents the more severe course of the disease, is higher22.
Limitations of our study
Since our study was retrospective, some laboratory findings and respiratory function findings could not be obtained. In this regard, a study can be organized to investigate the laboratory findings showing the severity of chronic inflammation in patients with severe COVID-19 pneumonia, respiratory functional characteristics, and the relationship between radiological imaging and MLAP features. Although this study is a retrospective observational study and provides valuable information about the potential etiology of the disease, it typically cannot definitively determine causality.
Conclusions
This study showed that severe COVID-19 and mediastinal lymph node involvement (SUVmax: 3-5) were associated regardless of age, gender, comorbidities, and disease outcomes. Establishing reliable SUVMAX values in severe post-COVID-19 patients will help guide clinical decisions, adapt therapeutic approaches, and avoid unnecessary surgical interventions for patients with MLAP who require surgical diagnosis and treatment, and will help these patients avoid surgery complications.

